Older LGBT Peoples beliefs and experiences regarding General

Older LGBT People’s beliefs and experiences regarding General Practice Services Michael Toze Ph. D Student mtoze@lincoln. ac. uk

Population and Setting • LGBT people aged 60+ – A population who have lived through significant social change (1967 change in law; ICD and DSM pathologisation; equality legislation). – A population who may now be experiencing agerelated health needs • GP services – point of entry into medical services – address later-life health issues relating to lifestyle and wellbeing – Manage patient records.
, Guasp (undated), smaller local surveys – fear of discrimination,")
Existing Literature • Rivers (2006), Guasp (undated), smaller local surveys – fear of discrimination, worries about coming out, heteronormativity • Stonewall (2015) – persistence of discriminatory attitudes among healthcare staff. • Elliot (2015) – LGB people of all ages have reduced levels of trust in GP and poorer health • Bishop (2013), Mc. Neil (2012) – similar issues being raised by trans people • Public Health Framework document – worse outcomes for older LGBT people

Research Gaps • Very little specific work on this population, and even less which focuses on general practice. • What research there is usually focuses on certain issues (HIV!) and populations who are easier to access/more visible (typically urban, younger-old, gay men) • Research often undertaken by campaigning organisations – limited attention to analysis/theory • Largely focused on older LGBT health within “deficit model” – risk factors and vulnerabilities, highlighting the extreme (negative) cases. What about resilience, community knowledge, peer support?

Study Design • Aiming for 40 interviews with LGBT+ people aged 60+ from around the UK, sampling purposively for diversity • Currently 36 aged 60 -82 • Recruited via LGBT community groups, “snowball” samples, magazines/email bulletins • Open-ended, exploratory interviews, focusing on GP experiences, but also how people use community support e. g. LGBT groups, online resources. • Ethical considerations – anonymity, confidentiality • Thematic inductive analysis using N-Vivo

Coming out “It's a good idea to tell your doctor if you're gay, lesbian or bisexual. If your doctor knows about your sexuality or sexual preferences, it can be easier to discuss your life, relationships and health concerns. They can also keep an eye out for any health problems that might be relevant to you. “ (NHS Choices website, Gay Health: Access to Healthcare)
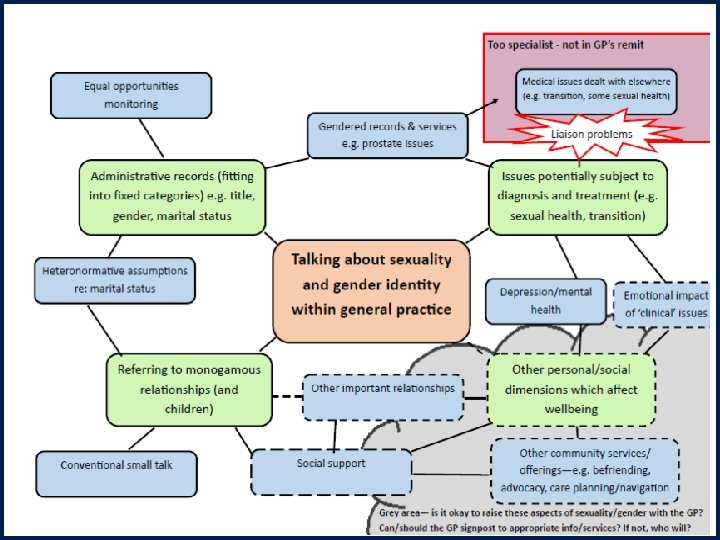

Talking about identity requires context “Uhm, I didn’t actually, it [coming out to the GP] wasn’t um, it was[n’t] just something totally out of the, out of the blue that was just ‘by the way’. I wouldn’t do that. (Julie, lesbian woman, 65) “Obviously I, I would only, I wouldn’t sort of, with a GP practice, kind of go in and announce it, it would more tend to come up, in the conversation of, you know if it, where it was relevant” (Margaret, lesbian woman, 67) “I don’t feel when I meet anyone new or any medical people or whatever I have to say: ‘Excuse me, before you speak I am a lesbian you know’ (Zenobia, lesbian woman, 64)

Monogamous relationships • “We walk in our surgery, you know, if I go on me own, pick up a tablet they say: ‘Where is he? Have you had a row? ’” (Mike, gay man, 62) • “…recently I had to go for an endoscopy so you know it was kind of ‘Have you got someone to go with you? ’ ‘Yes, my partner Claire will accompany me’ and that was the sort of context I might mention it in” (Margaret, lesbian woman, 67) • “I’d like to go to a diabetic [support group] because they do, like, meetings [for] diabetes, you know, when you get round and I don’t know how I would be treated if I came out and I’m not prepared to lie any more and say: ‘uh, uh I live with my ppartner’, you know? I live with a man, don’t I, and I have done for thirty bloody years, for Christ’s sake. Uhm, so rather than participate, you withdraw. ” (Oscar, gay man, 65)

Administrative issues • “Indeed it’s gone on the record, it’s always been on the record, in fact we recently renewed it with when we went to [new GP] the record that uhm e- each can be, oh how do you put it? That confidentiality can be breached between the two of us. In other words, y’know, we be treated like a married couple”(Jeremy, gay man, 69) • “They’ve got a delightful practice manager who’s been y’know, very helpful. Y’know sort of, when I explained she said: ‘Oh that’s no problem. We’ll change your name but we can’t change your gender unless you’ve got a’. But they happily use my doctor title anyway. ” (Vonni, trans woman, 68)

Diagnosis and treatment relating to gender identity or sexuality • “I think it’s, uh, I mean personally I think it’s important [to be out to the GP] so that he knows that if there’s anything, uh, particularly on the sexual health side” (Barry, gay man, 67) • She said ‘What’s the problem? ’ I said ‘Well there’s blah, I’m transgender, I want to, y’know get some treatment for that, HRT etcetera. ’ ‘How long’ve you been like this for? Y’know just general conversation really about it. And she said: ‘I don’t know very much about it myself. I’ve got no experience of it in the practice, ’ she said, ‘myself, uh but obviously I’ll refer you on to the gender clinic in Nottingham. ” (Laura, trans woman, 60)

Clinical issues that are “too specialist” for general practice • “I’ve no real complaint with my GP as a person per se. Other than the whole system is not terribly helpful when it comes to transgender people. If the CCG think it’s nothing to do with them, this whole kind of pass the buck, oh the gender identity clinic deal with that. ” (Vonni, trans woman, 68) • “Living in a town where you don’t have a sexual health clinic the, the GP’s clinics should be trying to be doing more uhm because the rise of um STDs within our town […. ] The publicity that they have with posters and things that they have around the surgery do not mention sexual health matters. ” (Chris, gay man, 66)

Grey area – tackling wellbeing and lifestyle issues. • “I don’t know. Is, is there a lack of interest in lifestyle? I, I don’t. Should there be a greater interest in lifestyle and happiness? I don’t know. Have they got the time, tch, interest or facilities? I don’t know. It, it was just a passing thought. ” (TFR, gay man, 67) • “…yet I don’t feel I could go to my GP here. Even though I’ve revealed to her my sexual identity, I’m not sure I would actually be very happy in asking for a counselling service. What I’ve actually looked at this morning funnily enough is the LGBT counselling service [run by a local charity]. Uhm, so I suppose I haven’t got confidence that normal NHS counselling services, not that I think they couldn’t or shouldn’t, I don’t know. I’m not sure. Perhaps I would, I would probably prefer to go via the LGBT uhm, because I wouldn’t have any qualms obviously right from the start. Y’know we we’ve not even got to go through that bit, have we, of of ‘This is my sexual identity, these are my issues’. ” (Julie, lesbian woman, 65)
 conclusions • “Coming out” in general practice is not a single phenomenon. •")
(Early) conclusions • “Coming out” in general practice is not a single phenomenon. • Wider debates about the GP role, continuity of care, doctor -patient relationships are relevant to how services think about and address the needs of LGBT people over 60. • Wider LGBT networks are important for health and wellbeing, and many interviewees were extremely active in these networks. However, the join-up between networks and general practice was often poor (though some specific examples of good practice).

Any Questions? Michael Toze University of Lincoln mtoze@lincoln. ac. uk
- Slides: 15