Operation Mobilization Early mobility and decreased ICU stays

Operation Mobilization. Early mobility and decreased ICU stays Presenters: Katelyn Fergan, Paige Garcia, Raquel Hansen, Rebekah Kim, Vania Lara, Ashley Moon, Kendra Teetsal, Daniela Torres & Anna Wang

INTRODUCTION The importance of early mobilization in ICU patients has been understood for decades, since WWII when early mobility was encouraged among injured soldiers to get them back on the battlefield Richard Asher, M. D. describing the bedridden patient: “The blood clotting in his veins, the lime draining from his bones, the scybala stacking up in his colon, the flesh rotting from his seat, the urine leaking from his distended bladder, and the spirit evaporating from his soul”. Evans, B. (2009). Patient mobility in the ICU. Retrieved from www. hanys. org-qualityclincal_operational_initiatives/vapp/docs/patient_mobility_in_the_ICU. pdf
 • Over the past recent decades, developments in life support technologies")
INTRODUCTION (CONT. ) • Over the past recent decades, developments in life support technologies have increased the use of deep sedation and bed rest in ICU patients Prolonged immobilization associated with negative health outcomes such as: neuromuscular dysfunction or ICU-acquired weakness, increased ventilator dependency, decreased bone mass density, decreased peristalsis and increased risk of pressure ulcers and hospital-acquired infections risk among others. increased LOS
 • While some hospitals have early mobilization protocols in place, others")
INTRODUCTION (CONT. ) • While some hospitals have early mobilization protocols in place, others either do not have protocols in place or rely solely on mobility orders. Adherence to both mobility protocols and orders is low in many critical care settings due to competing priorities of care, among other factors. As nurses, we have the most direct contact with patients and are thus most capable of ensuring that early mobilization is implemented among patients.

PICOT In adult ICU patients, hospitalized for any length of time, is early mobilization as compared to immobilization associated with shorter ICU stays?

Summary of Current Practice National Hospitals throughout the country that use early mobilization interventions/protocols have decreased length of stay. Studies conducted in Iowa, North Carolina, and California showed a reduction in hospital stay with implementation of early mobilization. Even with mobility protocols in place they are not always followed. Hospitals without a mobility protocol have less overall mobility of ICU patients and longer ICU stays. �Minimal mobility such as turning, or transferring to a stretcher with no other movements are being performed. Zomorodi, M. , Topley, D. , & Mc. Anaw, M. (2012). Developing a mobility protocol for early mobilization of patients in a surgical/trauma ICU. Critical Care Research and Practice. 2012 1 -10 Doi: 10. 1155/2012/964547
 State/local: Banner University Medical Center Critical Care Early")
Summary of Current Practice (cont. ) State/local: Banner University Medical Center Critical Care Early Mobility Protocol �Not all nurses aware of protocol �ICU nurses stated “we try to ambulate patients as early as possible and often as possible”
 St. Joseph’s Hospital �Activity Per Protocol Order Lacks")
Summary of Current Practice (cont. ) St. Joseph’s Hospital �Activity Per Protocol Order Lacks education and implementation Hogan, C. (2015). Early mobilization in the hospitalized patient. Medical staff newsletter: St. Joseph’s healthcare. Retrieved from: http: //www. stjosephhospital. com/Default. aspx? DN=e 6 d 0 de 38 -0 fc 4 -4 b 3 db 94 b-bde 1 eef 3480 f
 Observation: In local hospitals protocols are not being")
Summary of Current Practice (cont. ) Observation: In local hospitals protocols are not being followed or they are partially carried out. Patients have little to no mobilization or they are fully ambulated with no transition in between. Overall Most protocols follow a similar algorithm � A 3 -4 phase protocol with exclusion criteria Many healthcare members and patients are unaware of mobility protocols and the benefits of early mobilization. Further education and training is required

SYNOPSIS OF CURRENT LITERATURE FINDINGS According to multiple studies, patients who experienced early mobilization protocols in ICUs were shown to have decreased lengths of stay Immobilization leads to longer days on ventilation and lower levels of functionality � 59% of patients who received early mobilization spent less days on mechanical vent. with higher levels of functional independence � The other 35% received usual care with no interventions Usual care (including no mobilization) leads to 6 days on average longer stay Engel, H. J. , Tatebe, S. Alonzo, P. B. , Mustilleand, R. L. , & Rivera, M. J. (2013). Physical therapist-established intensive care unit early mobilization program: quality improvement project for critical care at the University of California San Francisco Medical Center. Journal of the American Physical Therapy Association, 93(7), 975 -985. doi: 10. 2522/ptj. 20110420 Pandullo, S. , Spilman, S. , Smith, J. , Kingery, L. , Pille, S. , Rondinelli, R. , & Sahr, S. (2015). Time for critically ill patients to regain mobility after early mobilization in the intensive care unit and transition to a general inpatient floor. Journal of Critical Care. http: //dx. doi. org/10. 1016/j. jcrc. 2015. 08. 007

SYNOPSIS OF CURRENT LITERATURE FINDINGS Immobilization increases care and time dedicated to patient � More time and resources used More money spent on staff and tools involved in patient care � Re-intubation rate 50% increased with immobilization � 60% increase in hospital-acquired infections when compared to mobile patients In general, immobilization has been proven to be an issue in ICUs � Decreased quality of care � Increased length of stay � Decreased independence of pt upon discharge � Increase in hospital-acquired infections � Increase in pt anxiety and fear related to hospital stay Clark, D. E. , Lowman, J. D. , Griffin, R. L. , Matthews, H. M. , & Reiff, D. A. (2013). Effectiveness of an Early Mobilization Protocol in a Trauma and Burns Intensive Care Unit: A Retrospective Cohort Study. Physical Therapy, 93(2), 186 -196. doi: 10. 2522/ptj. 20110417 Titsworth, W. L. , Correia, T. , Reed, R. , Guin, P. , Archibald, L. , Layon, A. J. , & J. Mocco (2012). The effect of increased mobility on morbidity in the neurointensive care unit. Journal of Neurosurgery, 116(6), 1379 -1388. doi: 0. 3171/2012. 2. JNS 111881

SYNOPSIS OF CURRENT LITERATURE FINDINGS Lord, R. K. , Mayhew, C. R. , Koruplou, R. , Mantheiy, E. C. , Friedman, M. A. , Palmer, J. B. , Needleham, D. M. (2015). ICU early physical rehabilitation programs: Financial modeling of cost savings. Critical Care Medicine, 41(3), 717 -724. doi: 10. 1097/CCM. 0 b 013 e 3182711 de 2

Limitations of Research Articles Small sample sizes Study performed at only one hospital Focus on physical therapy or occupational therapy interventions Specific populations (i. e. neurological)

Strengths of Research Articles Control Groups Cohort study Complicated comorbid conditions Study at least 1 year long Mean age >60 years old Studies from different types of ICUs � Neuro ICU � Medical ICU � Trauma ICU � Surgical ICU

Evidence Based Recommendations In general, research recommends that mobilization should be implemented within 24 hours of admission � Nurses should also follow an appropriate protocol that allows patients progress efficiently Positive results after an early mobilization intervention among patients in the intensive care unit (ICU) � Trauma, burn, neurological, and medical/surgical ICU. Eight out of nine studies associated with shorter ICU stays—ranged from two days to six days Other findings: significant increase in ambulation, increase in discharges, fewer pulmonary and vascular complications, fewer physical therapy referrals, and a decrease in hospital-acquired infections Early mobilization safe and feasible If early mobilization is to be implemented among ICU patients, safety concerns should first be addressed

REFERENCES FOR STRENGTHS, LIMITATIONS, AND RECOMMENDATIONS Clark, D. E. , Lowman, J. D. , Griffin, R. L. , Matthews, H. M. , & Reiff, D. A. (2013). Effectiveness of an Early Mobilization Protocol in a Trauma and Burns Intensive Care Unit: A Retrospective Cohort Study. Physical Therapy, 93(2), 186 -196. doi: 10. 2522/ptj. 20110417 Drolet, A. , De. Juilio, P. , Harkless, S. , Henricks, S. , Kamin, E. , Leddy, E. A. , Williams, S. (2013). Move to improve: The feasibility of using an early mobility protocol to increase ambulation in the intensive and intermediate care settings. Physical Therapy, 93(2), 197 -207. doi: 10. 2522/ptj. 20110400 Engel, H. J. , Tatebe, S. Alonzo, P. B. , Mustilleand, R. L. , & Rivera, M. J. (2013). Physical therapist-established intensive care unit early mobilization program: quality improvement project for critical care at the University of California San Francisco Medical Center. Journal of the American Physical Therapy Association, 93(7), 975 -985. doi: 10. 2522/ptj. 20110420 Klein, K. , Mulkey, M. , Bena, J. F. , Albert, N. M. (2015). Clinical and psychological effects of early mobilization in patients treated in a neurologic ICU: A comparative study. Critical Care Medicine 43(4), p 865– 873 doi: 10. 1097/CCM. 0000000787 Mah, J. M. , Staff, I. , Fichandler, D. , & Butler, K. L. (2013). Resource-efficient mobilization programs in the intensive care unit: who stands to win? The American Journal of Surgery, 206, 488 -493. Retrieved from http: //dx. doi. org/10. 1016/j. amjrug. 2013. 001 Pandullo, S. , Spilman, S. , Smith, J. , Kingery, L. , Pille, S. , Rondinelli, R. , & Sahr, S. (2015). Time for critically ill patients to regain mobility after early mobilization in the intensive care unit and transition to a general inpatient floor. Journal of Critical Care. http: //dx. doi. org/10. 1016/j. jcrc. 2015. 08. 007 Titsworth, W. L. , Correia, T. , Reed, R. , Guin, P. , Archibald, L. , Layon, A. J. , & J. Mocco (2012). The effect of increased mobility on morbidity in the neurointensive care unit. Journal of Neurosurgery, 116(6), 1379 -1388. doi: 0. 3171/2012. 2. JNS 111881 Wang, Y. T. , Haines, T. P. , Ritchie, P. , Walker, C. , Ansell, T. A. , Ryan, D. T. , Lim, P. , Vij, S. , Acs, R. , Fealy, N. , & Skinner, E. H. (2014). Early mobilization on continuous renal replacement therapy is safe and may improve filter life. Critical Care, 18(4), R 161 -R 170. doi: 10. 1186/cc 14001 Witcher, R. , Stoerger, L. , Dzierba, A. L. , Silverstein, A. , Rosengart, A. , Brodie, D. , & Berger, K. (2015). Effect of early mobilization on sedation practices in the neurosciences intensive care unit: A preimplementation and postimplementation evaluation. Journal of Critical Care, (30), 344 -347. Retrieved from http: //zp 9 vv 3 zm 2 k. search. serialssolutions. com/? V=1. 0&sid=Pub. Med: Link. Out&pmid=25573283

ACTION PLAN Create a research informed, nurse-driven mobility protocol A comprehensive protocol will be created using a combination of multiple protocols from different facilities and studies and include specific parameters and instructions for initiating mobility Protocol will be implemented at Banner University Medical Center- Tucson Campus in the medical intensive care unit Implementation will focus on education

BANNER UNIVERSITY MEDICAL CENTER- TUCSON CAMPUS “One thing remains constant: our unwavering commitment to improve clinical quality and efficiency and provide a superior patient care experience by leveraging innovation and technology. ” -Peter S. Fine President and CEO of Banner Health “To make a difference in people's lives through excellent patient care” -Banner Health Mission Statement

TIME LINE September 1, 2015 - October 29, 2016: Research current evidence, develop protocol and plan to implement early ambulation protocol in Banner intensive care units January 1, 2016 - March 15, 2016: Receive approval from unit managers, medical executive committee, intensive care physician teams, and consult with a physical therapist liaison to develop training. March 16, 2016 -March 30, 2016: Four training sessions will occur over two week period; each training session will be 90 minutes and held by a physical therapist. All nurses and PCTs on the medical ICU will be expected to attend one of the four planned training sessions. Employees will be compensated for attending training. April 1, 2016 - August 1, 2016: Implementation of protocol in the medical ICU. August 1, 2016 - September 1, 2016: Evaluation of successfulness of protocol and discussion and plans to implement into the CVICU and trauma/surgical ICU

EDUCATION The protocol will be implemented with education as a primary focus All nurses and PCT’s will be required to attend one 90 minute training session Training sessions will be held over a two week period and staff members will have four date & time options to choose from to attend Staff members will be paid for the mandatory training Training will be led by a physical therapist Staff members will be required to pass (>70%) a comprehension test at the end of training

TRAINING SESSION RNs and PCTs will be educated about the protocol, when to initiate, exclusion criteria, and how to implement into their care Staff will be trained about body mechanics and how to safely ambulate patients How to cluster care to include protocol When to stop mobilization How to plan with patient discharge exercise and mobility
")
“AMBU GURU” The protocol will include the implementation of an Ambulation Guru (Ambu Guru) At the beginning of every shift the charge nurse will assign one nurse the job of “Ambu Guru” This nurse will be expected to remind other staff members throughout the day to utilize “Operation Mobilization” All RNs and PCTs will be trained to be an Ambu Guru at their required training session
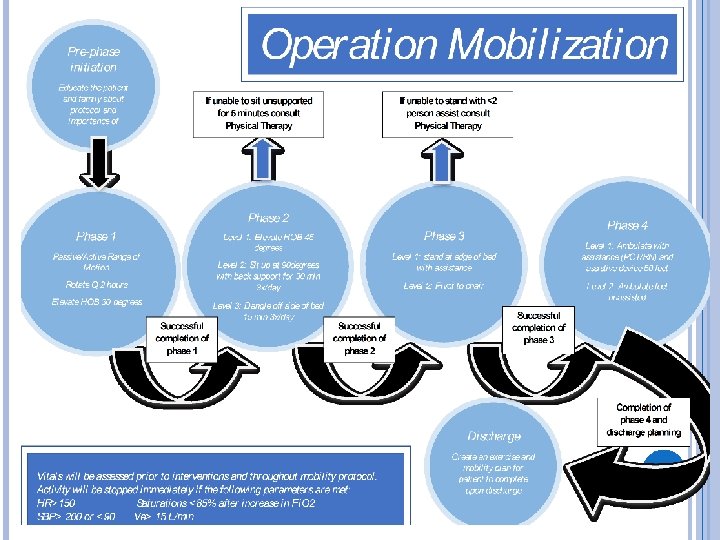

If none of the exclusion criteria is met the nurse may initiate Operation Mobilization Pre-phase initiation Educate the patient and family about protocol and importance of ambulation

Phase 1 Passive/Active Range of Motion Rotate Q 2 hours Elevate HOB 30 degrees

Phase 2 Level 1: Elevate HOB 45 degrees Level 2: Sit up at 90 degrees with back support for 30 min 3 x/day Level 3: Dangle off side of bed 15 min 3 x/day If unable to sit unsupport ed for 5 minutes consult Physical Therapy

Phase 3 Level 1: stand at edge of bed with assistance Level 2: Pivot to chair If unable to stand <2 person assist consult Physical Therapy
 and assistive device 50 feet Level")
Phase 4 Level 1: Ambulate with assistance (PCT/RN) and assistive device 50 feet Level 2: Ambulate 50 feet unassisted

Discharge Create an exercise and mobility plan for patient to complete upon discharge

Vitals will be assessed prior to interventions and throughout mobility protocol. Activity will be stopped immediately if the following parameters are met: HR>150 SBP> 200 or <90 Saturations <85% after increase in Fi. O 2 Ve> 15 L/min

EXCLUSION CRITERIA All patient’s who do not meet exclusion criteria will be started on the mobility protocol within 24 hours of admission to the Medical ICU If a patient meets one of the parameters listed on the exclusion criteria the nurse must obtain physician approval prior to implementing “Operation Mobilization” The nurse will be expected to begin mobility protocol for all patients eligible to receive intervention
 Cerebral spinal fluid (CSF) leak Acute stroke")
EXCLUSION CRITERIA Neurological: Increased intracranial pressure (ICP) Cerebral spinal fluid (CSF) leak Acute stroke within 24 hours Unsecured, ruptured aneurysm Respiratory: Positive end expiratory pressure (PEEP) >12 Fractional expired oxygen (Fi. O 2) >. 8 Minute volume > 15 L/min Hypoxemia (saturation <88%) Tachypnea (respiratory rate > 30 breaths per minute)
 or pulmonary embolism (PE) within 24")
EXCLUSION CRITERIA Circulatory New deep vein thrombosis (DVT) or pulmonary embolism (PE) within 24 hours Unstable arrhythmia within 24 hours New onset chest pain Tachycardia (heart rate >150) Systolic blood pressure (SBP) >200 mm. Hg or <90 mm. Hg Mean arterial pressure (MAP) <60 mm. Hg or >140 mm. Hg Active bleeding

EXCLUSION CRITERIA Musculoskeletal: Ordered bed rest Unstable/acute fractures Hematological: Hemaglobin < 7 g/d. L Platelet count <2, 000 INR > 5. 0 Other: Femoral arterial line Recent hip surgery Transition to comfort care

OPERATION MOBILIZATION PROMOTION Protocol will be posted throughout the unit Patient’s will receive information about protocol upon admission “Ask your nurse about Operation Mobilization” sign will be posted in all patient rooms The assigned “Ambu Guru” will enforce protocol throughout shift and report compliance
 Training PCT Training nurses $30, 000")
Cost Analysis Hiring new PCT ($30, 000 yearly) Training PCT Training nurses $30, 000 yearly salary divide by 12 months= $2, 500/month x 4 months $10, 000 for four months x 10 PCT $11. 63 hourly x 90 min x 22 PCT $34. 32 hourly x 90 min x 50 nurses $100, 000. 00 $383. 79 $2, 574. 00 Trainer (physical therapist) $20. 18 x 9 hours $181. 62 Buying 10 extra walkers $35. 50 x 15 walkers $532. 50 Laminated posters in each room $2. 39 x 24 posters $57. 36 Total: $103, 729. 27
 came out to $63, 750")
COMPARISON Total cost of the resource-efficient mobility program (REMP) came out to $63, 750 Our cost for Operation Mobilization $103, 699. 00 � Will focus on education throughout the protocol � Will focus on nursing aspect applying the protocol with the help of PCT � The hospital will benefit and will save money � Decrease length of hospitalization � Reducing medical complications associated with prolong immobilization Mah, J. M. , Staff, I. , Fichandler, D. , & Butler, K. L. (2013). Resource-efficient mobilization programs in the intensive care unit: who stands to win? The American Journal of Surgery, 206, 488 -493. Retrieved from http: //dx. doi. org/10. 1016/j. amjrug. 2013. 001

COST OF IMMOBILITY 900, 000 patients in the United States each year are affected by deep vein thrombosis (DVT) and pulmonary embolism (PE) in hospital settings. DVT annual estimated cost ranges between $4. 9 to $7. 5 billion and $8. 5 to $19. 8 billion pertains to the annual estimated cost for PE treatment. A total of 28, 953 patients were diagnosed with DVT and 35, 550 patients were diagnosed with PE. Daily cost for the first day of treating a DVT patient was $2, 321, second day $1, 875 and third day $1, 558. For a PE patient, daily cost for the first day was $2, 981, second day $2, 034, and third day was $1, 564. Dasta, J. F. , Pilon, D. , Mody, S. H. , Lopatto, J. , Laliberte, F. , Germain, G. , Bookhart, B. K. , Lefebvre, P. , & Nutescu, E. A. (2014). Daily hospitalization costs in patients with deep vein thrombosis or pulmonary embolism treated with anticoagulant therapy. EJournal of Thrombosis Research Journal. 135, 303 -310. Retrieved from http: //dx. doi. org/10. 1016/j. thromres. 2014. 11. 024

COST OF IMMOBILITY 1 million to 2. 5 million patients develop pressure ulcers annually in the United States ranging from Stage to Stage IV. The cost to treat and heal a pressure ulcer depends on the severity of the pressure ulcer condition. For instance, it can cost hundreds of dollars for Stage I and II pressure ulcers and up to $5, 000 to $151, 700 for Stage III and IV pressure ulcers. Meddings, J. , Reichert, H. , Rogers, M. A. M. , Hofer, T. P. , Mc. Mahon, L. F. , Grazier, K. L. (2015). Under pressure: Financial effect of the hospital-acquired conditions initiative-a statewide analysis of pressure ulcer development and payment. The American Geriatrics Society Journal, 63, 1407 -1412. doi: 10. 1111/jps. 13475
. Patient care technician salary in Tucson, AZ.")
ADDITIONAL REFERENCES FOR COST ANALYSIS Indeed (2015). Patient care technician salary in Tucson, AZ. Retrieved from http: //www. indeed. com/salary? q 1=Patient+Care+Technician&l 1=Tucson%2 C+A Z Payscale: Human capital (2015). Patient care technician salary. Retrieved from http: //www. payscale. com/research/US/Job=Patient_Care_Technician/Hourly_ Rate Payscale: Human capital (2015). Physical therapist salary in Tucson. Retrieved from http: //www. payscale. com/research/US/Job=Physical_Therapist_Assistant/Salar y/fa 2719 cd/Tucson-AZ Salary. Genius (2015). RN salary in Tucson, Arizona. Retrieved from http: //salarygenius. com/az/tucson/salary/rn-salary? p=2 Walkers. (2015). Allegro medical. com. Retrieved from http: //www. allegromedical. com/walkers-c 516/2 -button-folding-walker-with-5 wheelsp 565603. html? utm_campaign=Comparison%20 Shopping&utm_source=froogle &utm_medium=feed&CS_003=9164468&CS_010=b 4 b 946 b 06 f 18013013 d 52 c 41 38899 c 05&gclid =CJDY 55 Dy 6 Mg. CFc 5 efgod 1 ic. EDQ&kwid=productadsplaid^101314403053 -sku^762%20565603%2001@ADL 4 ALLEGRO-ad. Type^PLAdevice^c-adid^65352197773#762+565603+01

Risk vs. Benefit of Protocol Risk for the institution: Increased initial cost More liability Risk for the nurse: More responsibility Extra documentation Fatigue

Risk vs. Benefit of Protocol Risk for the patient: • Increased pain after exercise • Increased need for pain medication • Increased risk of fall and injuries • Transient oxygen desaturation • Line dislodgement • Hypotension • Cardiac arrest • Loss of consciousness
 Benefit to the institution: Patient shorter length")
Risk vs. Benefit of Protocol (cont. ) Benefit to the institution: Patient shorter length of stay Decreased number of hospitalacquired infection Decreased mortality Reduced overall hospital cost Increase the hospital reputation Benefit to the nurse: Increased education Better patient-nurse relationship
 Benefit to the patient: Decreased lengths of")
Risk vs. Benefit of Protocol (cont. ) Benefit to the patient: Decreased lengths of ICU and hospital stay Decreased the use of mechanical ventilation Lower the patient’s cost Less sedation and delirium, and decreased depression and anxiety

Outcomes All nurses and PCTs will attend one of the four mandatory training sessions before the implementation of “Operation Mobilization” The “Ambu Guru” will report that 100% of the protocol was accomplished each day for each patient. Each patient room will have a posted protocol before implementation. Patients will not experience any falls during the four month trial of “Operation Mobilization” Each patient and/or patient family will verbalize an understanding of the importance of early mobility upon admission to the ICU. The average length of hospital stay in the ICU will decrease by two days over a period of four months.

Conclusion Early mobilization is associated with a decreased ICU length of stay An early mobilization protocol such as Operation Mobilization would be safe and feasible to implement in the ICU setting Because nurses have the most direct contact with their patients, it is important for an early mobilization protocol to be led by nurses and enforced by nurses. The early mobilization protocol requires interdisciplinary coordination and cooperation, and thus education of staff is necessary for its effective implementation

REFERENCES Clark, D. E. , Lowman, J. D. , Griffin, R. L. , Matthews, H. M. , & Reiff, D. A. (2013). Effectiveness of an Early Mobilization Protocol in a Trauma and Burns Intensive Care Unit: A Retrospective Cohort Study. Physical Therapy, 93(2), 186 -196. doi: 10. 2522/ptj. 20110417 Dasta, J. F. , Pilon, D. , Mody, S. H. , Lopatto, J. , Laliberte, F. , Germain, G. , Bookhart, B. K. , Lefebvre, P. , & Nutescu, E. A. (2014). Daily hospitalization costs in patients with deep vein thrombosis or pulmonary embolism treated with anticoagulant therapy. E-Journal of Thrombosis Research Journal. 135, 303 -310. Retrieved from http: //dx. doi. org/10. 1016/j. thromres. 2014. 11. 024 Drolet, A. , De. Juilio, P. , Harkless, S. , Henricks, S. , Kamin, E. , Leddy, E. A. , Williams, S. (2013). Move to improve: The feasibility of using an early mobility protocol to increase ambulation in the intensive and intermediate care settings. Physical Therapy, 93(2), 197 -207. doi: 10. 2522/ptj. 20110400 Engel, H. J. , Tatebe, S. Alonzo, P. B. , Mustilleand, R. L. , & Rivera, M. J. (2013). Physical therapist-established intensive care unit early mobilization program: quality improvement project for critical care at the University of California San Francisco Medical Center. Journal of the American Physical Therapy Association, 93(7), 975 -985. doi: 10. 2522/ptj. 20110420 Evans, B. (2009). Patient mobility in the ICU. Retrieved from www. hanys. org-qualityclincal_operational_initiatives/vapp/docs/patient_mobility_in_the_ICU. pdf Hogan, C. (2015). Early mobilization in the hospitalized patient. Medical staff newsletter: St. Joseph’s healthcare. Retrieved from: http: //www. stjosephhospital. com/Default. aspx? DN=e 6 d 0 de 38 -0 fc 4 -4 b 3 d-b 94 b-bde 1 eef 3480 f Klein, K. , Mulkey, M. , Bena, J. F. , Albert, N. M. (2015). Clinical and psychological effects of early mobilization in patients treated in a neurologic ICU: A comparative study. Critical Care Medicine 43(4), p 865– 873 doi: 10. 1097/CCM. 0000000787 Lord, R. K. , Mayhew, C. R. , Koruplou, R. , Mantheiy, E. C. , Friedman, M. A. , Palmer, J. B. , & Needham, D. M. (2015). ICU early physical rehabilitation programs: Financial modeling of cost savings. Critical Care Medicine, 41(3), 717 -724. doi: 10. 1097/CCM. 0 b 013 e 3182711 de 2 Mah, J. M. , Staff, I. , Fichandler, D. , & Butler, K. L. (2013). Resource-efficient mobilization programs in the intensive care unit: who stands to win? The American Journal of Surgery, 206, 488 -493. Retrieved from http: //dx. doi. org/10. 1016/j. amjrug. 2013. 001

REFERENCES Meddings, J. , Reichert, H. , Rogers, M. A. M. , Hofer, T. P. , Mc. Mahon, L. F. , Grazier, K. L. (2015). Under pressure: Financial effect of the hospital-acquired conditions initiative-a statewide analysis of pressure ulcer development and payment. The American Geriatrics Society Journal, 63, 1407 -1412. doi: 10. 1111/jps. 13475 Pandullo, S. , Spilman, S. , Smith, J. , Kingery, L. , Pille, S. , Rondinelli, R. , & Sahr, S. (2015). Time for critically ill patients to regain mobility after early mobilization in the intensive care unit and transition to a general inpatient floor. Journal of Critical Care. http: //dx. doi. org/10. 1016/j. jcrc. 2015. 08. 007 Titsworth, W. L. , Correia, T. , Reed, R. , Guin, P. , Archibald, L. , Layon, A. J. , & J. Mocco (2012). The effect of increased mobility on morbidity in the neurointensive care unit. Journal of Neurosurgery, 116(6), 1379 -1388. doi: 0. 3171/2012. 2. JNS 111881 Wang, Y. T. , Haines, T. P. , Ritchie, P. , Walker, C. , Ansell, T. A. , Ryan, D. T. , Lim, P. , Vij, S. , Acs, R. , Fealy, N. , & Skinner, E. H. (2014). Early mobilization on continuous renal replacement therapy is safe and may improve filter life. Critical Care, 18(4), R 161 -R 170. doi: 10. 1186/cc 14001 Witcher, R. , Stoerger, L. , Dzierba, A. L. , Silverstein, A. , Rosengart, A. , Brodie, D. , & Berger, K. (2015). Effect of early mobilization on sedation practices in the neurosciences intensive care unit: A preimplementation and postimplementation evaluation. Journal of Critical Care, (30), 344 -347. Retrieved from http: //zp 9 vv 3 zm 2 k. search. serialssolutions. com/? V=1. 0&sid=Pub. Med: Link. Out&pmid=25573283 Zomorodi, M. , Topley, D. , & Mc. Anaw, M. (2012). Developing a mobility protocol for early mobilization of patients in a surgical/trauma ICU. Critical Care Research and Practice. 2012 1 -10 Doi: 10. 1155/2012/964547

QUESTIONS?
- Slides: 49