Optional IVC Filters Indications for Placement and Retrieval















 Filters: Initial Communication: Risk of Adverse Events with Long")

- Slides: 35
Optional IVC Filters: Indications for Placement and Retrieval Adam J. Doyle, M. D. Assistant Professor of Surgery Division of Vascular Surgery University of Rochester Medical Center
No Disclosures
Objectives • Review indications for placement • Review indications for removal • Suggestions for surveillance of IVC filters that cannot be removed via endovascular techniques
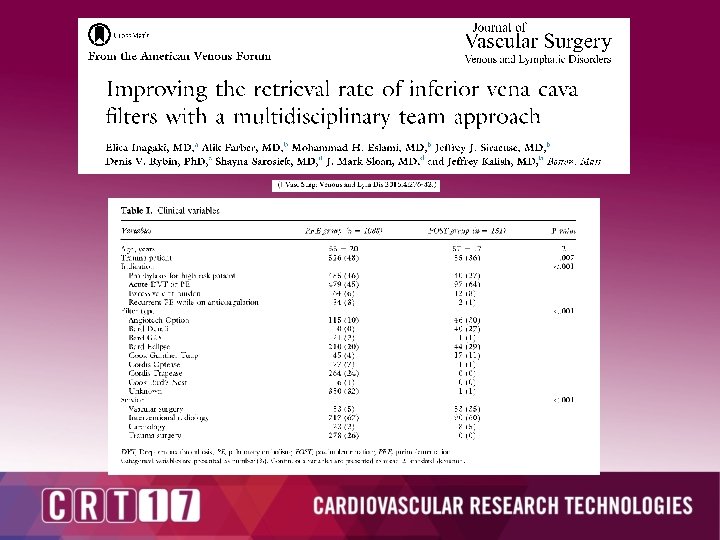
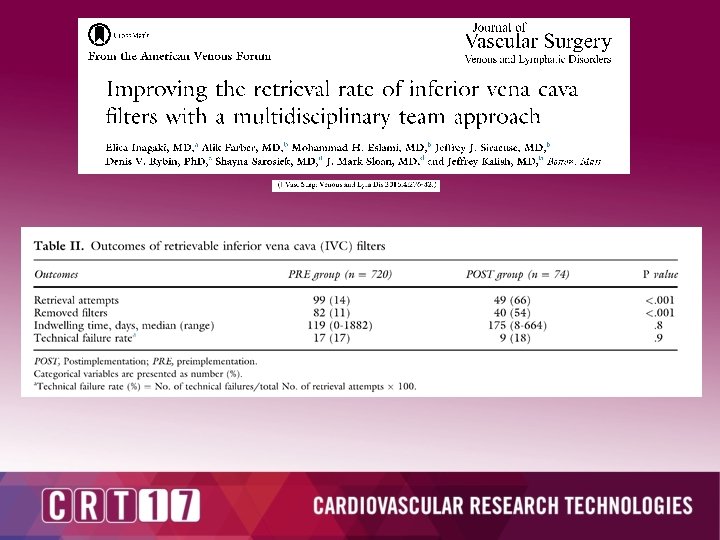
The High Risk Trauma Patient • < 25% of Patients had IVC filters retrieved
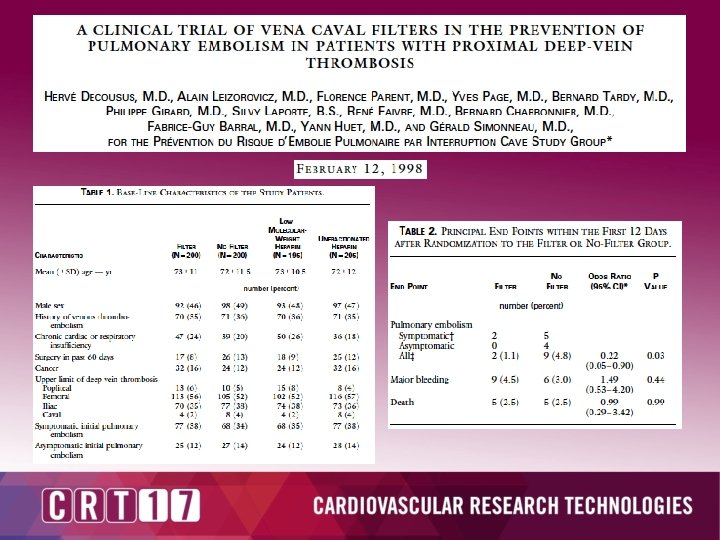
But one more PE might kill the patient. . . • * • mm
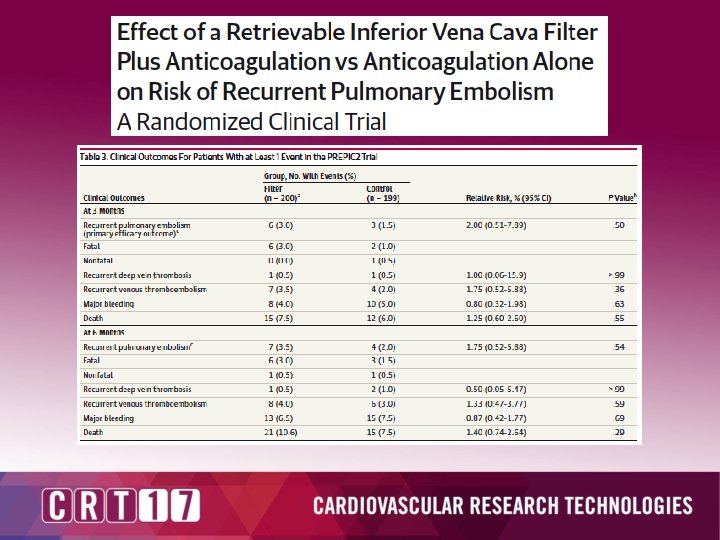
• - Randomized high risk DVT/PE patients to anticoagulation alone vs anticoagulation + IVCF – Age > 75 – Active CA – Severe cardiopulmory disease – CVA with paralysis – Iliocaval DVT – Signs of RV dysfunction or MI
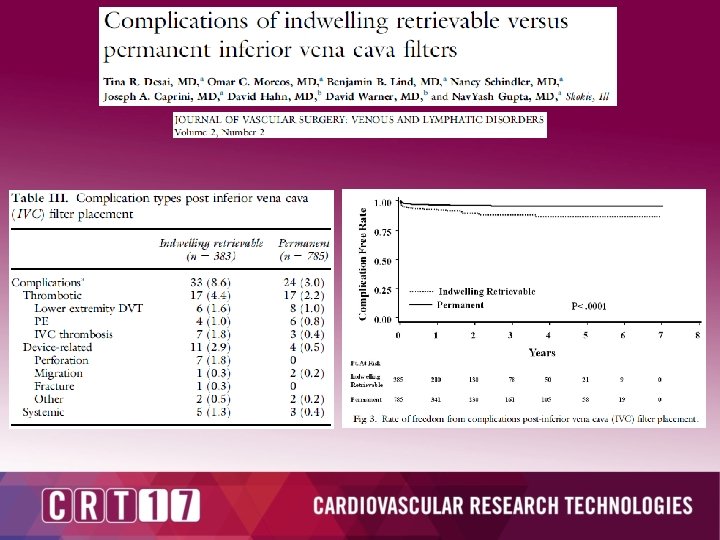
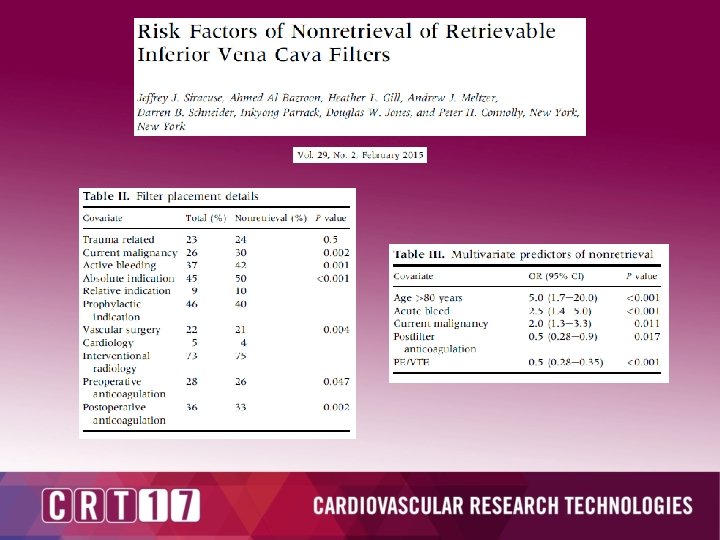
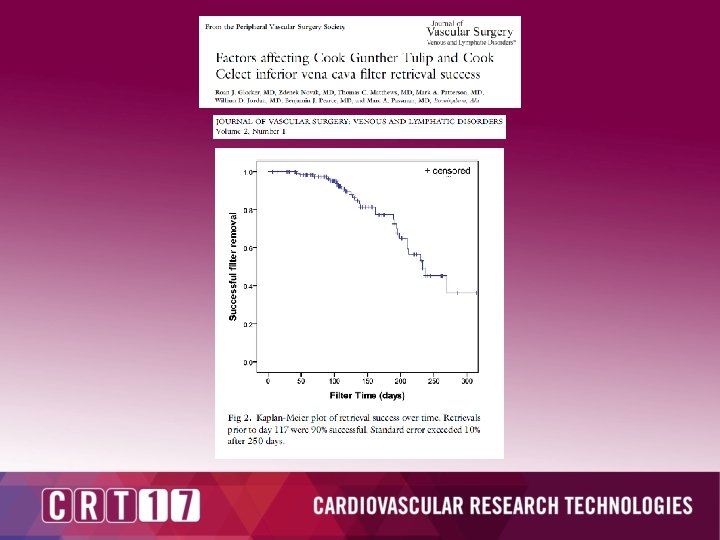
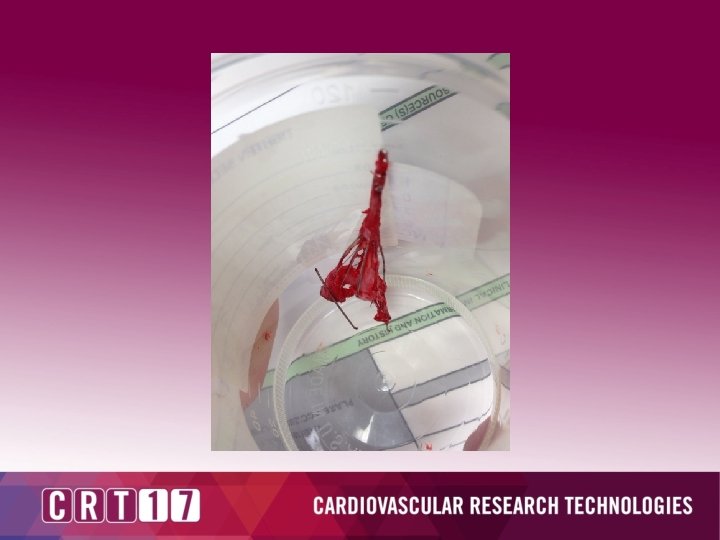
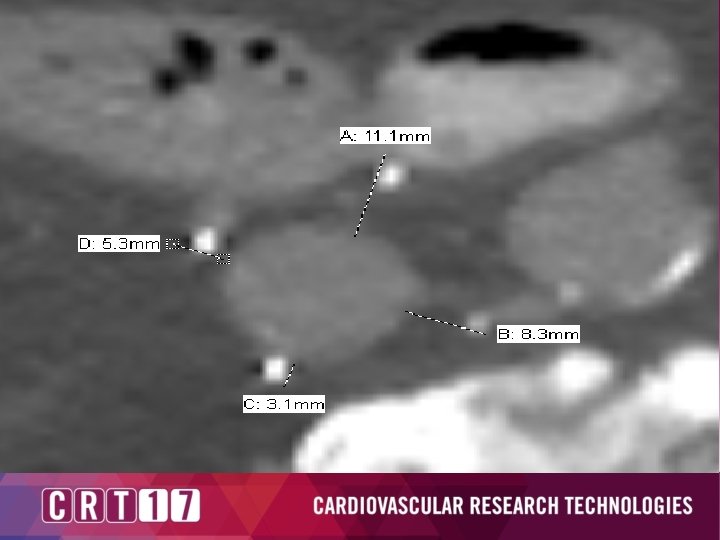
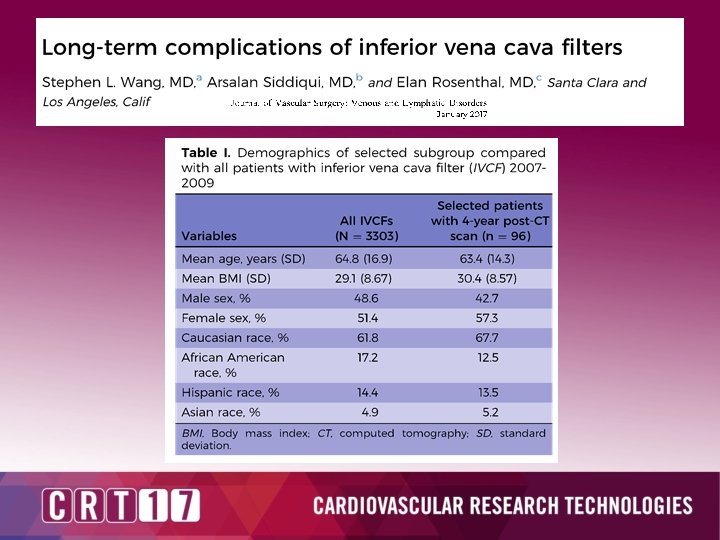
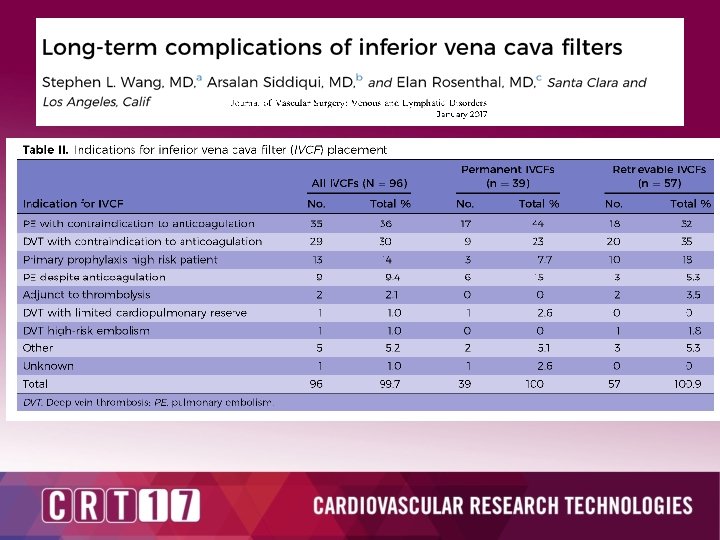
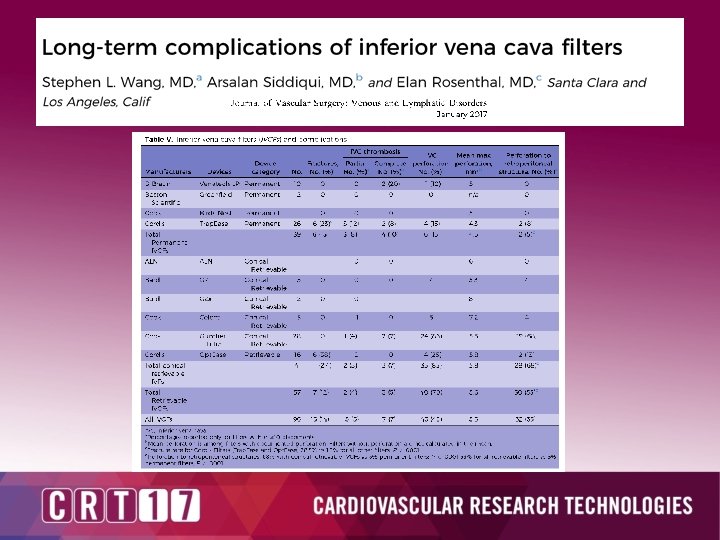
Device Related Complications
Device Related Complications
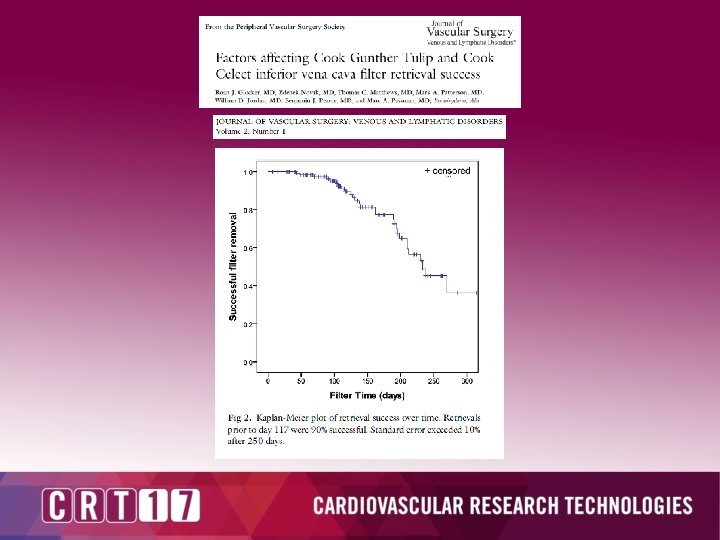
Cook’s CIVC trial which has yet to be published: https: //www. clinicaltrials. gov/ct 2/show/NCT 02046096 This prospective, multicenter, single-arm clinical study will further evaluate the safety and effectiveness of specifically, the Günther Tulip Vena Cava Filter and Cook Celect Vena Cava Filters in patients in need of temporary or permanent IVC filter placement for the prevention of pulmonary embolism.
What is the evidence and what are the indications?
Chest Guidelines
Chest Guidelines
Chest Guidelines
FDA: Inferior Vena Cava (IVC) Filters: Initial Communication: Risk of Adverse Events with Long Term Use. 2010 “If a patient has a retrievable IVC filter that should be removed based on his or her individual risk/benefit profile, the primary care physician and/or those providing ongoing patient care should refer the patient for IVC filter removal when feasible and clinically indicated. ”
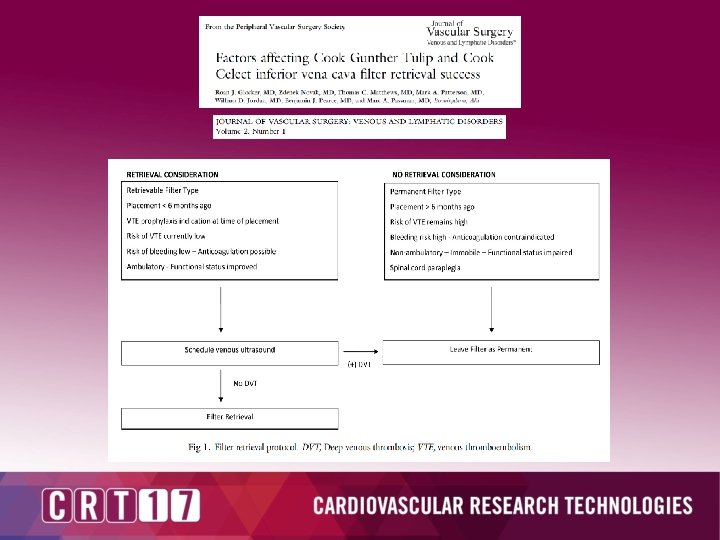
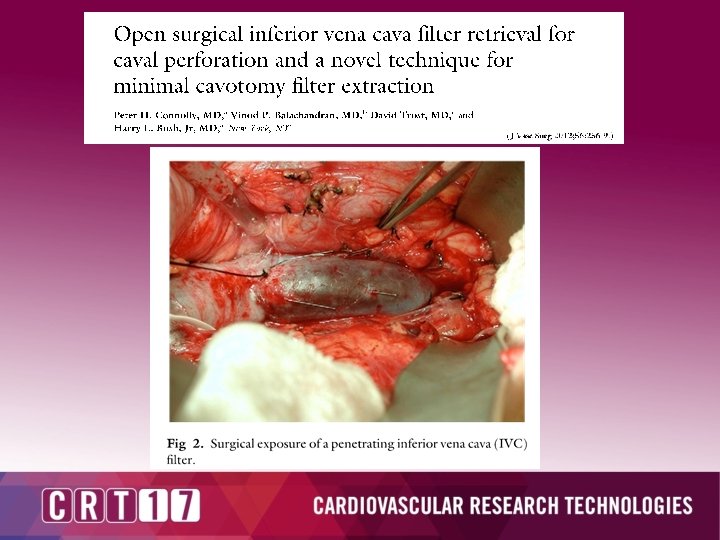
Take Home Points • IVC Filters are an effective tool when used correctly – Indications for placement: • Acute DVT or PE with contraindication/intolerance of therapeutic anticoagulation • Recurrent PE while on therapeutic anticoagulation • Consider the use of permanent IVC filter given lower rates of device related complications if it is unlikely the filter will be removed • Patients should be started on therapeutic anticoagulation as soon as able after IVC filter placement • Attempt removal of all temporary filters as soon as possible • Consider surveillance imaging of all IVC filters to assess for device related complications • Consider open surgical removal of IVC filters in patients with complications