Orthopaedic Emergencies Orthopedic Emergencies Open Fractures Acute Compartment



 fracture occurs when the skin overlying a fracture")
, usually clean, no soft")
 ,")




 Paresthesias Paralysis")
< 30 mm.")





 - Usually caused by fall")

















 Growth retardation,")










 Paramedical staff Primary trauma center")
 guidelines Primary and secondary surveys Adequate airway")

















 & The Canadian C-spine rule Both have:")


 AABBCDS Adequacy, Alignment Bone abnormality, Base of skull Cartilage")






 10 mm (adult) Retropharyngeal space (C 2 -")









 -weakness/paraparesis in multiple root distribution -reduced deep tendon reflexes")
 to preserve bowel")


- Slides: 94
Orthopaedic Emergencies
Orthopedic Emergencies Open Fractures Acute Compartment Syndrome Neurovascular injuries Dislocations Septic Joints Spinal cord injury
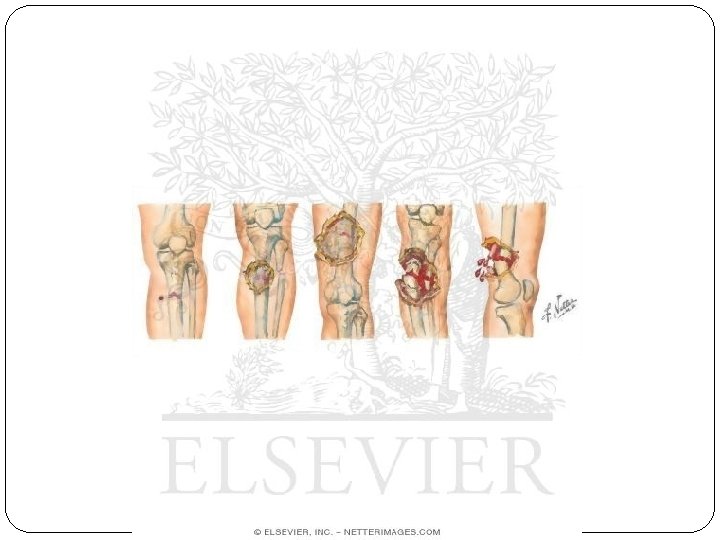
Open Fractures
Open Fractures An open (or compound) fracture occurs when the skin overlying a fracture is broken, allowing communication between the fracture and the external environment
Open Fractures- Gustilo-Anderson Classification: Type I: Small wound (<1 cm), usually clean, no soft tissue damage and no skin crushing (i. e. a low energy fracture) Type II: Moderate wound (>1 cm), minimal soft tissue damage or loss, may have comminution of fracture (i. e. a low-moderate energy fracture) Type III: Severe skin wound, extensive soft tissue damage (i. e. high energy fracture) Three grades: A – adequate soft tissue coverage, B – fracture cover not possible without local/distant flaps, C – arterial injury that needs to be repaired.
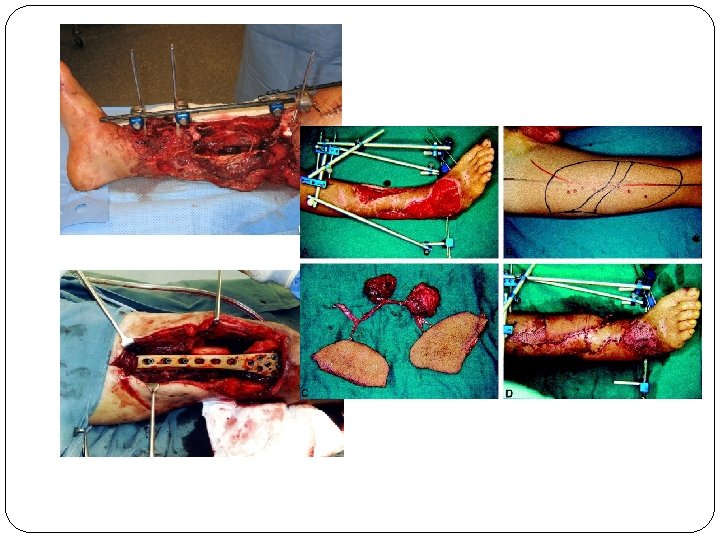
Open Fractures- Management ABCDE – check neurovascular status (pulses, cap. refill, sensation, motor) , fluid resuscitation, blood Antibiotics, tetanus prophylaxis – 48 -72 hrs Surgical debridement – removal of de-vitalised tissue, irrigation Stabilization of fracture – internal/external, if closure delayed then external prefered Early definitive wound cover – split skin grafts, local/distant flaps (involve plastics)
Open Fractures- Complications Wound infection – 2% in Type I , >10% in Type III Osteomyelitis – staph aureus, pseudomona sp. Gas gangrene Tetanus Non-union/malunion
Acute Compartment Syndrome
Acute Compartment Syndrome An injury or condition that causes prolonged elevation of interstitial tissue pressures Increased pressure within enclosed fascial compartment leads to impaired tissue perfusion Prolonged ischemia causes cell damage which leads to oedema Oedema further increase compartment pressure leading to a vicious cycle Extensive muscle and nerve death >4 hours Nerve may regenerate but infarcted muscle is replaced by fibrous tissue (Volkmann’s ischaemic contracture)
ACS- Etiology Crush injury Circumferential burns Snake bites Fractures – 75% Tourniquets, constrictive dressings/plasters Haematoma – pt with coagulopathy at increased risk
ACS- Findings 5 Ps of ischaemia Pain (out of proportion to injury) Paresthesias Paralysis Pulselessness Pallor Severe pain, “bursting” sensation Pain with passive stretch Tense compartment Tight, shiny skin Can confirm diagnosis by measuring intracompartmental pressures (Stryker STIC)
120 mm Hg Difference between diastolic pressure and compartment pressure (delta pressure)< 30 mm. Hg is indication for immediate decompression 60 mm Hg Pulse Pressure Ischemia 30 mm Hg Elevated Pressure 10 mm Hg Normal 0 mm Hg
ACS - Mangement Early recognition Muscle necrosis at delta pressure < 30 mm Hg Irreversible injury 4 -6 hrs Remove cast, bandages and dressings Arrange urgent fasciotomy
Fasciotomy
ACS- Complications Volkman ischaemic contractures Permanent nerve damage Limb ischaemia and amputation Rhabdomyolysis and renal failure
Dislocations
Dislocations Displacement of bones at a joint from their normal position Do xrays before and after reduction to look for any associated fractures
Dislocation- Shoulder Most common major joint dislocation Anterior (95%) - Usually caused by fall on hand Posterior (2 -4%) – Electrocution/seizure May be associated with: Fracture dislocation Rotator cuff tear Neurovascular injury
Dislocation- Knee Injury to popliteal artery and vein is common Peroneal nerve injury in 20 -40% of knee dislocations Associated with ligamentous injury Anterior (31%) Posterior (25%) Lateral (13%) Medial (3%)
Dislocation- Hip Usually high-energy trauma More frequent in young patients Posterior- hip in internal rotation, most common Anterior- hip in external rotation Central - acetabular fracture May result in avascular necrosis of femoral head Sciatic nerve injury in 10 -35%
Neurovascular Injuries
Neurovascular Injuries Fractures and dislocations can be associated with vascular and nerve damage Always check neurovascular status before and after reduction
Neurovascular Injuries - Etiology Fracture Humerus, femur Dislocation Elbow, knee Direct/penetrating trauma Thrombus Direct Compression/ Acute Compartment Syndrome Cast, unconscious
Common vascular injuries Injury Vessel 1 st rib fracture Subclavian artery/vein Shoulder dislocation Axillary artery Humeral supracondylar fracture Brachial artery Elbow Dislocation Brachial artery Pelvic fracture Presacral and internal iliac Femoral supracondylar fracture Femoral artery Knee dislocation Popliteal artery/vein Proximal tibial Popliteal artery/vein
Clinical Features & Mx Paraesthesia/numbness Injured limb cold, cyanosed, pulse weak/absent Call for help! Remove all bandages and splints Reduce the fracture/ dislocation and reassess circulation If no improvement then vessels must be explored by operation If vascular injury suspected angiogram should be performed immediately
Common nerve injuries Injury Nerve Shoulder dislocation Axillary Humeral shaft fracture Radial Humeral supracondylar fracture Radial or median Elbow medial condyle Ulnar Monteggia fracture-dislocation Posterior-interosseous Hip dislocation Sciatic Knee dislocation Peroneal
Clinical Features & Mx Paraesthesia and weakness to supplied area Closed injuries: nerve seldom severed, 90% recovery in 4 months. If not do nerve conduction studies +/- repair Open injuries: Nerve injury likely complete. Should be explored at time of debridement/repair Indications for early exploration: Nerve injury associated with open fracture Nerve injury in fracture that needs internal fixation Presence of concomitant vascular injury Nerve damage diagnosed after manipulation of fracture
Septic Joint Septic Arthritis
Septic Joint/Septic Arthritis Inflammation of a synovial membrane with purulent effusion into the joint capsule. Followed by articular cartilage erosion by bacterial and cellular enzymes. Usually monoarticular Usually bacterial Staph aureus Streptococcus Neisseria gonorrhoeae
Septic Joint- Etiology Direct invasion through penetrating wound, intra-articular injection, arthroscopy Direct spread from adjacent bone abcess Blood spread from distant site
Septic Joint- Location Knee- 40 -50% Hip- 20 -25%* *Hip is the most common in infants and very young children Wrist- 10% Shoulder, ankle, elbow- 10 -15%
Septic Joint- Risk Factors Prosthetic joint Joint surgery Rheumatoid arthritis Elderly Diabetes Mellitus IV drug use Immunosupression AIDS
Septic Joint- Signs and Symptoms Rapid onset Joint pain Joint swelling Joint warmth Joint erythema Decreased range of motion Pain with active and passive ROM Fever, raised WCC/CRP, positive blood cultures
Septic Joint- Treatment Diagnosis by aspiration Gram stain, microscopy, culture Leucocytes >50 000/ml highly suggestive of sepsis Joint washout in theatre IV Abx 4 -7 days then orally for another 3 weeks Analgesia Splintage
Septic Joint- Complications Rapid destruction of joint with delayed treatment (>24 hours) Growth retardation, deformity of joint (children) Degenerative joint disease Osteomyelitis Joint fibrosis and ankylosing Sepsis Death
Spinal cord injury
Outline Goal of spine trauma care Pre-hospital management Clinical and neurologic assessment Acute spinal cord injury Term, type and clinical characteristic Common cervical spine fracture and dislocation
Goal of spine trauma care Protect further injury during evaluation and management Identify spine injury or document absence of spine injury Optimize conditions for maximal neurologic recovery
Goal of spine trauma care Maintain or restore spinal alignment Minimize loss of spinal mobility Obtain healed & stable spine Facilitate rehabilitation
Suspected Spinal Injury High speed crash Unconscious Multiple injuries Neurological deficit Spinal pain/tenderness
Pre-hospital management Protect spine at all times during the management of patients with multiple injuries Up to 15% of spinal injuries have a second (possibly non adjacent) fracture elsewhere in the spine Ideally, whole spine should be immobilized in neutral position on a firm surface
PROTECTION PRIORITY Detection Secondary “Log-rolling”
Pre-hospital management Cervical spine immobilization Transportation of spinal cord-injured patients
Cervical spine immobilization “Safe assumptions” Head injury and unconscious Multiple trauma Fall Severely injured worker Unstable spinal column Hard backboard, rigid cervical collar and lateral support (sand bag) Neutral position
Philadelphia hard collar
Transportation of spinal cord-injured patients Emergency Medical Systems (EMS) Paramedical staff Primary trauma center Spinal injury center
Clinical assessment Advance Trauma Life Support (ATLS) guidelines Primary and secondary surveys Adequate airway and ventilation are the most important factors Supplemental oxygenation Early intubation is critical to limit secondary injury from hypoxia
Physical examination Information Mechanism energy, energy Direction of Impact Associated Injuries
Is the patient awake or “unexaminable”? What’s the difference ? Awake ask/answer question pain/tenderness motor/sensory exam OW! Not awake you can ask (but they won’t answer) can’t assess tenderness no motor/sensory exam ------
“Unexaminable” ≠ “No exam”
Physical examination Inspection and palpation Occiput to Coccyx Soft tissue swelling and bruising Point of spinal tenderness Gap or Step-off Spasm of associated muscles Neurological assessment Motor, sensation and reflexes PR Do not forget the cranial nerve (C 0 -C 1 injury)
Neurogenic Shock Temporary loss of autonomic function of the cord at the level of injury results from cervical or high thoracic injury Presentation Flaccid paralysis distal to injury site Loss of autonomic function hypotension vasodilatation loss of bladder and bowel control loss of thermoregulation warm, pink, dry below injury site bradycardia
Comparison of neurogenic and hypovolemic shock Neurogenic Hypovolemic Etiology Loss of sympathetic outflow Loss of blood volume Blood pressure Hypotension Heart rate Bradycardia Tachycardia Skin temperature Warm Cold Urine output Normal Low 57
Definitions of terms Neurologic level Most caudal segment with normal sensory and motor function both sides Skeletal level Radiographic level of greatest vertebral damage Complete injury Absence of sensory and motor function in the lowest sacral segment Incomplete injury Partial preservation of sensory and/or motor function below the neurologic level
Neurologic assessment Spinal shock Bulbocavernosus reflex Complete VS incomplete cord injury ตองพนภาวะ spinal shock ไปกอน Sacral sparing Voluntary anal sphincter control Toe flexor Perianal sensation Anal wink reflex
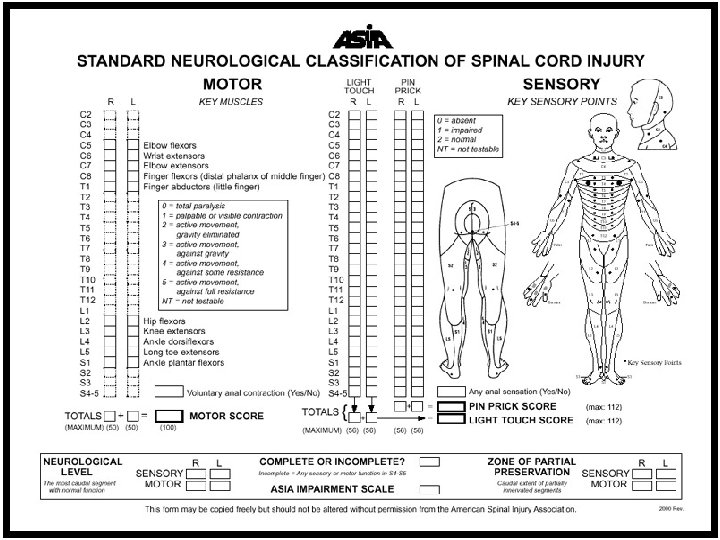
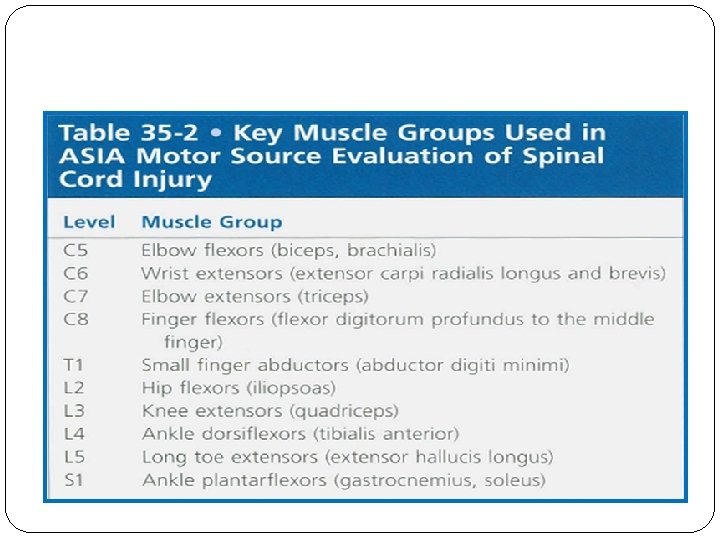
Neurologic assessment American Spinal Injury Association grade Grade A – E American Spinal Injury Association score Motor score (total = 100 points) Key muscles : 10 muscles Sensory score (total = 112 points) Key sensory points : 28 dermatomes
Incomplete cord injury Anterior cord syndrome Brown-Sequard syndrome Central cord syndrome
Anterior cord syndrome Loss of motor, pain and temperature Preserved propioception and deep touch
Brown-Sequard syndrome Loss of ipsilateral motor and propioception Loss of contralateral pain and temperature
Central cord syndrome Weakness : upper > lower Variable sensory loss Sacral sparing
Radiographic imaging Who needs an x- ray of the spine ? ü NEXUS -The National Emergency X- Radiograph Utilization Study Prospective study to validate a rule for the decision to obtain cervical spine x- ray in trauma patients Hoffman, N Engl J Med 2000; 343: 94 -99 ü Canadian C-Spine rules Prospective study whereby patients were evaluated for 20 standardized clinical findings as a basis formulating a decision as to the need for subsequent cervical spine radiography Stiell I. JAMA. 2001; 286: 1841 -1846
NEXUS Criteria: 1. Absence of tenderness in the posterior midline 2. Absence of a neurological deficit 3. Normal level of alertness (GCS score = 15) 4. No evidence of intoxication (drugs or alcohol) 5. No distracting injury/pain
NEXUS Patient who fulfilled all 5 of the criteria were considered low risk for C-spine injury No need C-spine X-ray For patients who had any of the 5 criteria radiographic imaging was indicated ( AP, lateral and open mouth views)
The Canadian C-spine Rule for alert and stable trauma patients where cervical spine injury is a concern. Any high-risk factor that mandates radiography? Age>65 yrs or Dangerous mechanism or Paresthesia in extremities NO Any low-risk factor that allows safe assessment of range of motion? • Simple rear-end MVC, or • Sitting position in ER, or • Ambulatory at any time, or • Delayed onset of neck pain, or • Absence of midline C-spine tenderness YES Able to actively rotate neck? • 45 degrees left and right ABLE No Radiography YES NO Radiography UNABLE
National Emergency X Radiography Utilization Study (NEXUS) & The Canadian C-spine rule Both have: Excellent negative predictive value for excluding patients identified as low risk
Clearance of Cervical Spine Injury in Conscious, Symptomatic Patients 1. Radiological evaluation of the cervical spine is indicated for all patients who do not meet the criteria for clinical clearance as described above 2. Imaging studies should be technically adequate and interpreted by experienced clinicians
Cervical Spine Imaging Options Plain films AP, lateral and open mouth view Optional: Oblique and Swimmer’s CT Better for occult fractures MRI Very good for spinal cord, soft tissue and ligamentous injuries Flexion-Extension Plain Films to determine stability
Radiolographic evaluation X-ray Guidelines (cervical) AABBCDS Adequacy, Alignment Bone abnormality, Base of skull Cartilage Disc space Soft tissue
Adequacy Must visualize entire C-spine A film that does not show the upper border of T 1 is inadequate Caudal traction on the arms may help If can not, get swimmer’s view or CT
Swimmer’s view
Alignment • The anterior vertebral line, posterior vertebral line, and spinolaminar line should have a smooth curve with no steps or discontinuities • Malalignment of the posterior vertebral bodies is more significant than that anteriorly, which may be due to rotation • A step-off of >3. 5 mm is significant anywhere
Lateral Cervical Spine X-Ray Anterior subluxation of one vertebra on another indicates facet dislocation < 50% of the width of a vertebral body unilateral facet dislocation > 50% bilateral facet dislocation
Bones
Disc Spaces Should be uniform Assess spaces between the spinous processes
Soft tissue Nasopharyngeal space (C 1) 10 mm (adult) Retropharyngeal space (C 2 - C 4) 5 -7 mm Retrotracheal space 14 mm (children) 22 mm (adults) (C 5 -C 7)
AP C-spine Films Spinous processes should line up Disc space should be uniform Vertebral body height should be uniform. Check for oblique fractures.
Open mouth view Adequacy: all of the dens and lateral borders of C 1 & C 2 Alignment: lateral masses of C 1 and C 2 Bone: Inspect dens for lucent fracture lines
CT Scan Thin cut CT scan should be used to evaluate abnormal, suspicious or poorly visualized areas on plain film The combination of plain film and directed CT scan provides a false negative rate of less than 0. 1%
MRI Ideally all patients with abnormal neurological examination should be evaluated with MRI scan
Management of SCI Primary Goal Prevent secondary injury Immobilization of the spine begins in the initial assessment Treat the spine as a long bone Secure joint above and below Caution with “partial” spine splinting
Management of SCI Spinal motion restriction: immobilization devices ABCs Increase Fi. O 2 Assist ventilations as needed with c-spine control Indications for intubation : Acute respiratory failure GCS <9 Increased RR with hypoxia PCO 2 > 50 VC < 10 m. L/kg IV Access & fluids titrated to BP ~ 90 -100 mm. Hg
Management of SCI Look for other injuries: “Life over Limb” Transport to appropriate SCI center once stabilized Consider high dose methylprednisolone Controversial as recent evidence questions benefit Must be started < 8 hours of injury Do not use for penetrating trauma 30 mg/kg bolus over 15 minute After bolus: infusion 5. 4 mg/kg IV for 23 hours
Principle of treatment Spinal alignment deformity/subluxation/dislocation reduction Spinal column stability unstable stabilization Neurological status neurological deficit decompression
Cauda Equina Syndrome Compression of lumbosacral nerve roots below conus medullaris secondary to large central herniated disc/extrinsic mass/infection/trauma
Clinical Features motor (LMN signs) -weakness/paraparesis in multiple root distribution -reduced deep tendon reflexes (knee and ankle) -sphincter disturbance (urinary retention and fecal incontinence due to loss of anal sphincter tone) sensory -saddle anesthesia (most common sensory deficit) -pain in back radiating to legs, crossed straight leg test -bilateral sensory loss or pain: involving multiple dermatomes
Management Surgical emergency - requires urgent investigation and decompression (<48 hrs) to preserve bowel and bladder function
The End
Thank you for your attention