Ora Paltiel MD MSc Braun School of Public

Ora Paltiel, MD, MSc Braun School of Public Health & Community Medicine Hebrew University of Jerusalem Hadassah Medical Organization Israel

Epidemiological Reasoning Using Cancer Statistics Or, how to use descriptive statistics to raise hypotheses

Issues to be discussed Validity of data • Reporting • Confounding • Effect modification Using Descriptive Data • Burden of Disease • Planning • Hypothesis raising • Measuring progress

What are the objectives of epidemiology? 1. To determine the extent of disease (states of health) and/or behaviors in the community. 2. To identify the etiology or the cause/s of a disease and the risk factors - that is, factors that increase a person’s risk for a disease. 3. To study the natural history and prognosis of disease.

Objectives of epidemiology 4. To evaluate new preventive and therapeutic measures and new modes of health care delivery. 5. To provide the foundation for developing public policy and regulatory decisions relating to public health problems.
, Atlanta, Georgia,")
“When we measure, we know better” - Center for Disease Control (CDC), Atlanta, Georgia, USA

The epidemiological tool-box

Kaposi sarcoma in New York

The context of disease reporting

Lowest cancer death rate In the Former Yugoslav Republic of Macedonia, only 6 people per 100, 000 of population die from cancer each year

Lifetime risk of developing breast cancer, 1940 -1987

Lifetime risk of developing breast cancer, 1940 -1987 cont’d YEARONE IN…. 194020 195015 196014 197013 198011 1987 9 Source: American Cancer Society, 1991

Descriptive epidemiology - hypothesis raising rarely provides enough evidence for causation Person: characteristics for study include: • Age • Gender • Religion • Marital status • Ethnicity • Occupation • Socio-economic class • Heredity vs. Environment

Age-specific rates of Breast Cancer Mortality

Population Pyramids 1998 Russian Federation Israel

Trends of Cervical Cancer Mortality in Europe and North America
 per 100 000 women in")
Age-standardized cervical cancer death rates (and 95% confidence intervals) per 100 000 women in urban Canada by neighbourhood income quintile from 1971 to 1996. Q 1 = richest Q 5 = poorest.

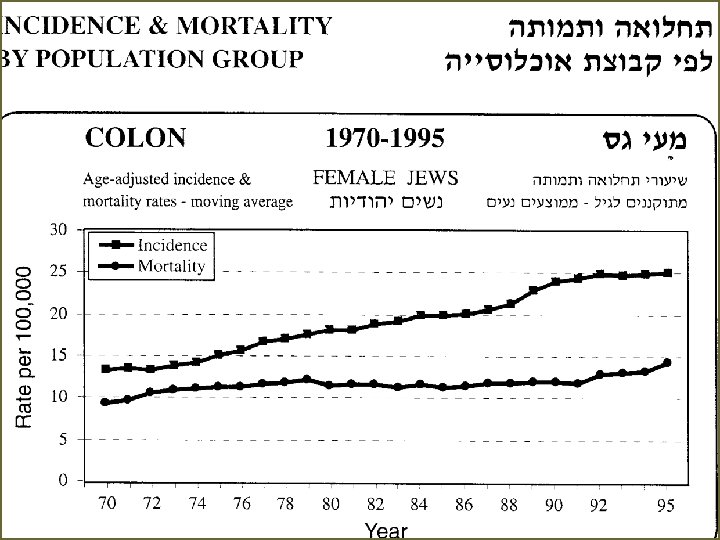
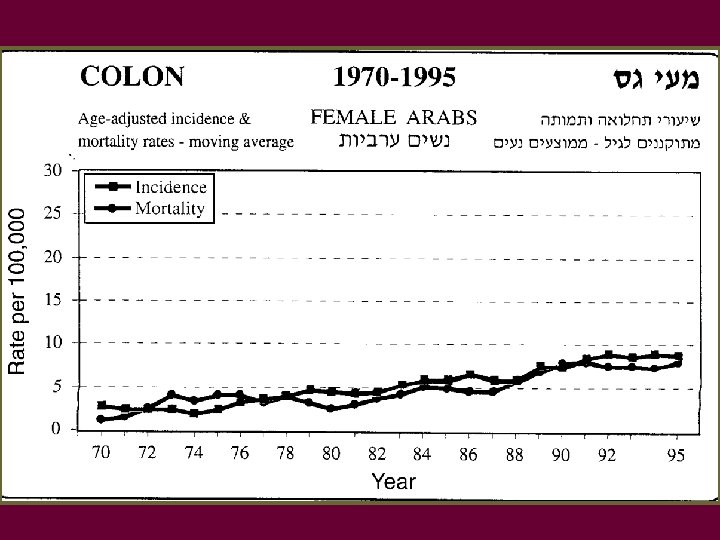
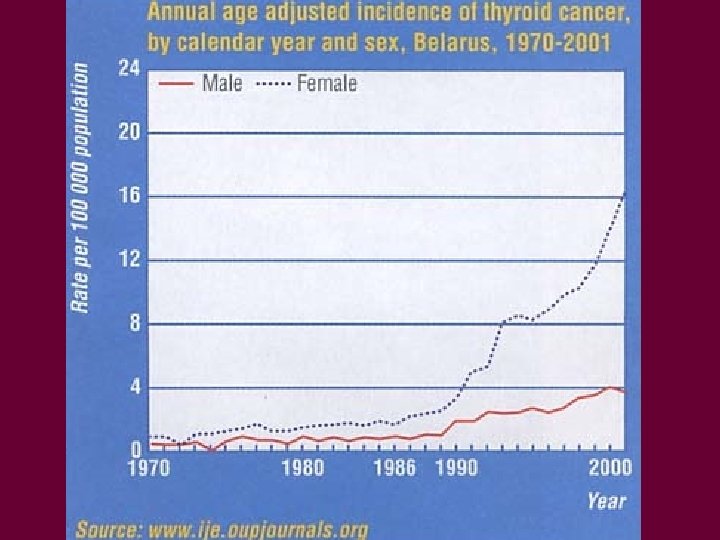
Place and time Time trends - raise hypotheses regarding environmental factors or results of medical care Geographic variation - on small + large scale, environmental genetic factors Study of migrants: important for separating environmental from genetic factors

Numbers of cases of cancer at 16 anatomical sites in developed and in developing countries, with relative ranks

Lung Cancer Mortality for Women 1998, ASR/100000

Lung Cancer Mortality for men 1998, ASR/100000

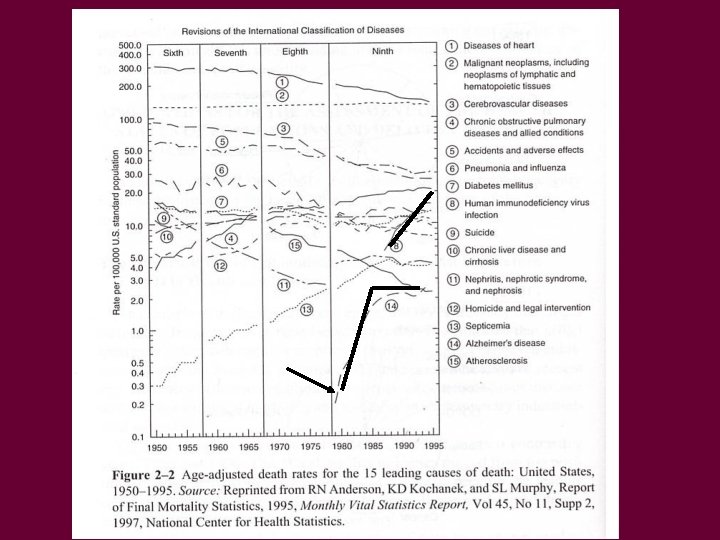
Age-adjusted cancer death rates, males by site, US, 1930 -1996

Age-adjusted cancer death rates, females by site, US, 1930 -1996

Estimated annual percent changes in mortality from all types of cancer in the US over 2 periods 19731990 and 1991 -1995, according to age group

Place and time cont’d Japanese colon cancer incidence: High Intermediate Low Japan Hawaii California - rate is affected by age at immigration - for breast cancer: 2 generations required for rate
 Different reporting 2) Different diagnostic criteria 3) Migrants are")
Biases in migrant studies 1) Different reporting 2) Different diagnostic criteria 3) Migrants are selected group

Where does evidence come from? Clinical observation Descriptive data Hypothesis raising

Clinical Descriptive observation data Analytical studies Hypothesis raising Hypothesis testing
- Slides: 32