Omega3 Nutrition Fish versus Supplements CSIRO FOOD AND


 Year of data collection Country Population Greenland Eskimos")
 in 2006 for omega-3 LCPUFA")















: • Symptoms of depression significantly reduced with")








- Slides: 30
Omega-3 Nutrition- Fish versus Supplements CSIRO FOOD AND NUTRITION Manny Noakes Research Director
n-3 LC PUFA intake • LC PUFA n-3 reputed wide-ranging health benefits. • Humans limited capacity to synthesize n-3 LC. • Consumption of preformed n-3 LC PUFA s needed. • Seafood best dietary source. ~20% Australians consumed fish & seafood (Aus Health Survey 2011/12) Vegan, vegetarian and non fish consumers may be very low in n-3 LC PUFA 2 | Slide from W Stonehouse
Median n-3 LC PUFA intakes (mg/day) Year of data collection Country Population Greenland Eskimos 1976 13, 000 Canada Inuit of Nunavik 1992 2115 James Bay Cree 1992 800 ∼ 2008 207 Kyushu<comma> SW island of Japan 1999 905 INTERLIPID study Aito Town 2003 810 INTERLIPID study Japanese living in Hawaii 2003 310 France All regions of France 1995 364 Nth Sth Europe 7 Centres in Europe 2003 239 Belgium Women living in Flanders 2009 199 Australia 1995 National Nutrition Survey German Nutrition Survey USA USDA Netherlands Rotterdam coronary calcification study Quebec Japan 3 | Meyer et al 2011 Median intakes (mg/day) 1995 1998 1994– 1996 1993 170 160 ∼ 115 97
Current Australian Guidelines • NHMRC nutrient reference values (NRVs) in 2006 for omega-3 LCPUFA recommending both an adequate intake 160 mg/day (men) and 90 mg/day (women) and a suggested dietary target to prevent chronic disease – 600 mg/day for men and 400 mg/day for women. • FSANZ also supports the consumption of omega-3 LCPUFA by allowing general-level health claims for heart health on commercially available food products. The food must contain a minimum of 50 mg EPA+DHA combined in a serving of food. • Australian Dietary Guidelines recommend at least 2 serves of (any) fish per week. 4 | Slide from W Stonehouse
Health Claims for Heart Health FSANZ EPA & DHA contribute to heart health EFSA • DHA & EPA contribute to normal function of the heart (0. 25 g/d) • DHA & EPA contribute to maintenance of normal blood pressure (3 g/d) • DHA & EPA contribute to maintenance of normal blood triglyceride levels (2 g/d) • DHA contributes to maintenance of normal blood triglyceride levels (2 g/d in combination with EPA) FDA Supportive but not conclusive research shows consumption of EPA & DHA omega-3 fatty acids may reduce risk of coronary heart disease. 5 | Slide from W Stonehouse
2008 6 | Recommendations
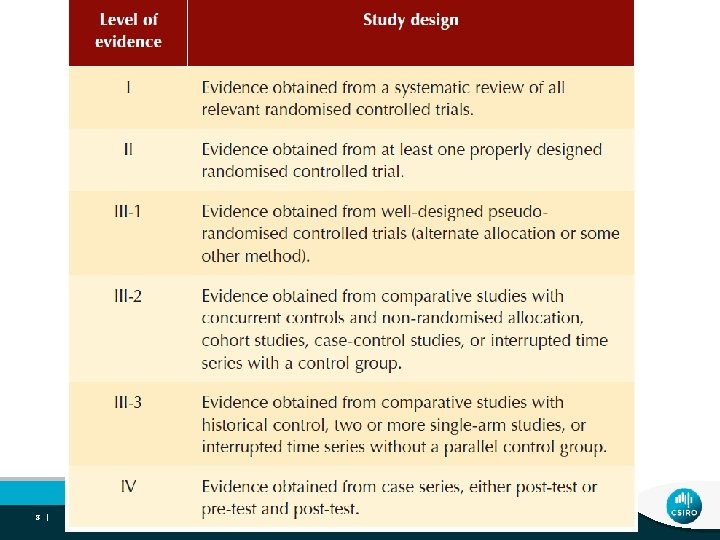
Systematic reviews – literature between 2007 -2013 FISH OIL SUPPLEMENTS • Are omega-3 LCPUFA supplements effective in the primary prevention of coronary heart disease? • Are omega-3 LCPUFA supplements an effective intervention for the secondary prevention of CHD? • Are omega-3 LCPUFA supplements effective in the prevention or treatment of heart failure? • Are omega-3 LCPUFA supplements an effective intervention for lowering plasma triglycerides in hypertriglyceridaemic patients? FISH • Is the reported consumption of omega-3 LCPUFA from fish associated with lower incidence of CHD events in primary prevention? • Is the reported consumption of fish associated with a lower incidence of CHD in patients with existing CHD (i. e. secondary prevention)? • Is the reported consumption of fish, or dietary patterns high in omega-3 LCPUFA associated with lower incidence of heart failure?
Fish Oil Studies 10 |
Are omega-3 LCPUFA supplements effective in the primary prevention of coronary heart There no current evidence that omega-3 LCPUFA disease? Kotwal etis al 2012 Level 1 • Omega 3 Fatty acids and cardiovascular outcomes: supplementation is beneficial or the primary systematic review and meta-analysis Rizos et al 2012 Level 1 CHD prevention of • Association between omega-3 fatty acid supplementation and risk of major cardiovascular disease events: a systematic review and meta-analysis Bosch et al 2012 Level 11 • n-3 fatty acids and cardiovascular outcomes in patients with dysglycemia Itakura et al 2011 Level 11 • Relationships between plasma fatty acid composition and coronary artery disease Roncaglioni et al. 2013 Level 11 • n-3 fatty acids in patients with multiple cardiovascular risk factors doses of EPA/DHA was 1 -2 g 11 |
Kotwal et al 2012 a systematic review and meta-analysis Level 1 Evidence 20 trials and >60 000 patients No effect of ω-3 fatty acids on composite cardiovascular outcomes Copyright © American Heart Association, Inc. All rights reserved.
Are omega-3 LCPUFA supplements effective in the secondary prevention of coronary heart disease? 5 Level 1 ismeta-analyses were included: Kotwal et al. ; Rizos LCPUFA There no current evidence that omega-3 et al. ; Kwak et al. ; Zhao et al. , and Marik et al. supplementation is beneficial for the secondary The two meta-analyses published prior to 2010 provided prevention of CHD evidence of benefit in patients with existing CHD, but the meta-analyses published after 2010 did not. 3. Level II RCTs included the OMEGA study (2010), Alpha to Omega study (2010) and GISSI Heart Failure (GISSI-HF) trial 2 trials provided 1 g EPA/DHA, one for 1 year (OMEGA and GISSI-HF), while the Alpha-Omega trial provided 400 mg EPA/DHA. The OMEGA trials did not find evidence of a beneficial effect 13 |
Might statins inhibit LC PUFA n-3? – possible mechanisms • de Lorgeril et al BMC Medicine 2013 • Statins increase arachidonic acid, the main n -6 fatty acid in cell membranes. • This may in turn inhibit the protective effects of n-3 because n-6 and n-3 fatty acids are in competition through various pathways involved in the development and complications of CHD. • Thus statins may inhibit n-3 by interfering in the n-3/n-6 interplay and favoring n-6. 14 |
Does Statin Use Mitigate the Benefit of Omega-3 Fatty Acids? • Seth et al. 2014 Meta-Regression of Randomized Trials • 23 studies with 38, 910 n-3 LCPUFA; 38, 866 controls. • Lower control group statin use (b = 0. 222, P = 0. 027) and higher DHA/EPA (b = -0. 105, P = 0. 033) ratio was associated with higher reduction in total mortality. Statin use may mitigate, and higher DHA/EPA ratio is associated with the beneficial effect of PUFA supplementation. 15 |
Are omega-3 LCPUFA supplements effective in the prevention or treatment of heart failure? GISSI-HF 7, 000 benefit patientsfrom with functional There is trial modest 1 g n-3 Class II to IV heart failure were randomised to 1 g/day LCPUFA in heart and in particular or placebo. Over a 3. 9 -year median follow-up, in those with greater absolute CHD risk. supplementation resulted in an absolute 9% reduction in mortality or admission to hospital (p=0. 04). Benefit was greater in elderly and diabetic patients and those with impaired left ventricular function (sub-groups with greater absolute risk). Around 300, 000 Australians are living with heart failure, and every year around another 30, 000 people are newly diagnosed with it 16 |
Are omega-3 LCPUFA effective for lowering plasma triglycerides in hypertriglyceridaemic patients? 2 These positivedata meta-analyses confirm high doses n-3 • LCPUFA Hartweg et andfor Reiner et al. 2011 asala 2007 means lowering plasma triglyceride levels. Effective Dosage: • Starting with 1200 mg/day DHA+EPA Increase if needed to: • 4000 mg/day • Checking patient’s response every 3 -4 weeks when the dose is changed, until target TG levels reached. 17 |
Do Omega-3 LCPUFA Alter the Risk or Incidence of High Blood Pressure? • 3 meta-analyses Appel et al 1993, Geleijnse et al 2002, Morris et al 1993 have shown that omega-3 LCPUFA reduce BP with the greatest effect in hypertensive patients -3. 4 to -5. 5 mm. Hg systolic BP -2. 0 to -3. 5 mm. Hg diastolic BP • Dokholyan et al. 2004 also suggested that greater than >3 g/day n-3 LCPUFA is required to reduce BP in patients with highnormal diastolic BP or stage 1 hypertension. Mori et al. showed that in overweight, mildlyhypercholesterolaemic patients, 4 g/day of encapsulated DHA, but not EPA, reduced 24 -hour BP by -5. 8/-3. 3 mm. Hg. 18 |
EPA/DHA and blood pressure: a meta-analysis. Miller et al 2014 • Effect of EPA+DHA on blood pressure in RCTs. • 70 RCTs were included. • The strongest effects in untreated hypertensives systolic blood pressure = -4. 51 mm Hg diastolic blood pressure = -3. 05 mm Hg • BP also lowered among normotensives Provision of EPA+DHA systolic blood pressure = -1. 25 reduces mm Hg systolic BP, while provision of ≥ 2 g omega 3 LCPUFA reduces diastolic BP. diastolic blood pressure = -0. 62 mm Hg 19 |
Omega-3 and LCPUFA Rheumatoid Arthritis • Patient-assessed pain, morning stiffness, number of painful and/or tender joints and non-steroidal antiinflammatory drug (NSAID) consumption • Large dosages EPA+DHA (>3 g/d) needed for 3 months to see symptomatic benefits. • 1 yr trial, 5. 5 g EPA+DHA/d – st lower failure rate of 1 -line therapy (Proudman et al. 2015) |
n-3 LCPUFA and Cognition Suggestive evidence DHA enhances learning and cognitive development in children; memory and reaction time • 3 Meta-analyses – n-3 LCPUFA particularly: improved memory, attention & • Individuals with low habitual intake processing speed in adults with of LC n-3 mild cognitive impairment / age • Children with low literacy ability -related cognitive decline • Age-related cognitive decline Stonehouse et al 2013 Stonehouse et al 2014 21 | Slide from W Stonehouse Yurko-Mauro et al 2015 Mazereeuw et al 2012 Cooper et al 2015
n-3 LCPUFA & Depression Meta-analysis (Martins, 2009): • Symptoms of depression significantly reduced with pure ethyl-EPA and high EPA (>50%) supplements. • No effects seen with pure DHA or high DHA (>50%) supplements. • Greatest effects in therapeutic populations (bipolar disorder and major depression) vs. mild-to-moderate depression • Dose-response effect. 22 |
n-3 LCPUFA in depression • Sublette et al 2011 - 15 trials 916 participants • % EPA in the supplements was the fixed-effect predictor, dichotomized into 2 groups: EPA < 60% or EPA ≥ 60% of the total EPA + DHA • Supplements with EPA ≥ 60% showed benefit on standardized mean depression scores (effect size = 0. 532; P <. 001) versus supplements with EPA < 60% (effect size = -0. 026; P =. 756) • Supplements with EPA < 60% were ineffective. Supplements containing EPA ≥ 60% of total EPA + DHA, in a dose range of 200 to 2, 200 mg/d of EPA in excess of DHA, were effective against primary depression. 23 |
Fish/Dietary Studies 24 |
Is consumption of omega-3 LCPUFA from fish associated with lower incidence of CHD events in primary prevention? Prospective cohort studies • de Goede et al , 2010 Marine (n-3) fatty acids, fish consumption, and the 10 -year risk of fatal and nonfatal coronary heart disease in a large population of Dutch adults with low fish intake • Joensen et al 2011 Marine n-3 polyunsaturated fatty acids in adipose tissue and the risk of acute coronary syndrome • Mozaffarian et al 2013 Plasma phospholipid longchain omega-3 fatty acids and total and causespecific mortality in older adults: a cohort study • Musa-Veloso et al. 2011 Impact of low v. moderate intakes of long-chain n-3 fatty acids on risk of coronary heart disease – benefit with >250 mg omega-3 LCPUFA from fish reducing the risk of sudden cardiac death by 35% • Streppel et al 2008 Long-term fish consumption and n-3 fatty acid intake in relation to (sudden) coronary heart disease death: the Zutphen study There is good evidence that increased consumption of fish or dietary patterns with omega-3 LCPUFA are associated with the primary prevention of coronary heart disease (Level 111) 25 |
Is consumption of fish associated with lower incidence of heart failure? Prospective cohort studies observational data are supportive • These Meta-analysis -7 prospective cohort studies - of a modest inverse fish 176, 441 association subjects withbetween 5, 480 cases of consumption heart failure. and High fish intake. Level protective against developing HF. heart failure. III • Cardiovascular Health Study - 4, 738 US adults >65 y. Highest quintile had 32% lower risk compared to those who consumed fish < or = to 1/month (p trend 0. 009). • A 14. 3 -year follow-up -The Atherosclerosis Risk in Communities (ARIC) study - plasma phospholipid omega-3 LCPUFA (especially EPA) at baseline inversely correlated with heart failure in women but not in men (P<0. 001). 26 |
Is consumption of fish associated with lower CHD in patients with existing CHD (i. e. secondary prevention)? Evidence support s the consumption Evidence from prospective cohort studies of fish oilystudies. fish for Only twoincluding applicable new secondary prevention of CHD. Level III Manger et al. 2010, Dietary intake of n-3 long-chain PUFA and coronary events in Norwegian patients with coronary artery disease. Pottala et al 2010 Blood EPA and DHA predict all-cause mortality in patients with stable coronary heart disease: the Heart and Soul study. 27 |
Are Omega-3 LCPUFA from Fish Associated with Lower Stroke Risk? • Mozaffarian et al. (2013) reported total plasma phospholipid omega-3 LCPUFA were inversely These data suggest that fish intake related to ischaemic stroke risk (p=0. 043) with a associated with lower stroke risk. 37% reduction in the highest versus the lowest quintile, but there was no significant effect on haemorrhagic stroke (p=0. 86). • DHA most strongly associated with reduction in ischaemic stroke and DPA with reduction in stroke death. • Larsson et al. , meta-analysis of fish consumption and stroke in 15 prospective studies, - increment of 3 servings of fish/week associated with a 6% lower incidence of total stroke. • Interventions with fish oil supplementation have not demonstrated any reduction in stroke. 28 | is
Key Findings: Omega-3 LCPUFA supplements - neither a beneficial nor adverse effect demonstrated in primary or secondary prevention of CHD. • The evidence continues to be positive for the role of omega-3 LCPUFA in the treatment of hypertriglyceridaemia • The evidence continues to be positive for the role of omega-3 LCPUFA as a benefit to prevent heart failure. • Higher fish intake was associated with lower incident rates of heart failure in addition to lower sudden cardiac death, stroke and myocardial infarction.
2015 Recommendations FISH • Dietary intake of fish consistently found to be of benefit for the protection from heart disease and stroke. Higher fish intake was associated with lower incident rates of heart failure, o lower sudden cardiac death, stroke and myocardial infarction. • Heart Foundation recommends all Australians include 2 -3 three serves fish (including oily fish)/week as part of a heart healthy eating pattern. • This amount of fish provides between 250 -500 mg per day of combined docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA). SUPPLEMENTS • Omega-3 LCPUFA supplements can be considered in patients with heart failure in additional to standard therapy. • Omega-3 LCPUFA supplements are effective in the treatment of hypertriglyceridaemia. 30 |