Orbital Disorders 2 By Professor Ahmad Mostafa Proptosis

Orbital Disorders 2 By Professor Ahmad Mostafa

Proptosis Definition n Clinical evaluation n Treatment n
 of one or")
I. Definition ■ Proptosis is defined as anterior displacement (or protrusion) of one or both globes within the bony orbit. ■ The normal distance (as measured with a Hertel Exophthalmometer) from the lateral orbital rim to the corneal apex (in adults) is 14 to 21 mm. ■ A distance > 21 mm or a 2 mm difference between the two eyes is generally abnormal.

II. Clinical evaluation of a case of proptosis n n n History Examination Investigations
 History ● The history should be taken prior to examining the patient and")
(A) History ● The history should be taken prior to examining the patient and should include: n n n n Ocular ENT Medical Neurological Family history Hx of trauma Hx. of malignancy Therapeutic hx.

1. Ocular History n The four main symptoms of orbital disease are: 1. 2. 3. 4. Proptosis Pain Diplopia Visual impairment

Pain n. A painful lesion is usually either: 1. Inflammatory or 2. Malignant

Diplopia n Diplopia in orbital diseases are caused by limitation of ocular motility which may be caused by: 1. Restrictive myopathy (dysthyroid ophthalmopathy) 2. Neurological lesion 3. Blow-out fracture 4. Optic nerve sheath meningioma

Visual impairment n Reduced visual acuity in orbital diseases may be caused by: 1. Optic nerve compression 2. Exposure keratopathy 3. Choroidal folds

Onset, duration & course n A benign tumor is usually slow growing, unassociated with pain, diplopia, or visual impairment n A rapidly progressive proptosis in a child would suggest a malignant tumor, whereas in adults an acute onset of painful proptosis associated with chemosis and diplopia would be more suggestive of orbital inflammatory pseudotumor

n A sudden onset would indicate orbital hemorrhage n Intermittent Proptosis: 1. Orbital varices (90%) increases on bending forward 2. Recurrent hemorrhage (hemophilia) 3. Vascular tumor n Chronic progressive proptosis: 1. Neoplastic 2. Chronic inflammatory

Benign Vs Malignant tumors Benign tumors are characterized by: - Slow course - Minimal or no limitation of ocular motility - No visual disturbances n Malignant tumors are characterized by: - Rapid course - Early limitation of ocular motility - Early visual disturbances & diplopia n

2. ENT History n Many orbital tumors and inflammations may develop secondary to primary lesions in the sinuses, nasal cavity, or nasopharynx, for example: 1. Ethmoidal sinusitis 2. Maxillary carcinoma
 History n A history of systemic disease or tumor may indicate")
3. Medical (Systemic) History n A history of systemic disease or tumor may indicate the cause of proptosis e. g. in cases of diabetes, neurofibromatosis, or carcinoma of the breast, lung or prostate.

4. Family history n A family history in a patient with a suspected orbital tumor should include questions about ocular disease, cancer, or other systemic familial disease.
 Examination n R/O Pseudoproptosis n Routine ocular examonation n Specific orbital examination")
(B) Examination n R/O Pseudoproptosis n Routine ocular examonation n Specific orbital examination
 R/O Pseudoproptosis n The main causes of pseudoproptosis are: 1. Large ipsilateral globe")
(1) R/O Pseudoproptosis n The main causes of pseudoproptosis are: 1. Large ipsilateral globe (high myopia, buphthalmos). 2. Contralateral enophthalmos (contralateral small globe, contralateral cicatricial tumour especially metastatic breast carcinoma) 3. Asymmetric orbital size (congenital, postirradiation, post-surgical) 4. Asymmetric palpebral fissures (usually caused by ipsilateral eyelid retraction, scarring or facial nerve paralysis or contralateral ptosis)
 Routine ocular examonation n The ocular examination should precede eualvation of the orbit,")
(2) Routine ocular examonation n The ocular examination should precede eualvation of the orbit, including: 1. 2. 3. 4. 5. 6. Visual acuity examination Slitlamp biomicroscopy Examination of the pupils Examination of ocular motility Tonometry (IOP) Fundus examination
 Specific orbital examination Inspection n Plapation n Auscultation n Compression (Retropulsion) n Sensation")
(3) Specific orbital examination Inspection n Plapation n Auscultation n Compression (Retropulsion) n Sensation n Measurement n Forced duction test n Dynamic properties n
")
1. Inspection Laterality: Unilateral Vs bilateral proptosis n Direction of proptosis (Axial & nonaxial) n The color of the eyelids n Pulsations n
 n Causes: 1. Dysthyroid ophthalmopathy (orbitopathy) or endocrinal exophthalmos Tumors")
Axial Proptosis (Straight forwards) n Causes: 1. Dysthyroid ophthalmopathy (orbitopathy) or endocrinal exophthalmos Tumors within the muscle cone (Intraconal): - Optic nerve glioma - Optic nerve sheath meningioma - Cavernous hemangioma - A-V malformations 2.

Non-axial Proptosis n Lesions outside the muscle cone asymmetric displacement of the globe e. g. deviation of the eye up, down, in, or out in addition to forward n Causes: a. Down & out: mucocele of the frontal sinus Down & in: lacrimal gland tumors Upwards: maxillary carcinoma Downwards: brain meningioma b. c. d.

2. Palpation n n Palpation of the orbital rim may reveal bony erosion or a mass. Palpation should be done gently with the index finger or little finger in the space between the globe and the orbital rim. Notice consistency, compressibility, fixity, or pulsations of any palpable mass. While performing palpation of the orbit, the degree of tenderness should also be noted. Extremely tender lesions are usually inflammatory in nature.

Masses palpable in the superonasal quadrant of the orbit may be: n Frontal mucocele n Meningocele/encephalocele n Demoid cyst

Masse palpable in the superotemporal quadrant of the orbit may be: n Dermoids n Lacrimal gland tumor n Orbital inflammatory pseudotumor

3. Auscultation in the region of the orbit may be helpful in some cases. n The detection of a bruit should suggest a carotid-cavernous fistula n It is synchronous with the heart n
 n Increaed resistance to retrodisplacement of the globe (retropulsion), suggests the")
4. Compression (Retropulsion) n Increaed resistance to retrodisplacement of the globe (retropulsion), suggests the presence of a retrobulbar mass, but it may also occur with dysthyroid ophthalmopathy.

5. Sensation Examination of sensation in the area supplied by the first and second divisions of trigeminal nerve is important. n Hypoesthesia of the cheek and lip is a typical finding in patients with blow-out fracture because of injury to the infraorbital nerve as it travels through its bony canal inthe orbital floor. n

6. Measurement By: Plastic ruler n Exophthalmometer n

n The generally accepted normal value (between the lateral orbital rim and apex of the cornea) is < 22 mm. n A difference > 2 mm between the 2 eyes is abnormal (suggests proptosis). n Values > 21 mm are usually abnormal.

Forced duction test It is a useful test for distinguishing restrictive ophthalmoplegia from neurogenic ophthalmoplegia. n It is particularly useful for differentiating between a medial wall blow-out fracture with medial rectus entrapment and 6 th cranial nerve palsy. n Negative test neurogenic n Positive test restrictive n
 2. Orbital varices n")
Dynamic properties Rapid change in size 1. Capillary hemangioma (infants) 2. Orbital varices n Pulsations + bruit C-C fistula n Pulsations – bruit 1. Orbital roof defect 2. A-V shunt n

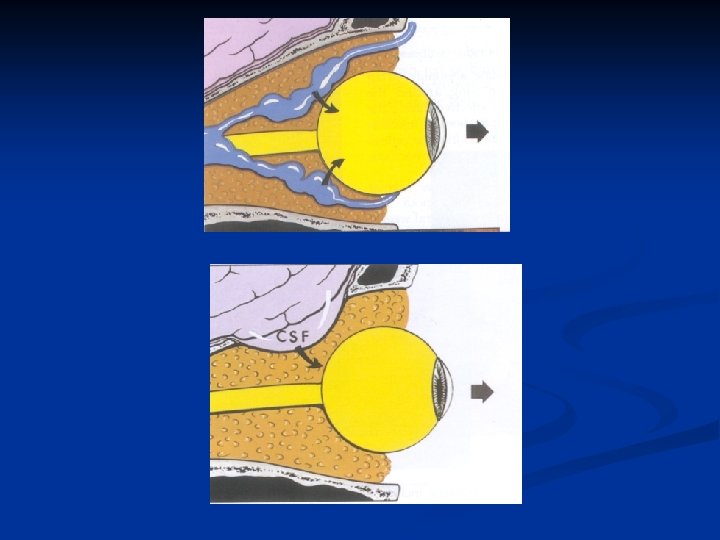
Pulsating Exophthalmos n Causes: 1. A-V shunt or aneurysm: The commonest is C-C fistula Cerebral pulsations due to defect in the orbital roof (congenital, traumatic, iatrogenic) Meningoencephalocele Highly vascular orbital tumor 2. 3. 4.
 Investigations (Orbital Diagnostic Techniques) n Plain X-rays n CT scan n MRI n")
(C) Investigations (Orbital Diagnostic Techniques) n Plain X-rays n CT scan n MRI n US n Biopsy techniques n Pathology

III. Treatment n Depends upon the cause of proptosis e. g. dysthyroid orbitopathy, inflammatory pseudotumor, orbital tumor …etc.
- Slides: 37