Oral Health Care Training Toolkit Managing oral care




 defines personal care")















- Slides: 21
Oral Health Care Training & Toolkit Managing oral care for the frail and elderly in residential homes Sarah Peckham – OHP Co-ordinator Jeni Malpass – Oral Health Educator Solent NHS Trust Dental Service
Solent NHS Trust Dental Services Ø Domiciliary Care Ø Dental Screening for elderly residents Ø Oral Health Promotion Input to Staff Ø Assist care homes with OH Care Plans
Why develop the Training & Toolkit ? Many of us have been in to a residential care home and given “The Talk” Advantages Disadvantages Raises awareness of oral diseases/conditions Difficult to measure outcomes Motivates the care home staff (if only for a short while) Practically impossible to evaluate Improvements in carers’ oral health but not necessarily for residents
What the “new approach” aims to achieve: Carers able to: Demonstrate the use of an oral health assessment tool Use the tool to identify the individual needs of residents Develop and document individual oral health care plans Demonstrate that they can provide the appropriate oral care for clients requiring assistance/support Provide evidence to meet CQC Outcomes
Care Quality Commission Health & Social care Act 2008 (Regulated Activities) defines personal care as: (a) Physical assistance given to a person in connection with……(v) oral care. (b) The prompting, together with supervision, of a person, in relation to the performance of any of the activities listed in paragraph (a).
What we can do for them – meeting outcomes: Outcome 2: Consent to care and treatment Ø Each resident, or an appropriate person acting on their behalf, has to give valid consent for the dental screening Ø The care home can provide evidence of this to help meet this outcome Ø If any dental treatment was required after the screening, valid consent would be sought again, providing the care home with another opportunity to collate evidence
What we can do for them – meeting outcomes: Outcome 4: Care and welfare of people who use the service Ø Staff are trained to devise individualised Oral Health Care Plans for their residents Ø This provides evidence for the CQC that residents’ individual needs and abilities have been taken into account Ø Oral Health Care Plans are based on published research evidence
What we can do for them – meeting outcomes: Outcome 14: Supporting workers Ø Staff who complete the Oral Health Care Training are given a certificate Ø This enable care homes to provide the CQC with evidence that staff have skills relevant to the task Ø Provides evidence that carers are keeping skills up to date in order to continue to carry out their role effectively
What we can do for them – meeting outcomes: Outcome 6: Co-operating with other providers Ø Supporting residents to access other health and social care services - allowing dental staff into the care home and facilitating care at local clinics when appropriate Ø The care home can provide evidence that any information that needs to be shared (e. g. medical history and DOB) is done so in a confidential manner
Oral Health Care Toolkit
The Toolkit contains: • Introduction • Assistance for meeting CQC outcomes • Staff’s role in supporting residents • Introduction to oral health assessments and care plans • Communication tips • Routine and planning • Oral care products • Referral guide • Resources
The Training : • Background knowledge to dental diseases • Choosing appropriate oral health care products
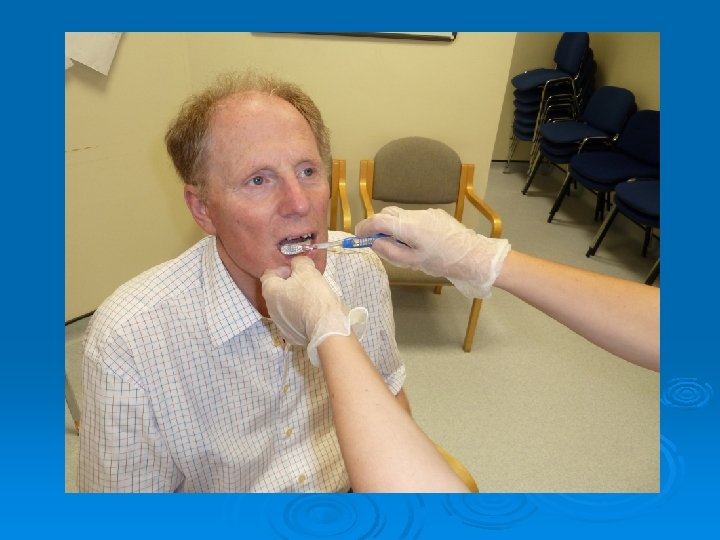
The Training : Hands-on tooth brushing competencies - step-by-step task breakdowns for: • Brushing with a manual tooth brush • Brushing with a powered tooth brush • Denture care
Brushing someone else’s teeth with a manual tooth brush. Task Break Down. 1. Gather items for tooth brushing. 2. Squeeze a pea sized blob of toothpaste on to the toothbrush. 3. Ask the resident to relax their lips and cheeks. 4. Work from the front of the mouth to the back. 5. Concentrate your brushing on one or two teeth at a time. 6. Position the bristles of the toothbrush on the part of the tooth where the gums and teeth meet and brush using a gentle, methodical approach. 7. Brush all surfaces of each tooth systematically. 8. Be aware of any loose teeth and brush with care. 9. Don’t avoid brushing if you notice bleeding – gently massage the gums with the bristles of the brush using circular motions. 10. If the resident wishes to spit after brushing, let them do so. It is not necessary for the resident to rinse. The resident can drink a glass of water if it is safe to do so. 11. If it is through the day replace any partial dentures and pat dry the lips 12. If it is the evening store dentures safely in a denture pot with water.
The Training : Oral health assessments and care plans
The Training : Oral health assessments and care plans
The Training : Routine and timing: • Ideally oral care should be carried out at bedtime and one other time but • Realistically – often carried out in morning only • May be due to lack of staff, lack of time • Maintaining consistent daily oral hygiene helps with residents’ cooperation Communication between carer and resident should: Be at a level of understanding appropriate to the resident Be delivered in a calm and relaxed manner
Southampton University “Healthy Conversations” -a framework for behaviour change brief interventions • techniques to allow people to find solutions to problems • uses open “discovery” questions • “How” • “What”
Further resources British Society of Gerodontology training resources for carers: http: //www. gerodontology. com/BSG-OH-RESOURCE-July 26 -2012. pdf Jeni Malpass jennifer. malpass@solent. nhs. uk Sarah Peckham sarah. peckham@solent. nhs. uk
Thank you for listening. Any questions?