OPIOID TOXICITY AND SPINAL ANALGESIA By Jennifer Gray

OPIOID TOXICITY AND SPINAL ANALGESIA By Jennifer Gray Specialist Clinical Pharmacist Neurosurgery, Pain and Palliative Care Ninewells Hospital 24/09/18

Opioid Toxicity

Signs of Opioid Toxicity �Respiratory Depression �Decreased level of consciousness �Pin point pupils �Seizures �Muscle spasms

Strategies to avoid opioid toxicity �Opioid avoidance/sparing �Utilise non-pharmacological interventions �Utilise non-opioid medications �Opioid rotation – attempt to find right drug �Spinal analgesia �Other interventions �Nerve blocks �Neuro-ablative procedures e. g. Cordotomy

Background �Intrathecal Drug Delivery is a method of giving medication directly into the spinal cord. �It’s an option when most other treatment options have failed �As the medications are delivered directly into the spinal cord, symptoms can be controlled with much smaller doses than would be required orally �Side effects are reduced �It is an unlicensed product

The Patient �Patient requires to be relatively fit prior to procedure (e. g. no infections and blood counts satisfactory) �Improvement in pain and quality of life is the end goal �Other Analgesia will be stopped or reduced prior to insertion �Patient is followed up by the chronic pain team every month
 �Pain Consultant(s) �Neurosurgeon �Palliative Pharmacist �Palliative Technician �Aseptic Pharmacist")
The Team �Palliative Care Consultant(s) �Pain Consultant(s) �Neurosurgeon �Palliative Pharmacist �Palliative Technician �Aseptic Pharmacist

Medications Commonly Used �Hydromorphone – Is a potent opioid with increasing intraspinal “off-label” use to treat cancer and nonmalignant pain. Side effects are less common compared to morphine �Clonidine – Is an a 2 Agonist that enhances the analgesic affect of the opioid. It is often effective for neuropathic pain. Side effects include hypotension and sedation �Levobupivicaine /Bupivicaine – Is a sodium channel blocker used as an anaesthetic. Side effects include motor weakness and urinary retention
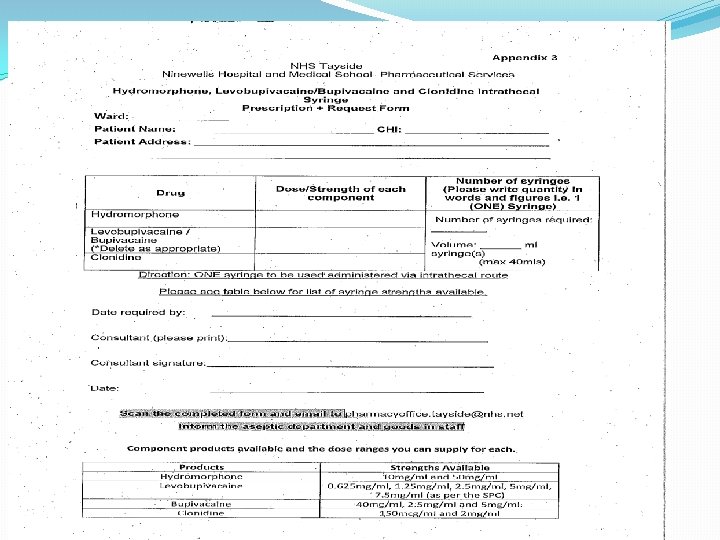

Ordering �Order product from ITH Pharma (company that specialises in the provision of aseptic compounding services for all therapy areas) �Manufacturing and delivery is roughly a one week process �They request a copy of the prescription �Product is labelled for the patient specifically with name and CHI �The cost is around £ 400 per syringe

Thank You Any Questions

Role of the Macmillan Nurse Sharon. Mc. Fadyen Clinical nurse specialists Team leader

4 Pillars of practice �Clinical �Education �Audit �Research

Case Study � 57 year old female �Metastatic Recto-sigmoid tumour �Chemotherapy – no response �Defunctioning loop colostomy �Referred to community macmillan

Home visit �Symptom assessment �Review analgesia-uncontrolled pain �Psychological support �Family support �Refer to OT for aids at home �Financial referral for benefits �Clinic appointment made with specialist palliative care consultant as complex pain

Symptom control clinic �Referred for symptom control-pain: �Back pain worsening despite increasing doses of MST and Gabapentin �Struggled to walk into clinic �Stood for entire clinic review – too painful to sit �Lumbar back pain radiating into buttocks and down the backs of both legs – progressive over a few weeks �Struggling to pass urine

Admitted to Roxburghe House �Admitted directly from symptom control clinic �Commenced high dose dexamethasone �Urgent MRI carried out �Cauda Equina compression due to infiltrating sacral mass � 10 # XRT �Titration of analgesia �On-going neuropathic back and leg pain

Carer Administration of Analgesia �Problems with Absorption �Diamorphine now only effective as required medication �Requiring breakthrough analgesia 3 -5 times per day �Desperate for home but sub/cut as required preclusive �Husband willing to administer �The patient also self administered with her husband drawing up �GP and D/N informed and agreed �Husband taught how to dilute, draw up and inject diamorphine by nurses at Roxburghe House

Home care �Husband drew up diamorphine before leaving for work �Patient self administered as required �Pain well controlled �Patient felt in control �GP visits weekly �Macmillan nurse visits weekly �District nurse involvement �Patient and husband happy with this care plan/self administration of medication

Personal Concerns �no governance around the process. �no guidance around how many injections could be given before informing a member of the medical profession. �no formal medication stock balance to keep the patient and carer safe � no built in review. �discussions around giving the 'last injection' and the psychological implications had not taken place.

Concerns Condition deteriorated and unable to self administer �community nurses were called in a crisis, patient frail and in pain -nurse was asked to administer sub/cut medication, but as there was no prescription for the nurse permitting the nurse to administer the analgesia, and she refused.

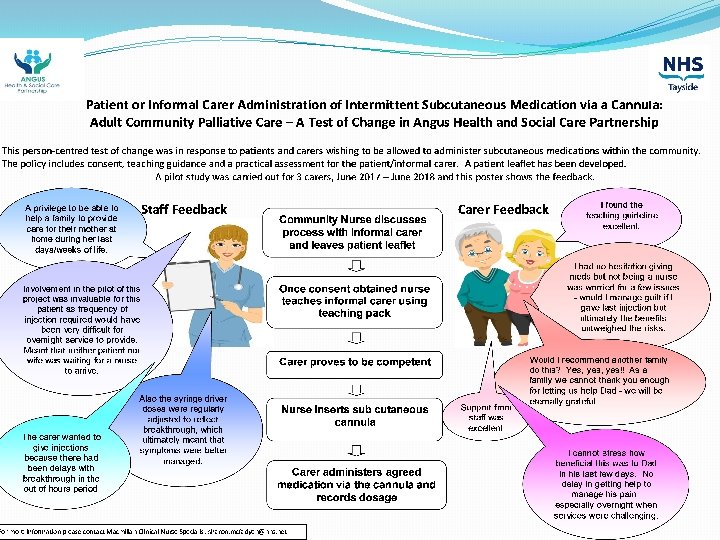
Devised a policy �Patient or informal carer administration of intermittent subcutaneous medication via a cannula: adult community palliative care

Policy �This patient-centred policy is in response to patients and carers wishing to be allowed to administer sub cutaneous medications within the community. �The policy includes consent, teaching guidance and a practical assessment for the patient/informal carer. � A patient leaflet has been developed.

Steps so far �Presented at clinical governance �Test of change with 3 patients �Positive feedback �Devised patient/informal carer leaflet �CLO advised changes to ‘last injection’ paragraph �Poster presentation at MCN forum �ADTC approval

The next steps �MCN endorsement �GP sub committee �Clinical quality forum CQF

Thank you �Sharon Mc. Fadyen �Community Macmillan Clinical Nurse Specialist

Conclusion Increasing pharmacists’ awareness about patient perspectives of barriers to communication with palliative care patients may assist in improving access to medicines information support.

Palliative Care Experiences of Community Pharmacy Alison Mac. Robbie Sept 2018

Research Question How do palliative care patients prefer to communicate with community pharmacists with regard to medicines information

Aim Identify palliative care patient perspectives of communication barriers, facilitators & preferences for analgesic medicines information in community pharmacies.

Methodology & Methods �MRC Framework Complexity �Critical Realist Perspective �Inductive �Prospective sample of community based adult palliative care patients �Semi-structured Interviews �Verbatim transcripts �Analysis using a grounded theory approach �Deliberative panel of pharmacists/managers

Ethics �North of Scotland Research Ethics Committee �University of Lancaster Research Ethics Committee

Inclusion & Exclusion Criteria Interviews Inclusion criteria Exclusion criteria Palliative Care Patients for whom the GP or Macmillan Nurse would not be surprised if they were to die in the next 12 months. English speaking 18 years or older With capacity Experiencing symptoms of pain Responsible for managing their own medicines Living in their own home Patients without capacity Patients with learning disabilities Diagnosed with dementia Living in managed care settings such as care homes

Demographics - Interviews � 11 semi-structured interviews in 6 carers were present (6 male, 5 female) �Age rage 48 -87 y � 3 urban, 8 rural � 10 retired, 1 employed �White (10 UK, 1 European) �Educational level ( 4 secondary, 3 GCSE, 2 further education, 2 higher education)

Pharmacy Types �Large Multiples 5 �Small multiples 3 �Independents 3

Uncertainty �Not wanting to take medicines – Fears �Not knowing illness symptoms or medicines effects �Wanting v not-wanting to know side-effects �Medicines confusing �Knowing how to use medicines in context of illness �Conflicting Information
![“You know, so yeah, that’s my basic is that they [medicines] make me ill.](http://slidetodoc.com/presentation_image_h2/8ddc0ed7ba3cac11bed2fb33810b1a63/image-38.jpg "“You know, so yeah, that’s my basic is that they [medicines] make me ill.")
“You know, so yeah, that’s my basic is that they [medicines] make me ill. fear

“I was a bit worried in case I ended up giving him too many. . of the breakthrough tablets…. ”

Lacking information to take part in treatment choices “I think almost before. If you were going onto a drug it would be better to know what’s coming…” �Relying on label and leaflet �Want personalised information �Rarely pharmacist advice �Sourcing information elsewhere
![“so if I’ve ask her [daughter] a question and she doesn’t know the answer,](http://slidetodoc.com/presentation_image_h2/8ddc0ed7ba3cac11bed2fb33810b1a63/image-42.jpg "“so if I’ve ask her [daughter] a question and she doesn’t know the answer,")
“so if I’ve ask her [daughter] a question and she doesn’t know the answer, she’ll find out for me. She’s phoned the GP, she’s phoned the consultant, she’s phoned the department here (hospice). ”
 get")
prior experience seen as retail not health �“Sometimes I don’t think they (pharmacy) get how important it is that you have the medication you know, especially when you live … I know it doesn’t seem like a long way but when I’ve travelled to [town name] to work and then come back, I don’t want to have to go back again you know. If I have to I will but I don’t want to have to. ”
 they don’t even know")
Perceptions – Larger Pharmacies “Whereas again in (multiple pharmacy name) they don’t even know who you are the medication … they’re not going to ask how somebody else is doing, you know. “ and

Perceptions – smaller pharmacies “But no … because I find that [smaller local pharmacy chain] is fine, they’re not over-busy like the big large [multiple pharmacy chain] you go into and I feel it’s just … you’re just a customer in there. But I feel no, you go round there and they’re friendly and they apologise all the time if they’ve to kept you waiting and things like that. ”

Illness barrier to waiting / listening to medicines advice. “Yeah, sometimes you’ve a long … like when you’re not feeling great and you’ve a prescription to pick up, you could be sitting in the chemist 10/20 minutes and when you’re not feeling 100% that feels like two hours. “

professionals - believe don’t need pharmacist “I see the medical people, the, my Macmillan nurse, the clinic and I can phone the doctor and say ‘I, I need a repeat prescription of Paracetamol and Ibuprofen’ or (Macmillan Nurse name) will do it or whoever. So it’s kind of cut out the pharmacy really. “

�“It’s just sometimes eh that you’d like … I can’t find anything at the time exactly, so there is times when you’d like to ask, aye. But eh…. . You canna say he’s just right either. But they’re sat there and they’re [pharmacy] just too busy to bother with you (coughs). ”

Medicines delivered – distancing from pharmacist access “I don’t. . I don’t deal with the pharmacist because …. the prescription just goes through and gets just delivered. So I don’t really. I’ve been in the chem in the shop but I. . I don’t really. No I haven’t but I suppose it would work if you did. ”

Key findings �All participants obtained medicines from a community pharmacy. They identified with being a customer rather than a patient and rarely reported accessing medicines information from this source. �Community pharmacists were reportedly not proactive in offering medicines information about prescription medicines.

Key findings cont �The importance and the nature of relationships with health care professionals (HCP) and their perceived roles, expectations and identities influenced the source of medicines information used by participants. �Participants believed they were expected to selfmanage their consumption of all medicines. �All participants took medicines which were perceived as essential to meet their hopes of reduced pain and improved independent functioning.

Key findings cont. �Participants found medicines confusing and were uncertain around their use. Their concerns potentially impacted upon medicines taking and perception of burdens related to medicines. �Where possible, participants avoided taking medicines because of fears related to prior beliefs and experiences and also concerns for the future.

Influences in medicines information seeking and communication mechanisms outcomes context A Mac. Robbie, 2016

Developed relationships with pharmacists, same environment A Mac. Robbie, 2016

Developed relationships with pharmacists, understanding of pharmacy role in same environment A Mac. Robbie, 2016

Preferences �Written information �Personalised information �What the medicine does �What the expected side-effects are �Can they safely take with other medicines �Want information ahead of prescribing to permit engagement in decision making about medicines taking �Good relationship builds trust �Being treated as a person/individual – respect, follow-up, being taken an interest in
")
Deliberative Panel � 4 participants (2 male/2 female, 30 – 60 years of age) out of potential 13 � 3 declined following 2 initial acceptances � 6 non responders

Process �Presentation of results & questions �Composite anonymous vignettes – facilitated deliberation �Feedback �Prioritisation

Analysis �Thematic �Emergent data from interviews and literature review synthesised
 �Minimising environmental")
Output �Lack of community pharmacy access to information (electronic, MDT communications, diagnoses) �Minimising environmental barriers – use of consultation room, the term ‘counter’ �Building relationships – use waiting time �Delivering a tangible role which is seen and understood by patients and healthcare professionals

Implementation within control of community pharmacists Access during out of hours period to Emergency Care Summary Medication record /Diagnosis/ Understanding of palliative care condition Implementation requiring involvement of resources external to community pharmacy Second pharmacist in each pharmacy to enable more time to spend with each patient – requires finance Relationship building with primary care team Knowing what pharmacy information is relevant to GP/District Nurse (DN) Access to patient records Pharmacist able to add to patient’s health record Regular use of consultation room for all patient contacts Promotes professional role Formalised pharmacist link to GP practice – Referral pathways – Information sharing bi-directional ( automatic and timeous) Recognised the validated level of training of pharmacy assistant Wide healthcare skills and upskill appropriately Pharmacist routinely included in clinical communications, from all primary and secondary care sources, which impact on and concern patients’ medicines Relationship building with patients Seeking to know the context of patient, their families and their social setting Have sufficient trained support staff to enable pharmacist to spend time with patients Requires finance Pharmacist – be the first point of contact for patients presenting prescriptions to the pharmacy Can carry out clinical check and counsel patient whilst support staff carry out technical dispensing roles Health Board Contract for professional community pharmaceutical services which recognises and remunerates appropriately for responsibility Continuity of pharmacist staff, relationship building with patients Better trained pharmacy assistant staff Triage: to recognise triggers, ‘antennae’ , to identify patient to pharmacist earlier Better trained delivery drivers Payment for responsibility for pharmacy assistant staff (i. e. more than supermarket for stacking shelves) standards and pay commensurate for services (retain assistant staff , promote career structure) Encourage patients to always use the same community pharmacy Structured and agreed salaries for locum pharmacists. Shift from individualised terms which have reduced salary and devalued role – Need to increase recruitment for rural areas Change terminology/environment around community pharmacy to promote professional role rather than retail environment e. g. ‘counter staff’ to pharmacy assistant staff Health and social care IT systems interfacing effectively with each other Register patients with the same community pharmacy (similar system to GPs for temporary holiday registration etc. )

Limitations of research �Patient self-report �Memory �Small sample �Uni-professsional deliberative panel

Rhetoric �Ask your pharmacist

Macmillan Palliative Care Rural Pharmacist Practitioner Skye & Lochalsh Dr Alison Mac. Robbie

3 year project Objectives: • Develop community pharmacy capacity to effectively, efficiently and safely support the needs of those in this rural community with palliative care needs regardless of care setting • Improve service provision/co-ordination ensuring opportunities are developed for training & peer support • Provide quality information to support practice

Service Gaps �Education � updates on medicines and how they are used �treatment options & formulations �for whole team (include carers) �legal issues for CD scripts �Pharmacy not recognised as source of clinical or medicines supply issues (want to feel empowered) �Dispelling opioid myths for patients �Supplies issues/delays with specials

Service Gaps �Stigma of placing patients on PC register in a small community �Need for better links between isolated dispensing practices & pharmacies �Integration of pharmacist into MDT team

Role �Provide specialist advice for healthcare professionals on palliative drugs. �Influence and monitor the management of medicines in all settings. �Provide a general pharmacy presence in community hospitals, care homes and dispensing practices. �Act as a link between healthcare professionals and organisations/resources.

Role cont. �Facilitate and/or provide training opportunities for staff. �Act as a point of contact and advice directly for patients with palliative needs.

Ask 3 Each time you talk to your pharmacist, doctor or nurse about medicines, ask these questions 1. What does this medicine do? 2. What do I need to do? 3. Why is it important for me to do this?

Interface – Medicines support needs Medicines Support Needs Information If admitted to hospital, please share this card with the staff looking after you. (please tick) ¨ I have my medicines provided in a blister pack (MDS/Dosset box) from my community pharmacist ¨ I have a chart provided from my pharmacy to help me with my Medicines ¨ I have care at home support with my medicines (level 3/managed support) ¨ I have other support needs with my medicines (please state) To hospital staff: please contact my community pharmacist (details over) to advise of hospital admission/discharge to assist medicines reconciliation and for continuity of medicines related needs. Patient name…………………… CHI………………. Date…………

Patient/Carer Support �Teach back tools �Drop-in clinics �‘Home’ visits �Search the health literacy place �http: //www. healthliteracyplace. org. uk/

Proposed Model
/ Annual")
�Challenges Year 3 - IT access processes - Time for publicity (award events)/ Annual leave - Impact of prescribing clinics �Still evaluating data – ask 3 /interface card audits �Capturing quality impact on dispensing practice staff (anonymity)

Year 3 - Sustainability �Transition of aspects to Pharmaceutical Palliative Care Model Scheme �CPs now integrated into GSF meetings �Good communication across settings �Patient/Carer continued request for information from community pharmacy �Informal availability and access to MRPP – visibility and focus

Fifty reasons to love your palliative care pharmacist. Walker KA, Scarpaci L, Mc. Pherson ML. https: //www. ncbi. nlm. nih. gov/pubmed/20508241 Am J Hosp Palliat Care. 2010 Dec; 27(8): 511 -3. doi: 10. 1177/1049909110371096. Epub 2010 May 27. Pharmacists have much to offer in caring for patients with an advanced illness. To celebrate the role of pharmacists in palliative care, we wanted to share 50 excellent reasons to love your pharmacist. This list was compiled by 3 pharmacists specializing in end-of-life care spanning from inpatient palliative care to home-based hospice. Our goal is to increase awareness among other hospice and palliative care practitioners by recognizing the skills pharmacists contribute in caring for patients at the end of life. We divided the list into categories: provision of pharmaceuticals, optimizing medication regimens, education and drug information, patient safety, and administration/formulary management.

Conclusion Increasing pharmacists’ awareness about patient perspectives of barriers to communication with palliative care patients may assist in improving access to medicines information support.

Macmillan Palliative ANP Role and Case Study Dee Cameron and Gill Tomison September 2018

Cornhill Macmillan Centre

The Advanced Practice Definition 1 ANPs are experienced and highly educated registered nurses who manage the complete clinical care of their patients, not focusing on any sole condition. ANPs have advanced level capability across the 4 pillars of practice: Clinical Practice, Facilitation of Learning, Leadership, Evidence, Research and Development. (Scottish Government 2017)

Definition 2 Advanced practice is a level of practice, rather than a type or specialty of practice. Advanced practitioners are educated at masters level in advanced practice and are assessed as competent in practice, using expert knowledge and skills. They have the freedom and authority to act, making autonomous decisions in the assessment, diagnosis and treatment of patients. (RCN 2018)

RCN

4 Pillars of Practice �Clinical practice �Leadership �Facilitation of Learning �Evidence of research and development.
.")
Clinical Practice �Two f/t Palliative ANPs and one f/t trainee ANP (23 month secondment). �Working within the Medical team (FY 2, Specialty Doctors [x 3], GP registrar, SP 3 GP Trainee and Palliative Medicine Consultants [x 2 p/t]). �IPU, HPCT and Day Services. �Participating on the duty rota, including weekends, carry the bleep for Special Palliative Care.

Clinical Practice – Core Competencies �Comprehensive History Taking �Clinical Assessment �Differential Diagnosis �Investigation �Treatment �Admission, Discharge and Referral.

Leadership �Senior Nurse – Role model; support to colleagues across service; SCN/CNS/ANP meets. �Non Medical Prescribing – In-house lead, NMPx audit, meets and representation at Tayside Group. �Policy, Guideline and Protocol development. �Service Development – identify and initiate improvements. �PNF and ANMAC. �Clinical Supervisors – inc. RRR’s, 1: 1’s.

Facilitation of Learning �In-House – Lunch &Learn, staff, Journal Club, CSCI. �Mentorship – Trainee ANP role. �GPST 3, Medical Students & FY 2 – during placement and more formally in teaching blocks. �Dundee University – Accountability for Clinical Skills Module, Advanced Practice. �Role Shadowing Opportunities. �Bleep – Consultative advisory & educational role.

Research & Development �Audits/Evaluations – NMPx, PPC, ANP role, education, HNA etc. �Ongoing review of the ANP role - Consideration of new ways of working/service developments i. e. IV interventions in Day Care inc. blood authorisation, biphosphonate therapy; Triage/Coordination role; Out reach care symptom control; Education (Care Homes & Community Hospitals). �Enhancement of Senior Nursing role - role model, expert practice. �Student Nurse Teaching – Opportunities for advanced practice.

Non Medical Prescribing Role o Daily prescriptions of medicines for pain & symptom control management, including controlled drugs and CSCI’s. o Completion of electronic discharge and pass prescription’s. o Provision of advice to other Health professionals in primary and secondary care (usually via the bleep). o Off-label prescribing.

Case Studies 1. ANP – During weekend working: - �Elderly gentleman with metastatic lung ca; ceiling of care – ward based measures. �On MST 30 mg BD. Due to increasing pain, required x 5 doses of breakthrough Oramorph 10 mg/5 mls in previous 24 hours. �On review, noticed to be slightly confused & drowsy with myoclonic jerking evident.

1. Assessment cont/. . . Differential Diagnosis – �Most likely opiate toxicity, however, could also be hypercalcaemia, sepsis (although observations okay). Management Plan �Bloods taken for FBC, U&E, LFT, CRP & Ca+ �Blood result - e. Gfr (60 to 50), otherwise nil significant. �TPAR reviewed - MST discontinued switched to Oxycodone via syringe driver over 24 hours, to be started at 4 pm.

Conclusion �The Case Study demonstrates the ANP role in assessment, diagnosis and treatment in the OOHs. As ANP’s we support complex physical, psychological, spiritual & family needs inc. complex end of life care. �Challenges – Autonomous practice, Non Medical Prescribing, increasing complexity & interventions in Specialist Palliative Care; succession planning. �Opportunities – Service Developments; increasing nursing focus; peer support.

Questions?

Complementary Therapies in Specialist Palliative Care

What are Complementary Therapies and Why? • Treatments used alongside conventional medicine • According to Macmillan, 1 in 3 cancer patients have CTs • Growing evidence base but a clear need for more research • Service feedback/ anecdotal evidence

Complementary Therapy Service

The of palliative care � Toaims achieve best possible quality of life for patients and their families � To affirm life and recognise death as part of a natural process � To integrate the psychological and spiritual aspects of patient care � To offer a support system to enable patients to life as actively as they can for as long as they can � To offer a support system to help family cope during the patients illness and with their own losses � To achieve best possible symptom management

The Value of Complementary Therapies in Palliative Care • To promote relaxation • To alleviate anxiety • To improve mood • To reduce pain • To reduce nausea • To alleviate other symptoms • To alleviate side effects of chemotherapy • To improve sleep and sleep pattern • To reduce stress and tension • To reduce psychological distress • To improve quality of life • To give hope • To offer a sense of control

Therapies currently available �Reiki �Massage �Reflexology �Bowen Therapy �Relaxation Therapy �HEARTS techniques �Aromatherapy and use of oils

Case study 1 • Bob-77 year old gentleman diagnosed with MND in 2015 • Uses Powered Wheelchair • Attends Day Care twice a week • Massage Therapy and MND

‘I am 77 years old with Spinal Stenosis, Myasthenis Gravis and MND. My life revolves around a wheelchair and bed. I am lucky enough to attend Macmillan Day Care two days a week and have been introduced to massage to hand lower arm as well as foot and lower leg. The experience is remarkable. The touch and manipulation is hypnotic and very soothing. The foot massage awakens sensory nerves and reduces my foot swelling. In the morning it is very difficult to get my shoes on but after massage shoes fit on easily. With moody music and sensory stimulation the whole experience calming and reflective I would love to have it everyday. ’ Bob, May 2017

Case study 2 • Anne-67 year old lady with severe COPD • LTOT • Lives alone • High anxiety component
 � ‘you")
Patient feedback � ‘it was lovely and made me fall asleep’ (massage) � ‘you made me forget about my pain for a while’ (massage) � ‘I slept the whole night I was so relaxed’(Reiki) � ‘I have never had a massage before and I really loved it’ (massage) � ‘My neck feels less stiff and painful now’ (Bowen Therapy) � ‘I was able to forget about things for a while’ (Reiki) � ‘I had more energy after my session, couldn’t believe it!’ (Reflexology)

Spiritual Care? Do you like Stories?






Navigating IDENTITY

Self-Aware Self-Compassion Self-Care Navigating IDENTITY
- Slides: 116