Orthopaedic Neurology Diagnostic Guide to Neurological Levels Motor





















, Extensor Carpi Radialis (Right)")






, Flexor Carpi Ulnaris (Right)")




, and Profundus (Right)")





























, Vastus Intermedius and Lateralis (Right)")










")


























- Slides: 120
Orthopaedic Neurology Diagnostic Guide to Neurological Levels
Motor Power w Interruption of the nerve root causes denervation and paralysis of its myotome. w Pressure on a nerve root can cause a decrease in muscle strength. w Muscle testing is utilized to evaluate whether or not a lesion is present and to what degree it is effecting the muscle strength.
Muscle Grading Chart w Muscle gradations w Description. n 5 – normal n n 4 – good n n 3 – fair n n 2 – poor n n 1 – trace n n 0 - zero n Complete range of motion against gravity with full resistance. Complete range of motion against gravity with some resistance. Complete range of motion against gravity. Complete range of motion with gravity eliminated. Evidence of slight contractility. No joint motion. No evidence of contractility.
Sensation w Pathology to the cord or nerve root results in loss of light touch, followed by loss of sensation of pain. w During recovery from nerve root injury, sensation of pain returns before light touch.
Sensation w The 2 sensations are tested separately, light touch with a cotton swab, pain with pinpricks. w Pinwheels can be utilized to evaluate sensation. w Results can be recorded on a dermatome chart as normal, hyperesthetic (increased), hyposthetic (decreased), dyesthetic (altered), or anesthetic (absent).
Reflex w Interruption in the basic reflex arc results in the loss of reflex, while pressures on the nerve root itself may decrease its intensity (hyporeflexia). w Interruption of the upper motor neuron’s regulatory control results in a hyperactive nerve (hyperreflexia). w Reflexes should be reported as normal, increased, or decreased utilizing bilateral comparison.
Stretch Reflex Arc
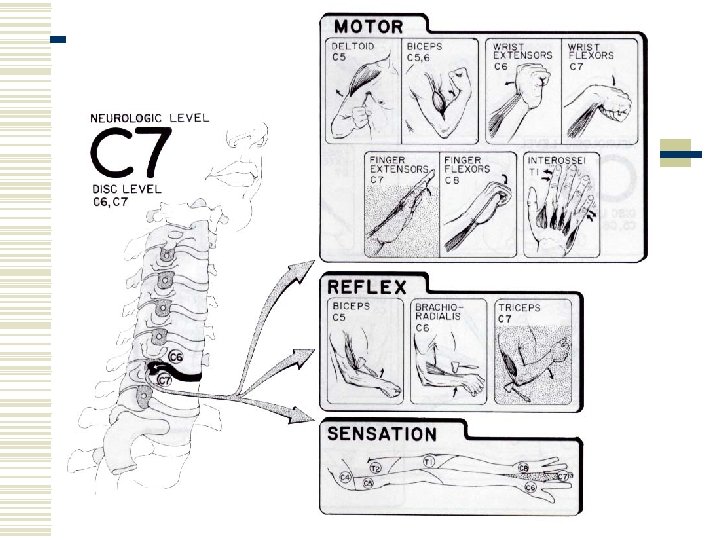
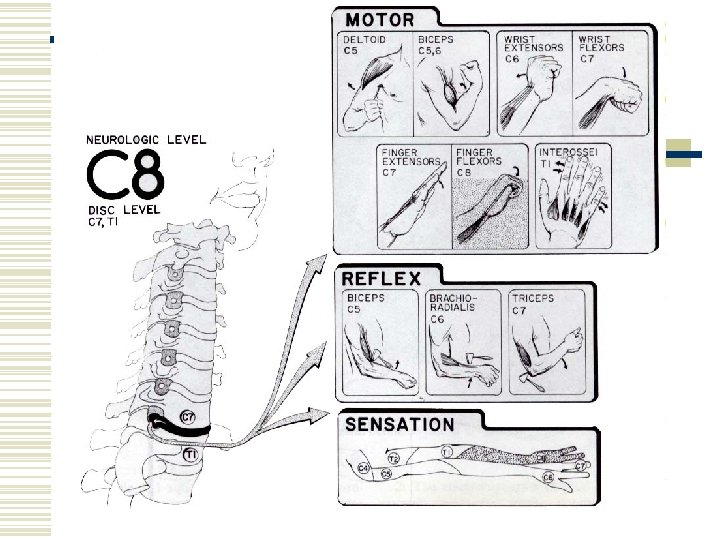
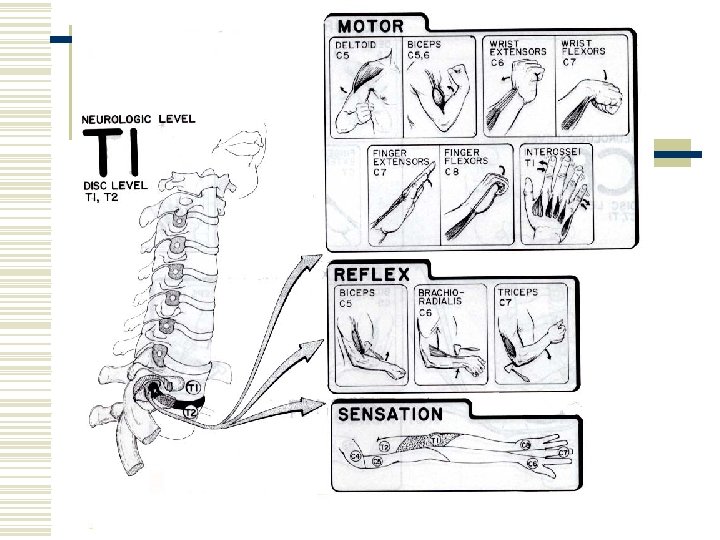
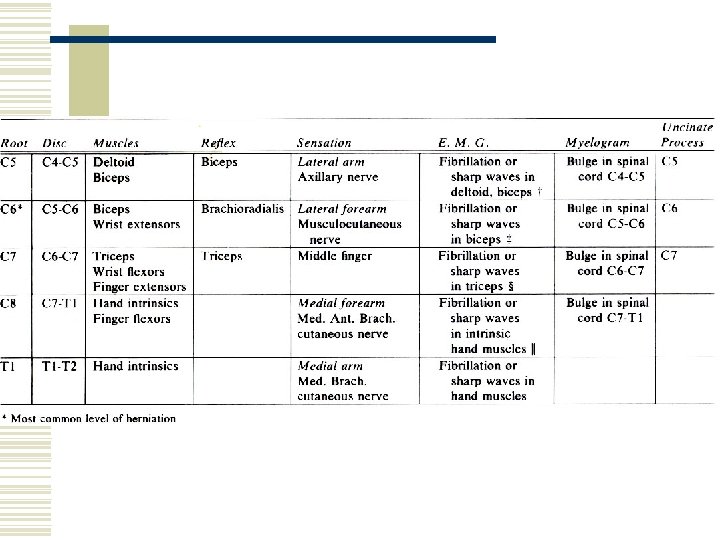
Nerve Root Lesions by Neurologic Level
Evaluation of Nerve Root Lesions Upper Extremity
Cervical Spine w C 5 is the 1 st significant contribution to the brachial plexus. w C 1 -4 are difficult to test; However, C 4 is the major innervation to the diaphragm (via the phrenic nerve).
The Cervical Spine
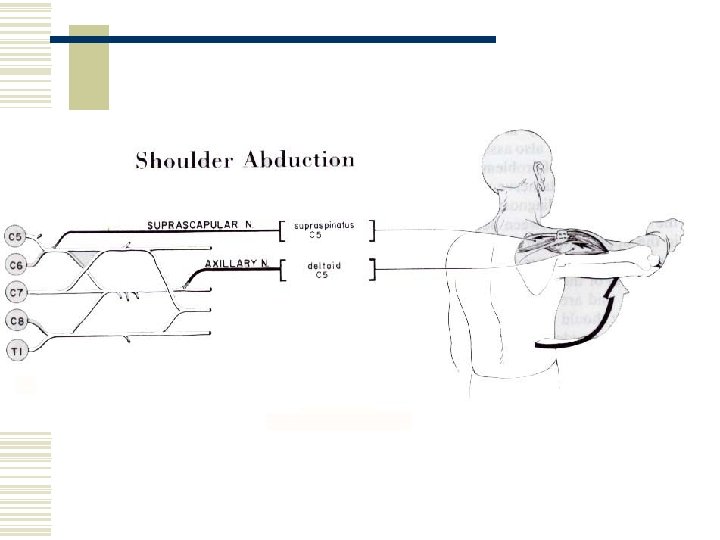
Deltoid & Supraspinatous
Elbow Flexion and Extension
Biceps Brachii & Brachialis
Functions of the Biceps
Muscle Test for the Biceps
Biceps Reflex Test
Memory Trick
Muscle Test Shoulder Abduction
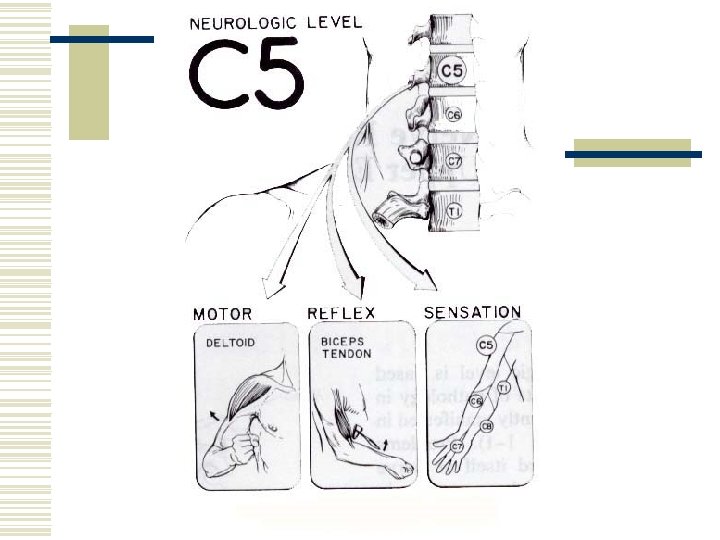
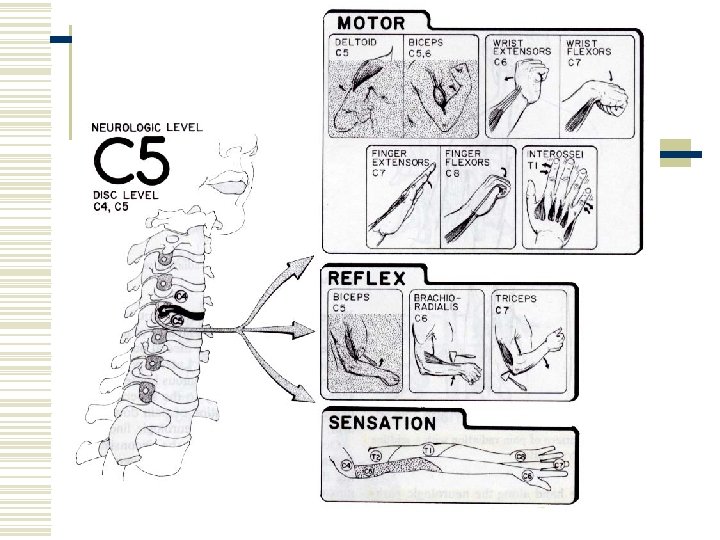
Sensory Distribution C 5
Wrist Extension and Flexion
Extensor Carpi Ulnaris (Left), Extensor Carpi Radialis (Right)
Muscle Test Wrist Extension
Brachioradialis Reflex Test
Memory Trick
Triceps Brachii
Walking With a Crutch Utilizes the Triceps Muscle
Muscle Test Wrist Flexors
Flexor Carpi Radialis (Left), Flexor Carpi Ulnaris (Right)
Finger Extension and Flexion
Extensor Digitorum
Muscle Test Finger Extension
Triceps Reflex Test
Flexor Digitorum Superficialis (Left), and Profundus (Right)
Lumbricales
Muscle Test Finger Flexors
Memory Trick
Finger Abduction and Adduction
Muscle Test Finger Abduction
Muscle Test Finger Adduction
Summary of Muscle Testing for the Upper Extremity
Summary of Reflex Testing for the Upper Extremity
Summary of Sensation for the Upper Extremity
Cervical Vertebrae and Nerve Roots
Herniated Cervical Disc
Occiput & C 1 Articulation
C 1 and C 2 Articulation
Anatomic Basis for Posterior Cervical Disc Herniation
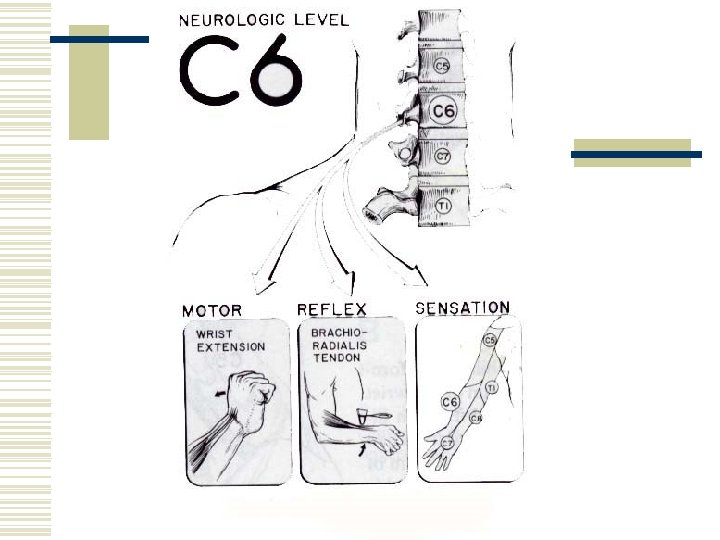
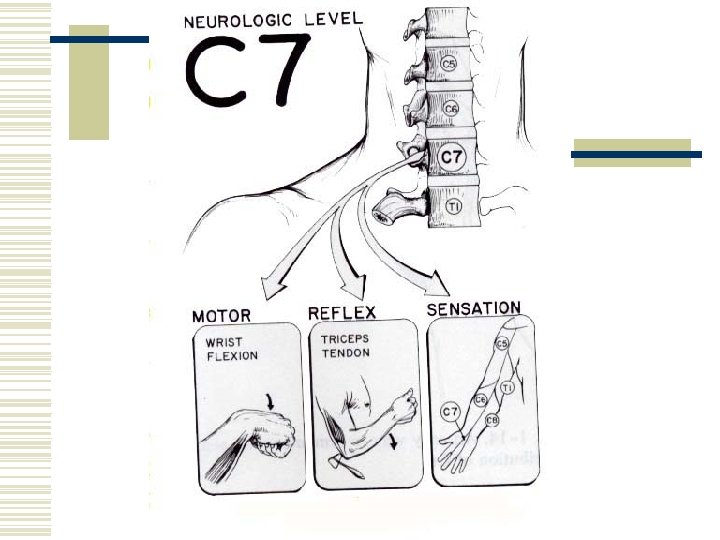
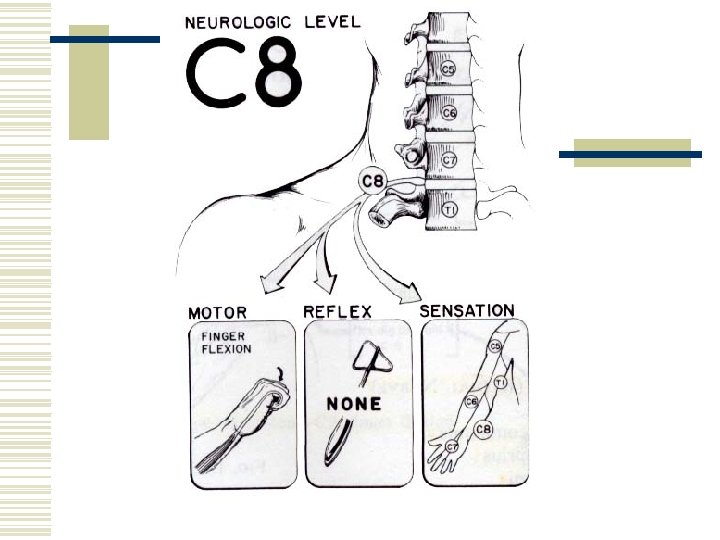
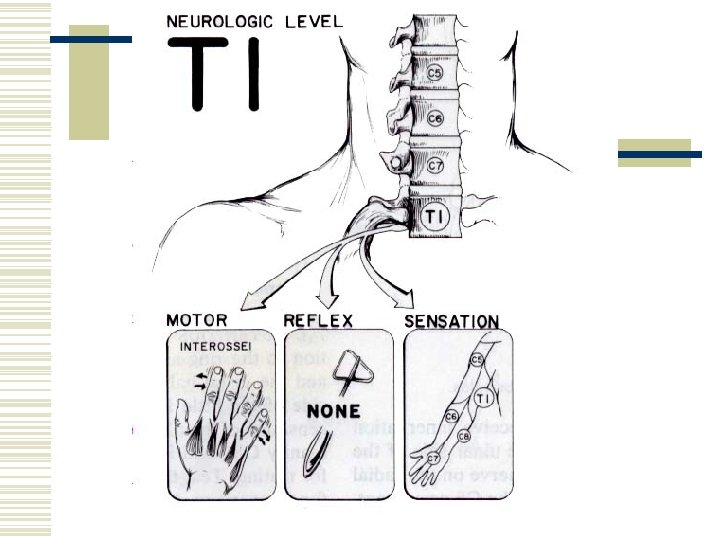
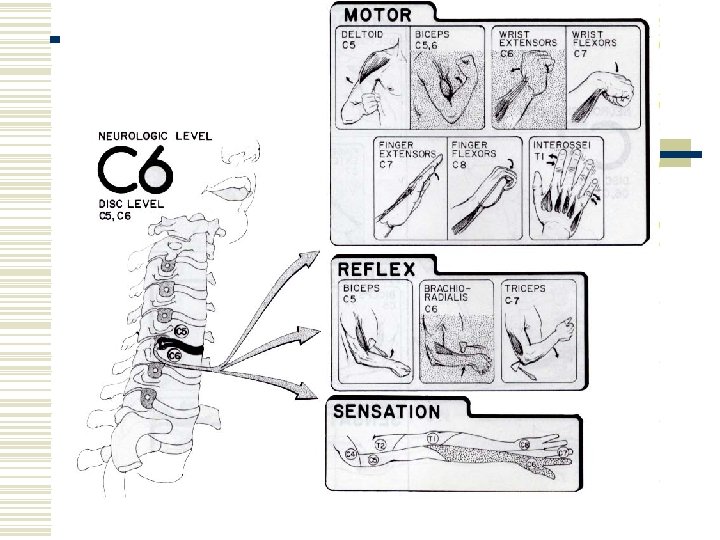
Neurologic Levels in Upper Extremity w Motor n n n C 5 – shoulder abduction C 6 – wrist extension C 7 – wrist flexion and finger extension C 8 – finger flexion T 1 – finger abduction, adduction
Neurologic Levels in Upper Extremity w Sensation n n n C 5 – lateral arm C 6 – lateral forearm, thumb, and index finger C 7 – middle finger (variable) C 8 – medial forearm, ring, and small finger T 1 – medial arm T 2 - Axilla
Neurologic Levels in Upper Extremity w Reflex n n n C 5 – biceps C 6 – Brachioradialis C 7 - triceps
Whiplash Injury to the Cervical Spine
Anatomy of a Cervical Vertebrae
Orthopedic Tests Cervical Spine w Valsalva test w Distraction test w Compression test
Valsalva Test
Distraction Test
Compression Test
Thoracic Spine
Beevor’s Spine
Hip Flexion
Iliopsoas
Muscle Test Iliopsoas
Knee Extension
Rectus Femoris (Left), Vastus Intermedius and Lateralis (Right)
Extension Lag
Muscle Test Quadriceps
Hip Adduction
Adductors
Muscle Test Hip Adductors
Dermatomes of the Lower Extremity
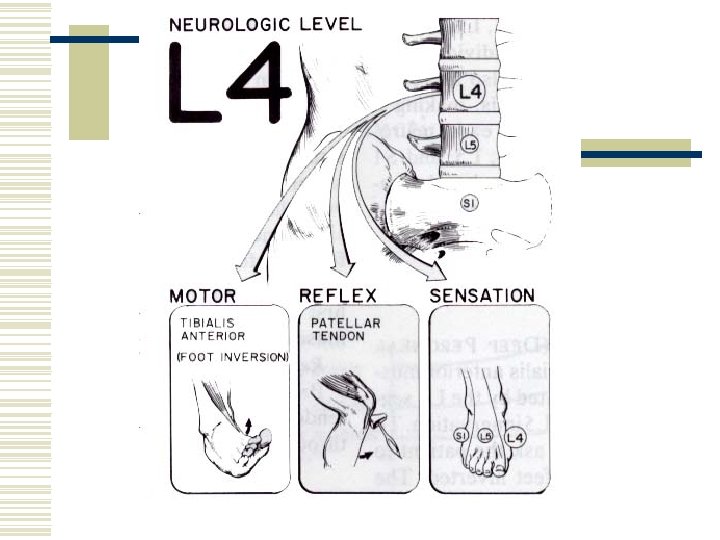
Foot Inversion
Muscle Test Tibialis Anterior
Patellar Tendon Reflex
Memory Trick
Foot Dorsiflexion (Ankle Extension)
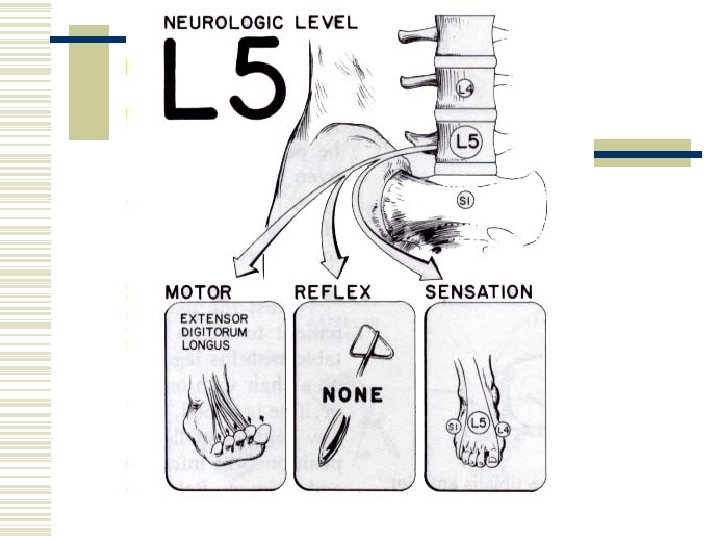
Extensor Hallucis Longus
Muscle Test Extensor Hallucis Longus
Muscle Test Toe Extensors
Memory Trick
Hip Abduction
Gluteus Medius
Muscle Test Gluteus Medius
L 5 Sensory Dermatome
Foot Eversion
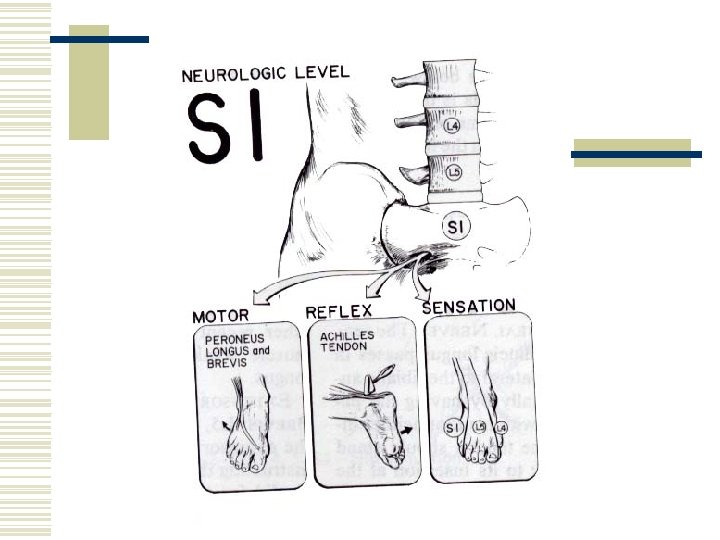
Peroneus Longus & Brevis
Muscle Test Peronei Muscles
Foot Plantarflexion
Gastrocnemius & Soleus
Muscle Test Gastrocnemius
Hip Extension
Gluteus Maximus
Muscle Test Gluteus Maximus
Achilles Reflex Test
Memory Trick
Sensory Dermatomes S 2, S 3, S 4, S 5
Sensory Dermatomes L 4 -S 1
Testing Sensation
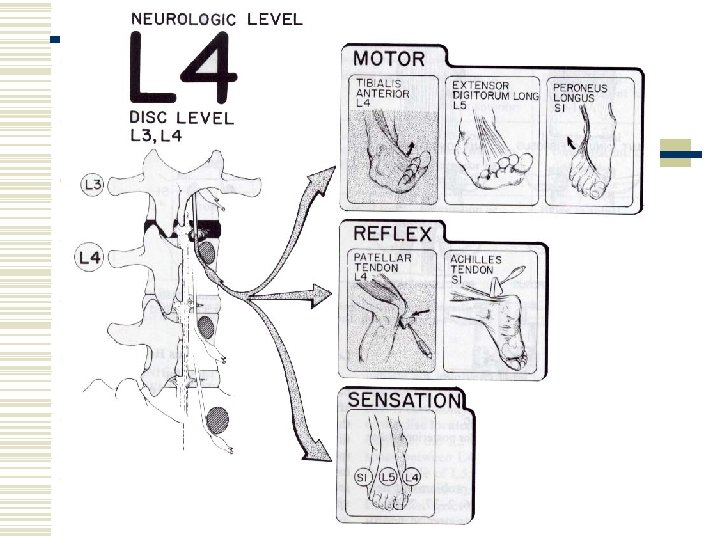
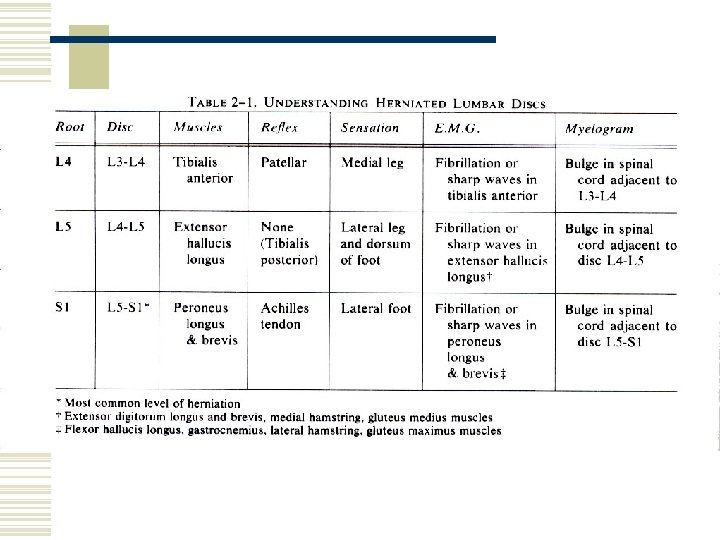
Anatomic Basis for Posterior Lumbar Disc Herniation
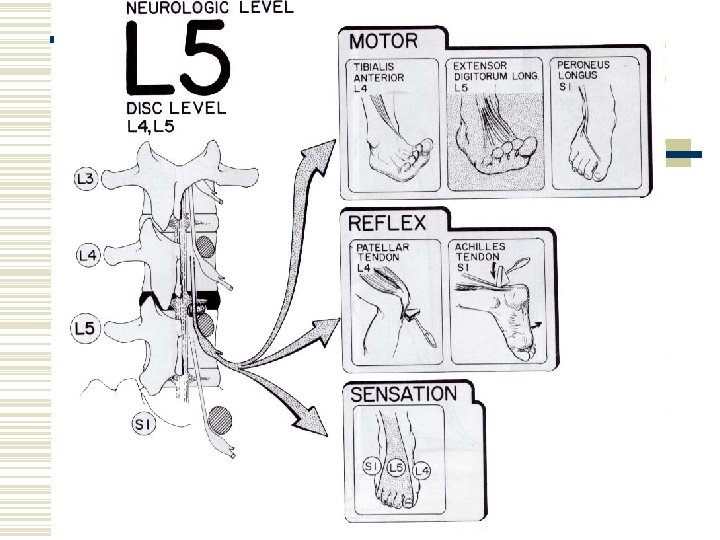
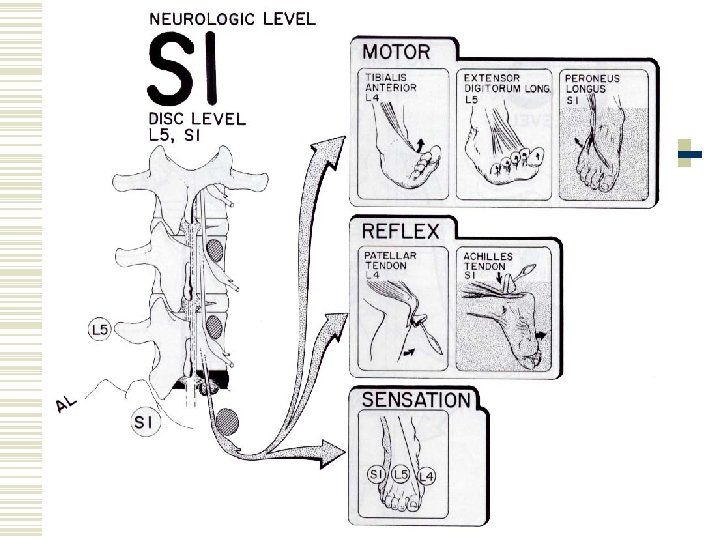
Neurologic Levels in Lower Extremity w Motor n n L 3 – quadriceps (L 2, L 3, L 4) L 4 – Tibialis anterior L 5 – toe extensors S 1 - Peronei
Neurologic Levels in Lower Extremity w Sensation n n n n T 12 – lower abdomen just proximal to inguinal ligament L 1 – upper thigh just distal to inguinal ligament L 2 – mid thigh L 3 – lower thigh L 4 – medial leg – medial side of foot L 5 – lateral leg – dorsum of foot S 1 – lateral side of foot S 2 – longitudinal strip, posterior thigh
Neurologic Levels in Lower Extremity w Reflex n n n L 4 – patellar L 5 – Tibialis posterior (difficult to obtain) S 1 – Achilles tendon