OSHE 5335 ERGONOMICS METHODS ANALYSIS TECHNIQUES EXAMPLE OF











 • Electromyography (EMG) • Nerve Conduction Study • Radiology")
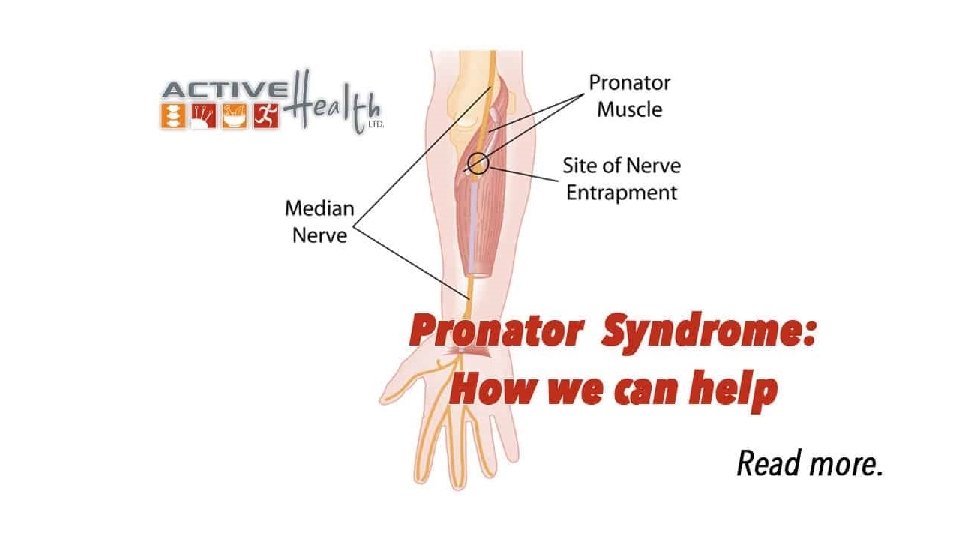
 • Compression neuropathy of the median nerve at the")
 • Placing pressure over the pronator muscle on both")



 • Surgical • Considered when conservation treatment fails • Indicated if patient")




 • Carpenters: Bio. Curve Hammers • Features a patented 19 -degree")
 • Weightlifter: Elbow Sleeves/Braces • Compression & support for weightlifting, Cross.")




 • Marine Dididze & Andrew I. Sherman (2020). Stat. Pearls Publishing: Pronator")
- Slides: 40
OSHE 5335 ERGONOMICS METHODS & ANALYSIS TECHNIQUES EXAMPLE OF CTD: PRONATOR ULNAR SYNDROME
TABLE OF CONTENTS • ABSTRACT • DESCRIPTION • CAUSES • SYMPTOMS • DIAGNOSIS • TREATMENT • ERGONOMIC SOLUTIONS (HOW TO FIX IT) • CONCLUSION • REFERENCES
ABSTRACT • The purpose of this presentation is to provide a comprehensive and informative overview of the pronator ulnar syndrome which may help make a fundamental difference between other types of compression syndromes such as: flexor-pronator mass syndrome, CTS, etc. • In the following slides, we will be talking about the description, causes, symptoms, diagnosis, treatment, and ergonomic solution.
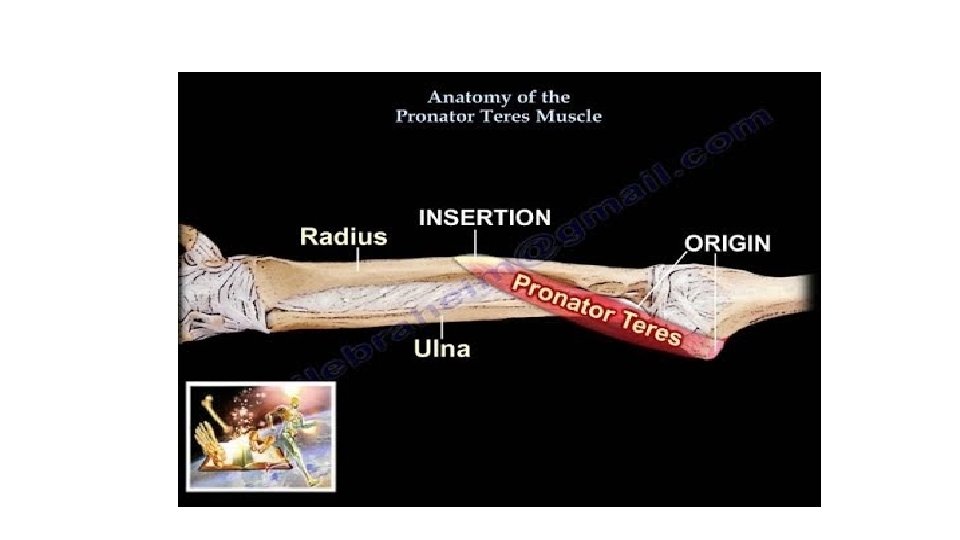
HISTORY • Was first described by Seyfferth in 1951. • It was originally thought that the median nerve was compressed between the 2 heads of the pronator teres. • Since Seyfferth’s original description, PS has been expanded to encompass compression of the median nerve at the ligament of Struthers, lacertus fibrous, pronator teres, etc.
EPIDEMIOLOGY • Rare condition that may be easily overlooked & mistaken for a more frequent carpal tunnel syndrome. • No age group preference has been described, but one study reports a higher prevalence of pronator teres syndrome in men.
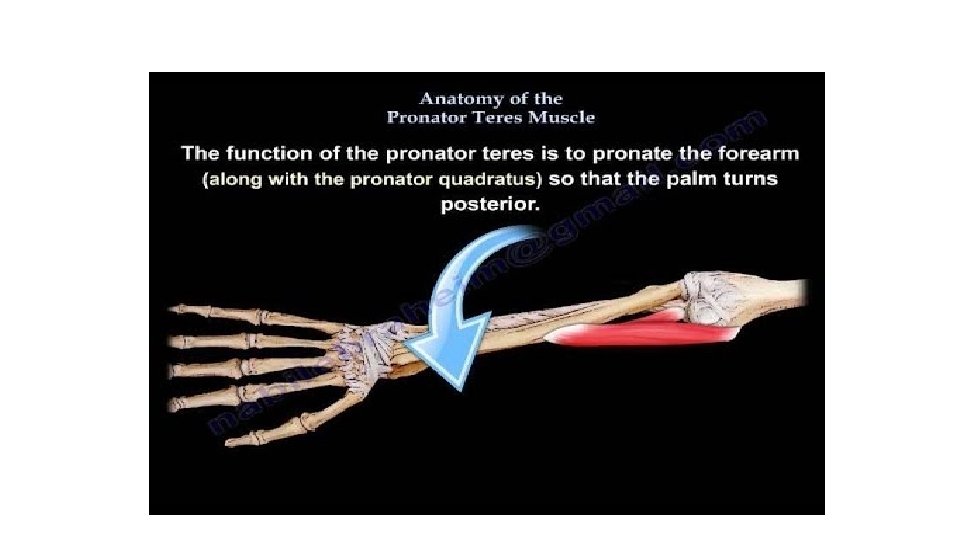
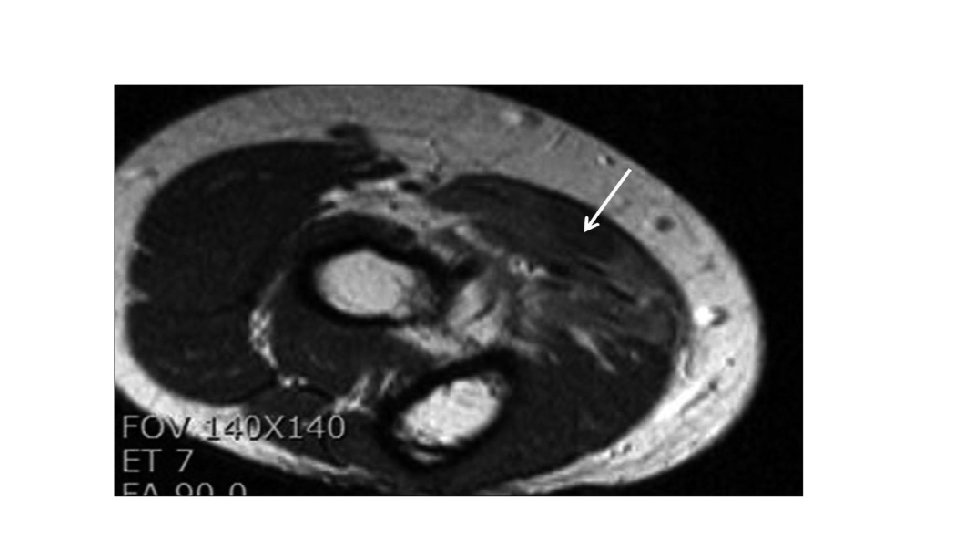
DESCRIPTION • Entrapment of the median nerve in the proximal forearm. • Repetitive strain injury among athletes, carpenters, mechanics, and writers, possibly due to overuse of pronator muscle. • Pinching of the nerve due to either direct pressure or mechanical compression cause interference in nerve conduction signals. • Repetitive stress applied to nerve over a period of time can cause nerve compression. • Pain in the proximal volar (anterior) forearm region, aggravated by resisted pronation of the forearm and flexion of the elbow. • Positive Phalen test over the pronator teres muscle can be present is 50% of cases.
The target nerve is the one located in the proximal forearm.
CAUSES • Pinching of the nerve due to either direct pressure or mechanical compression cause interference in nerve conduction signals. • Repetitive stress applied to nerve over a period of time can cause nerve compression. • Overuse of the pronator muscle. • Repetitive pronation and supination • Repetitive exertional grasping work: assembly line workers, carpenters, weightlifters, tennis players.
SYMPTOMS • Onset of symptoms are insidious • Abnormal sensibility in volar thumb the thumb, index, and long fingers. • Weakness of finger flexor muscles. • Pain in the proximal forearm. • Numbness in the palm consistent with the distribution of the palmar cutaneous branch of the median nerve.
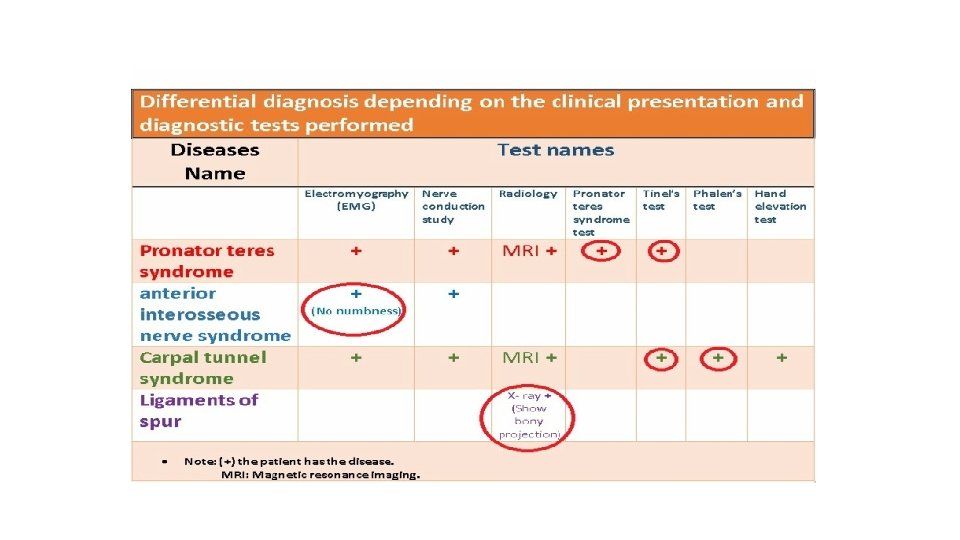
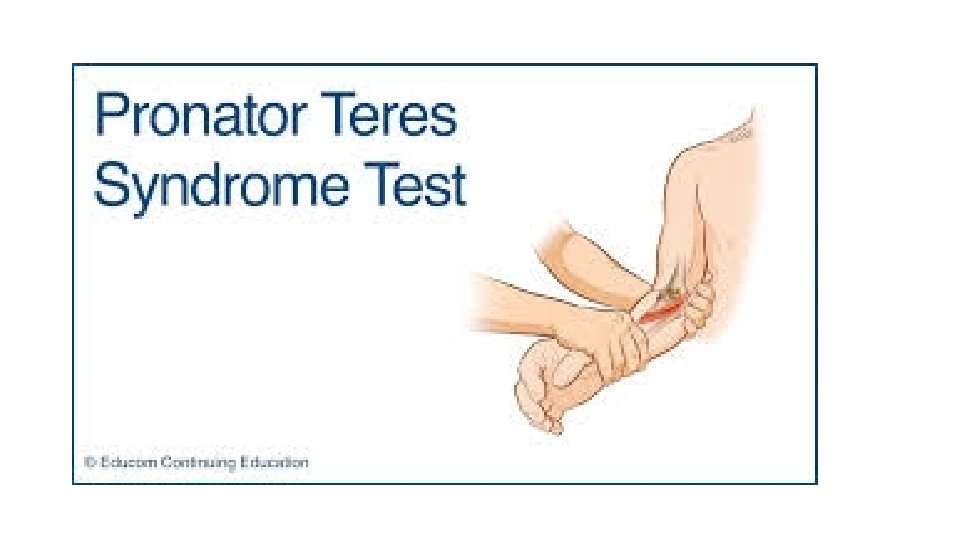
DIAGNOSIS • Usually a delay in diagnosis of 9 months to 2 years. • Although pronator syndrome is often misdiagnosed and does not occur as frequently as carpal tunnel syndrome, its clinical features are well described, and the diagnosis should be made if the clinical features are understood and reasonable suspicion exists. • Different tests are performed: Pronator Teres Test (PTS), Pronator Compression Test (PCT), and Phalen Test.
DIAGNOSIS (c’TD) • Electromyography (EMG) • Nerve Conduction Study • Radiology
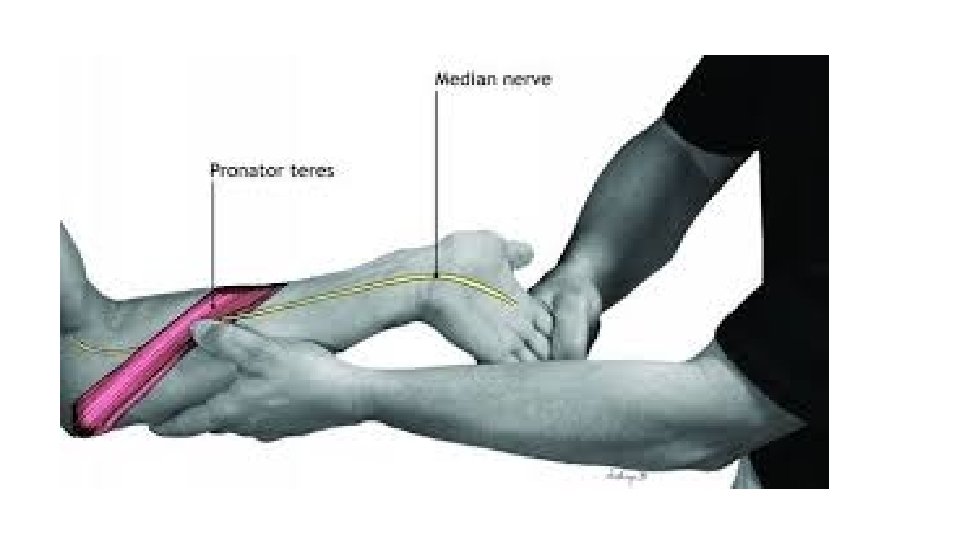
1 -Pronator Teres Test (PTS) • Compression neuropathy of the median nerve at the elbow. • The purpose: help differentiate between PTS and Carpal Tunnel Syndrome. • Physical findings: tenderness over the pronator teres & pain with resisted pronation of forearm.
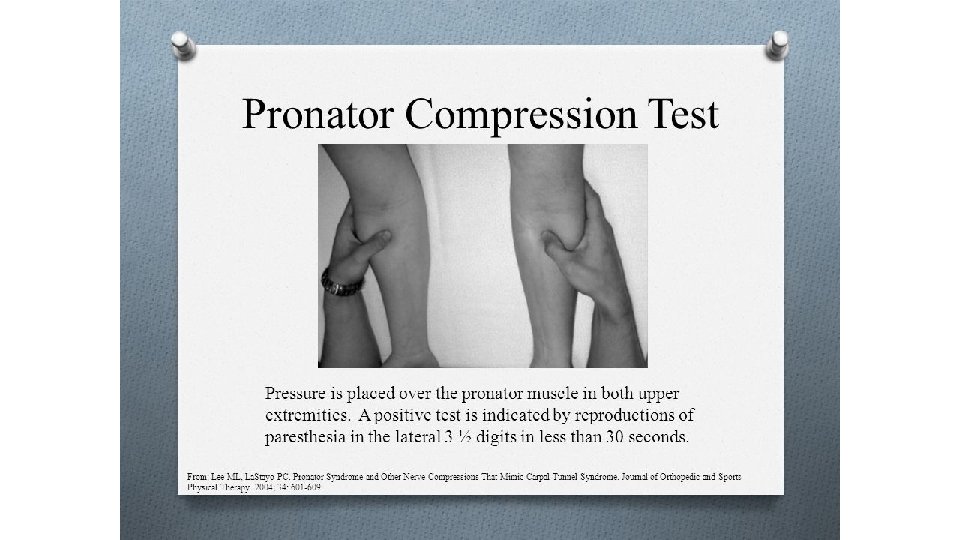
2 -Pronator Compression Test (CPT) • Placing pressure over the pronator muscle on both upper extremities. • Physical findings: A positive test is indicated by reproduction of paresthesia in the lateral 3 and ½ digits in 30 seconds or less.
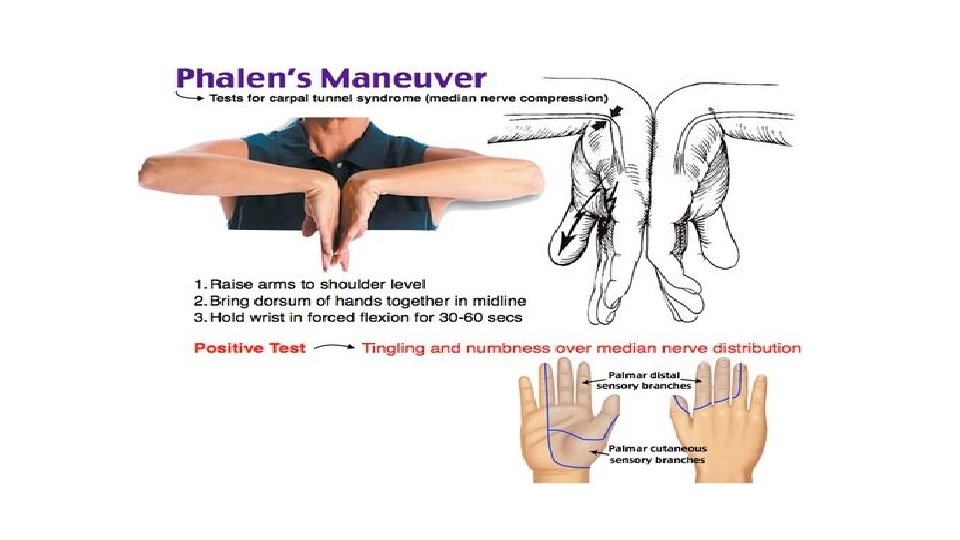
3 -Phalen’s Test • Raise arms to shoulder lever • Bring dorsum of hands together to midline • Hold wrist in forced flexion for 30 -60 secs. • If positive test, tingling & numbness over median nerve distribution. • If the patient has only a proximal median nerve compression, • Then the Phalen’s test for CTS would be expected to be negative.
TREATMENT • Conservative treatment • 50% of patients have been reported to recover in 4 months. • At least for 6 weeks • Rest/Immobilization: Most important aspect is to avoid aggravating activities such as repetitive pronation/supination and aggressive physical activities involving forceful grip. • Physical & occupational therapy, nonsteroidal antiinflammatory, local injections with corticosteroids or local anesthetic.
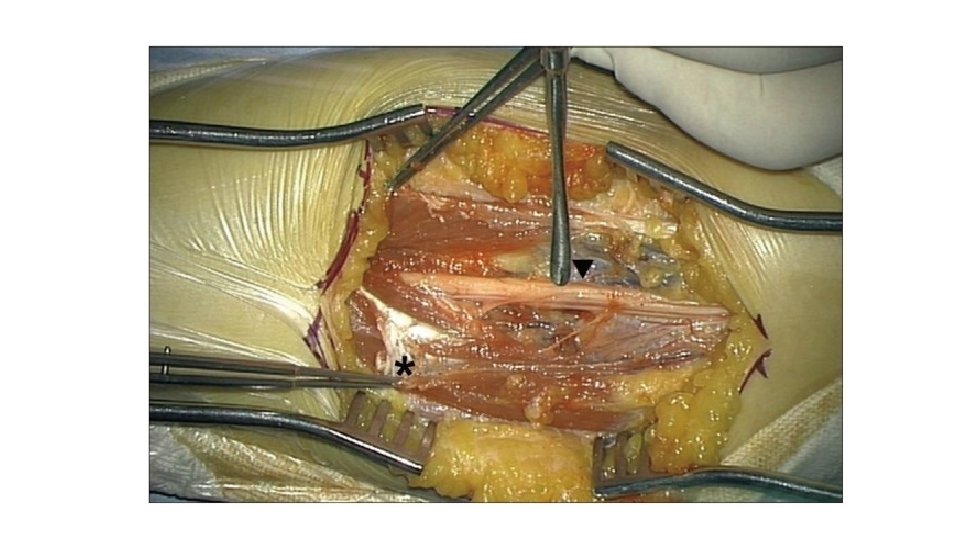
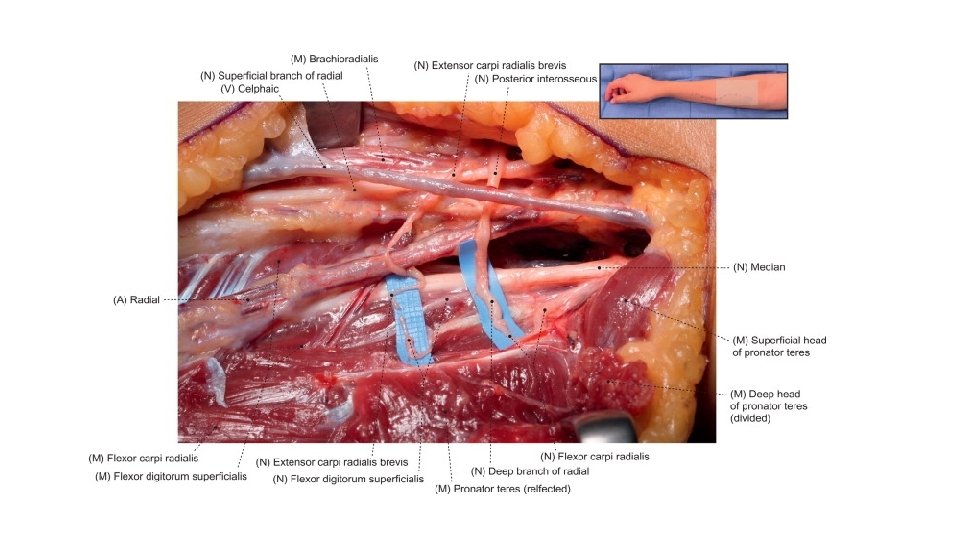
TREATMENT (C’td) • Surgical • Considered when conservation treatment fails • Indicated if patient is symptomatic • Has one or more objective findings in a physical examination of weakness or motor atrophy • Includes exploration of median nerve in the forearm and release of pronator teres muscle and other compressive structures (ligaments of Struthers, lacertus fibrosis, etc ).
TREATMENT COST Groupe I Group 2 Method Non-surgical Surgical Duration 13 +/- 5 months 12 +/- 2 months Treatment Steroid injections Surgery Direct Cost $3, 335 +/$2, 097 $3, 068 +/- $983
ERGONOMIC COST Curvstar Racket = $169 x 18 = 3, 042 Bio. Curve Hammers = $68. 75 x 18 = $1, 237. 5 Weightlifter Elbow Sleeves = $55 x 18 = $990
ERGONOMIC SOLUTIONS-TOOLS • Tennis Player: The Curvstar Racket • Does not follow the traditional straight-necked design of the average tennis racquet. • Takes an ergonomic tendencies like chairs and keyboards of the same design. • Reduces tension put on wrist & elbow while playing. • Curved frame reduces vibrations on each hit.
ERGONOMIC SOLUTIONS (C’td) • Carpenters: Bio. Curve Hammers • Features a patented 19 -degree bent handle that fits the contours of the hand while positioning the wrist in neutral. • Distributes force to large muscle groups, reducing worker fatigue. • High-carbon steel heads with oval-shaped hickory wood handles for strength, long life, and comfort.
ERGONOMIC SOLUTIONS (C’td) • Weightlifter: Elbow Sleeves/Braces • Compression & support for weightlifting, Cross. Fit, etc.
ERGONOMIC SOLUTIONS-POSTURE CHANGE • Carpenters: Target should be at the chest level • Weightlifter: Avoid far-reaching
CONCLUSION • Pronator ulnar syndrome is considered rare, especially in comparison to CTS. • With understanding of relevant anatomy, clinical presentation, and objective tests, a differentiation between the different nerve compression syndromes can at least be considered and investigated. • Based on experience & available literature, the most effective conservative intervention program would include rest/immobilization techniques.
REFERENCES • Tennis Now Newsletter. Curstar Racket Introduces Ergonomics to Tennis [Cited 09 February 2020]. Retrieved from http: //www. tennisnow. com/Blogs/Industry-Insider/April-2014 -(1)/Curvstar-Racquet-Introduces-Ergonomics-to. Tennis. aspx • Ali. Med Ergonomic Solutions. [Cited 09 February 2020]. Retrieved from https: //www. alimed. com/biocurve-hammers. html? pid=69999&gclid=Cjw. KCAi. A-P 7 x. BRAv. Eiw. Ao Vac. BP 9 wq. IEze. Wws. Hbr 9 Qrrqb. JY 0 OBc 2 au 4 EYQi. Qy. K 3 t 2 gi 9 Raa. U 1_hxo. C 9 A 8 QAv. D_Bw. E • Ali. Med Ergonomic Solutions. [Cited 09 February 2020]. Retrieved from https: //www. alimed. com/biocurvehammers. html? pid=69999&gclid=Cjw. KCAi. A-P 7 x. BRAv. Eiw. Aow. Vac. BP 9 wq. IEze. Wws. Hbr 9 Qrrqb. JY 0 OBc 2 au 4 EYQi. Qy. K 3 t 2 gi 9 Raa. U 1_hxo. C 9 A 8 QAv. D_Bw. E • Michael J. Lee & Paul C. La. Stayo (October, 2004). J Ortho Sports Phys Ther. Volume 34. • Marine Dididze & Andrew I. Sherman (2020). Stat. Pearls Publishing: Pronator Teres Syndrome. • Daniel H. Anna. The Occupational Environment: Its Evaluation, Control, and Management. 3 rd Edition, 1060.
REFERENCES (C’td) • Marine Dididze & Andrew I. Sherman (2020). Stat. Pearls Publishing: Pronator Teres Syndrome. • Daniel H. Anna. The Occupational Environment: Its Evaluation, Control, and Management. 3 rd Edition, 1060.