Operative Trauma Conference Ureter and Bladder Injuries Daniel

Operative Trauma Conference Ureter and Bladder Injuries Daniel Pust, MD 01 -11 -2011

Ureteral Injury • account for less than 1% of all genitourinary trauma • penetrating trauma • iatrogenic • blunt (6%)

Diagnostic Work-up • Microscopic Hematuria only present in 70 -80 % • 30 % false negative rate • CT scan and IVP 90 % sensitivity • Intra-op Methylenblue • Retrograde uretrography (post op, iatrogenic) • check drain fluid for creatinine

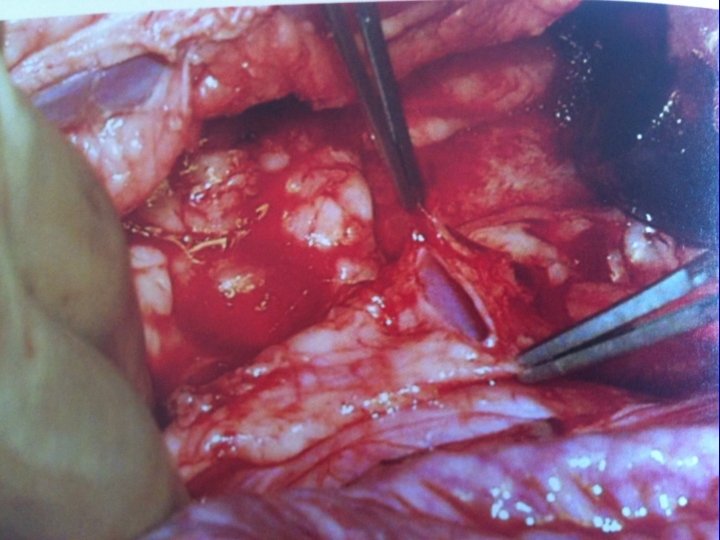
General Operative Principles • Locate ureter at the level of iliac vessels bifurcation • Trace proximal and distal • Avoid devascularization • Resect necrotic segment

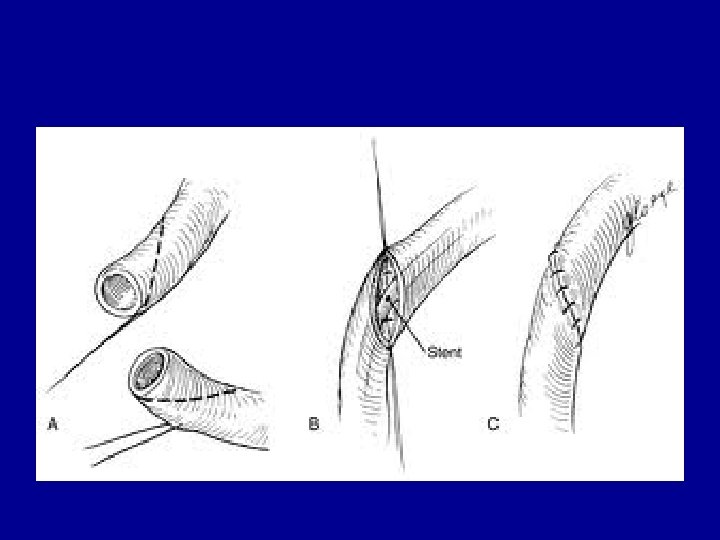
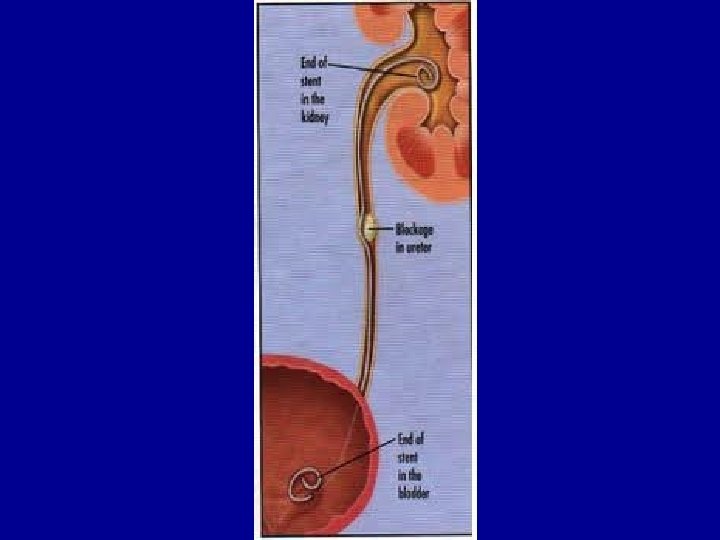
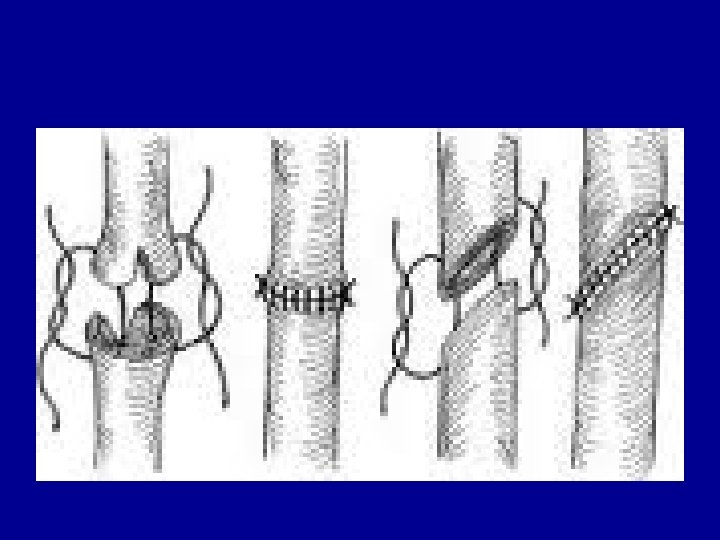
General Operative Principles • Double J stent • 6 or 7 Fr, 22 – 30 cm double J with Glidewire • One end positioned in renal pelvis, second end positioned in bladder • Spatulate ends • Tension free repair

General Operative Principles • • • 4 -0 Vicryl 4 -0 PDS Interrupted Place tissue (omentum) around repair JP-drains
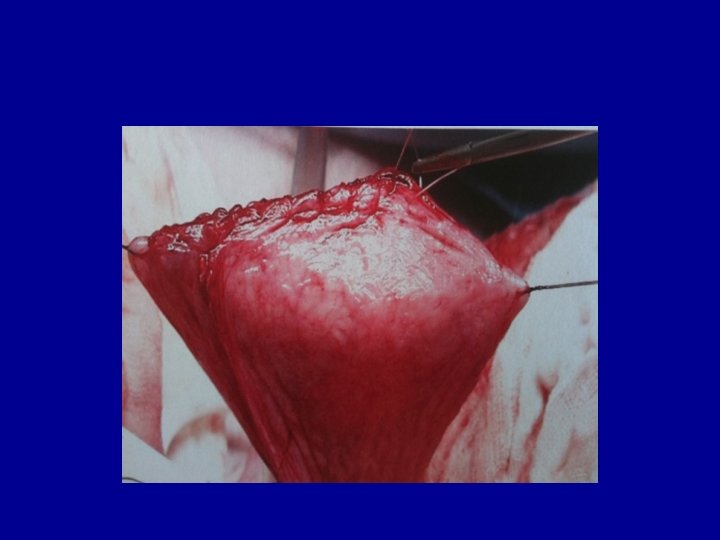
 Boari flap Small")
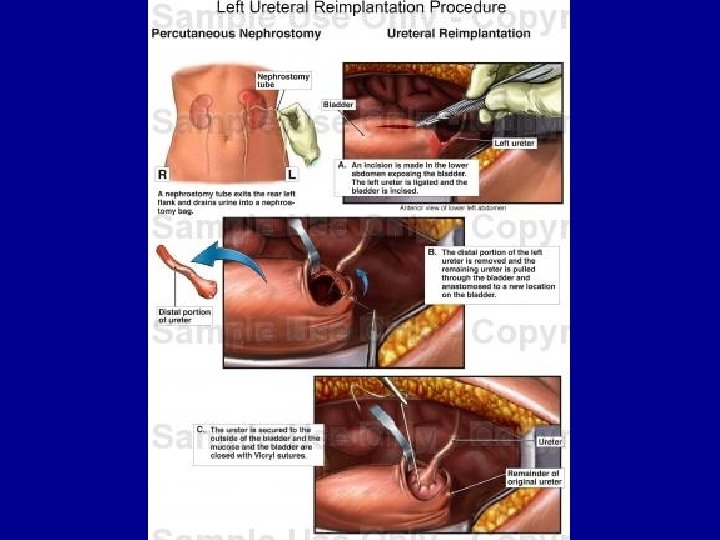
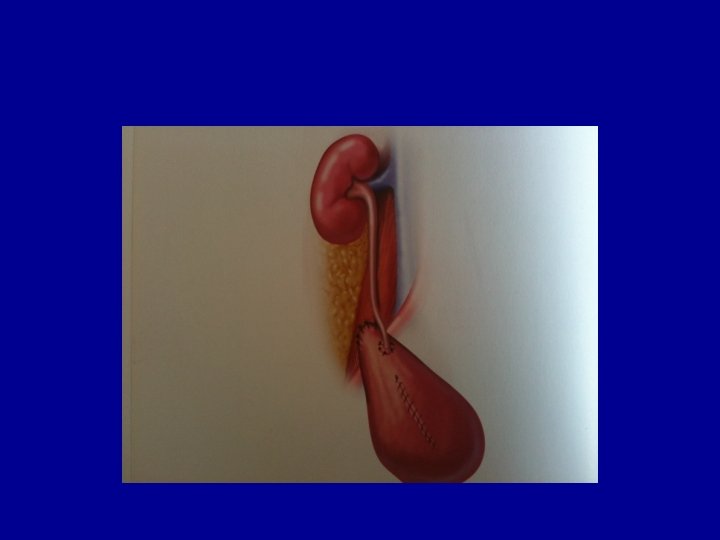
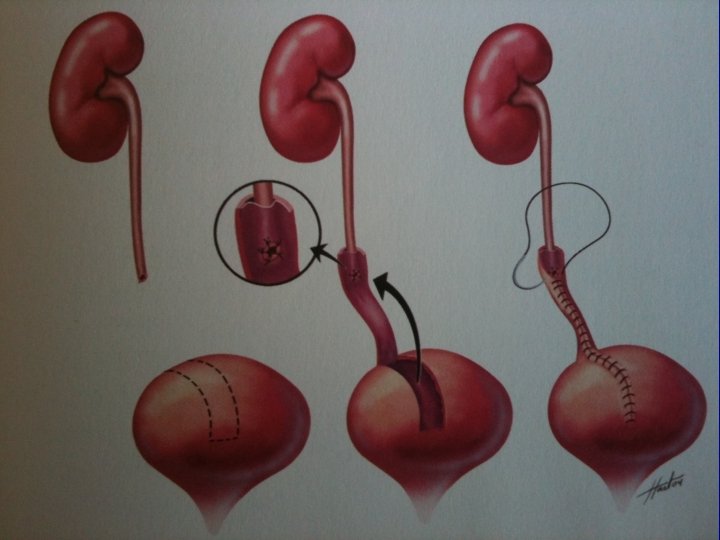
Types of repair • • • Primary anastomosis Ureteroneocystostomy (Psoas Hitch) Boari flap Small bowel interposition Damage control: ligate, delayed percutaneous Nephrostomy tube

DO NOT PERFORM • Transureterostomy • Uretrostomy



Boari flap

Small Bowel Interposition

Bladder Repair • 10 % of pelvic Fx are associated with bladder rupture • 94% have gross hematuria • Dx established by CT cystogram • extraperitoneal 58 % • Intraperitoneal 33 % • combined 10 %



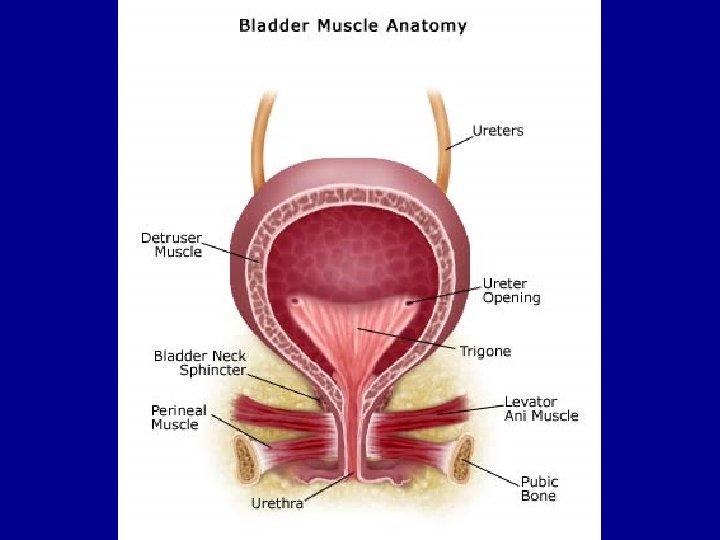
Bladder Repair • Carefully evaluated bladder • If injury present, open dome of the bladder in midline • Inspect bladder from the inside • Locate ureteral orifices and urethra •

• Repair extraperitoneal injuries from the inside • Single layer of interrupted 2 -0 or 3 -0 absorbable • Intraperitoneal rupture is closed with 2 layers of running absorbable suture

• • Foley for 10 -14 days Suprapubic tube is usually not indicated Always place drain Cystogram prior to Foley removal


- Slides: 29