OHSU BDMS Heart Co E ACS Program 3

OHSU - BDMS Heart Co. E ACS Program 3 rd Video Conference July 26, 2018

Agenda from OHSU • • • Brief update on upcoming visit Plan of OHSU visit to Thailand Schedule and plan for remaining video conference Standardization through cardiac Co. E at a local level Discussion on radial access, medication, same day discharge

Standardization STEMI Guidelines Reperfusion STEMI Equivalent 15 lead ECG Non STE ACS UA definition NSTEMI, hs-c. Tn Registry ACTION Registry-GWTG Format Definition

Guidelines BDMS Co. E Heart Articles STEMI Practice Guidelines Performance measure 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction (Article) 2015 ACC/AHA/SCAI Focused Update on Primary Percutaneous Coronary Intervention for Patients With ST-Elevation Myocardial Infarction (Article) 2012 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation (Article) 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation (Article) 2014 ���������������� ������ �� 2557 (Article) ����������������� ��� ST Elevation ������ (Article) 2006 ACC/AHA Clinical Performance Measures for Adults With ST-Elevation and Non-ST-Elevation Myocardial Infarction (Article) 2008 ACC/AHA Performance Measures for Adults With ST-Elevation and Non –ST-Elevation Myocardial Infarction (Article) 2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non- ST-Elevation Myocardial Infarction (Article) 2015 ACC/AHA/STS Statement on the Future of Registries and the

Guidelines NSTEMI BDMS Co. E Heart Practice Guidelines Performance measure UA Practice Guidelines Performance measure 2014 AHA/ACC Guideline for the Management of Patients with Non-STElevation Acute Coronary Syndromes (Article) 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation (Article) 2006 ACC/AHA Clinical Performance Measures for Adults With ST-Elevation and Non-ST-Elevation Myocardial Infarction (Article) 2008 ACC/AHA Performance Measures for Adults With ST-Elevation and Non–ST-Elevation Myocardial Infarction (Article) 2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non- ST-Elevation Myocardial Infarction (Article) See NSTEMI guidelines 2017 Classification of unstable angina and non-ST elevation myocardial infarction. Up. To. Date (Article) Unstable Angina: Is It Time for a Requiem? (Braunwald and Morrow) (Article) See NSTEMI Performance measure Statement from ACC/AHA 2008 Performance Measures for Adults With STElevation and Non–ST-Elevation Myocardial Infarction………… Unstable angina (UA) is not considered in this document, in part because of the difficulty in defining the population with certainty.

STEMI

BDMS Co. E Heart Reperfusion Therapy for Patients with STEMI ACCF/AHA 2013 Anticipated D 2 B >120 min Fibrinolysis within 30 min Transfer to PCI center Angiogram/PCI in (2)3 -24 h Next slide

BDMS Co. E Heart Reperfusion Therapy for Patients with STEMI ACCF/AHA 2013 For Thailand Not for Thailand IA (ESC 2012, 2017) IIA (ACC 2013) (For now) (Rescue PCI) (Pharmacoinvasive) STEMI Rx Rapid Reperfusion • Thrombolytic • PPCI • Pharm-invasive The Differences • Culture/knowledge effecting patient decision • Payment system effecting patient decision and time delay • Non PCI capable knowledge and resource • EMS system • Transport system: One/two ways, traffic, helicopter myth for STEMI primary PCI • Solo practice? • ….

The Differences • • Culture/knowledge effecting patient decision Payment system effecting patient decision and time delay Non PCI capable knowledge and resource EMS system Transport system: One/two ways, traffic, helicopter myth for STEMI primary PCI Solo practice ….

BDMS Co. E Heart Society of Cardiology/ACCF/AHA/World Heart Federation Task Force for the Universal Definition of Myocardial Infarction, 2012. “STEMI equivalent” § ST depression in 2 precordial leads (V 1–V 4) may indicate transmural posterior injury (Should perform posterior lead ECG, V 7 -9) § Multilead ST depression with coexistent ST elevation in lead a. VR has been described in patients with left main or proximal left anterior descending artery occlusion § Hyperacute T-wave changes may be observed in the very early phase of STEMI, before the development of ST elevation § [New or presumably new] LBBB have to meet Sgarbossa (-Smith) Criteria) § De Winter STT complex (Not include in current guidelines)

BDMS Co. E Heart

BDMS Co. E Heart

UA

BDMS Co. E Heart A Anginal pain characteristic Ask Location Substernal Others Characteristic Pressure Sharp Others Radiation Exertional relate Duration Relieved by rest 1 st episode Recurrent Crescendo angina CCS angina class Pleuro-pericarditis Others (To be placed in the patient medical record / MD to fill in) Yes No Pain - Pressure, tightness, heaviness, squeezing, fullness, burning, sharp, stabbing, indigestion. • * for ACS (UA) diagnosis needs at least 3 • It should be document on medical record. * Comment / Detail Substernal, shoulder(s), arms (L), neck-throat, Jaw(s), teeth, epigastrium. (see “location”) Second …… /minute …… (>20 Min) → Hours , Days , Weeks , Months * * * * (1, 2, 3, 4) Physician opinion can overide Good for all patient with chest pain. *

BDMS Co. E Heart B Proposal for using uniform UA definition for more uniform statistic Anginal pain in NSTE-ACS (UA and NSTEMI). 1. Prolonged (> 20 min) anginal pain at rest. 2. New onset (de novo) angina (class II or III of the Canadian Cardiovascular Society classification). 3. Recent destabilization of previously stable angina with at least Canadian Cardiovascular Society Class III angina characteristics (crescendo angina) 4. Post-MI angina. (Angina that occurs from a few hours to 30 days after acute MI is defined as postinfarction angina. Cleveland Clinic) NSTEMI 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation Note that 1 -3 criteria of “B” is in “A” too

NSTEMI and hs-c. Tn

BDMS Co. E Heart NSTEMI Diagnosis with 0 hr / 1 hr algorithm (For Roche Elecsys) Rule-out Rule-in 0 hr <5* >52 0 hr <12 0 – 1 hr <3 >5 NSTEMI 2015 ESC Guidelines * Only applicable if chest pain onset >3 h ng/L

BDMS Co. E Heart The first algorithm to rule-in or rule-out AMI within 0 to 1 hour 2015 NSTE-ACS ESC Guidelines Reccommend c. Tn. T-hs values in patients presenting to the emergency department with chest pain 1 0 h < 12 ng/L △ 1 h < 3 ng/L 0 h < 5 ng/L* Rule-out and 0 h ≥ 52 ng/L △ 1 h ≥ 5 ng/L Other Observational zone later, e. g. 3 h) (retest or Rule-in The troponin values have to be used in conjunction with full clinical assessment including clinical symptoms and 12 -lead ECG 1 Roffi, M. et al. (2016). Eur Heart J 37(3), 267 -315 AMI = acute myocardial infarction, ESC = European Society of Cardiology, ECG = electrocardiogram, NSTE-ACS = non-ST-segment elevation acute coronary syndrome * Only applicable if chest pain onset > 3 h

BDMS Co. E Heart Characteristics of the 0 h/3 h and the 0 h/1 h algorithms 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation – Web Addenda Recommend 0 h/1 h algorithm GRACE = Global Registry of Acute Coronary Events; MI = myocardial infarction. a = Effectiveness is quantified by the percentage of consecutive chest pain patients clearly classified as rule-out or rule-in of acute MI (i. e. , approximately 60% for the 0 h/3 h algorithm and approximately 75% for the 0 h/1 h algorithm)

Factors Associated With Appropriate Selection of Invasive Strategy or Ischemia-Guided Strategy in Patients With NSTE-ACS Immediate invasive (within 2 h) 1. Refractory angina 2. Signs or symptoms of HF or new or worsening mitral regurgitation 3. Hemodynamic instability (and cardiogenic shock) 4. Recurrent angina or ischemia at rest or with low-level activities despite intensive medical therapy 5. Sustained VT or VF Early invasive 1. None of the above, but GRACE risk score >140 2. Temporal change in Tn (within 24 h) 3. New or presumably new ST depression Delayed invasive 1. None of the above but diabetes mellitus (within 25 72 h) 2. Renal insufficiency (GFR <60 m. L/min/1. 73 m²) 3. Reduced LV systolic function (EF <0. 40) 4. Early post infarction angina 5. PCI within 6 mo 6. Prior CABG 7. GRACE risk score 109– 140; TIMI score ≥ 2 Ischemia-guided 1. Low-risk score (e. g. , TIMI [0 or 1], GRACE [<109]) strategy 2. Low-risk Tn-negative female patients 3. Patient or clinician preference in the absence of high-risk features ACC/AHA 2014 Guidelines (Slide set) BDMS Co. E Heart YES □ □ □ □ □

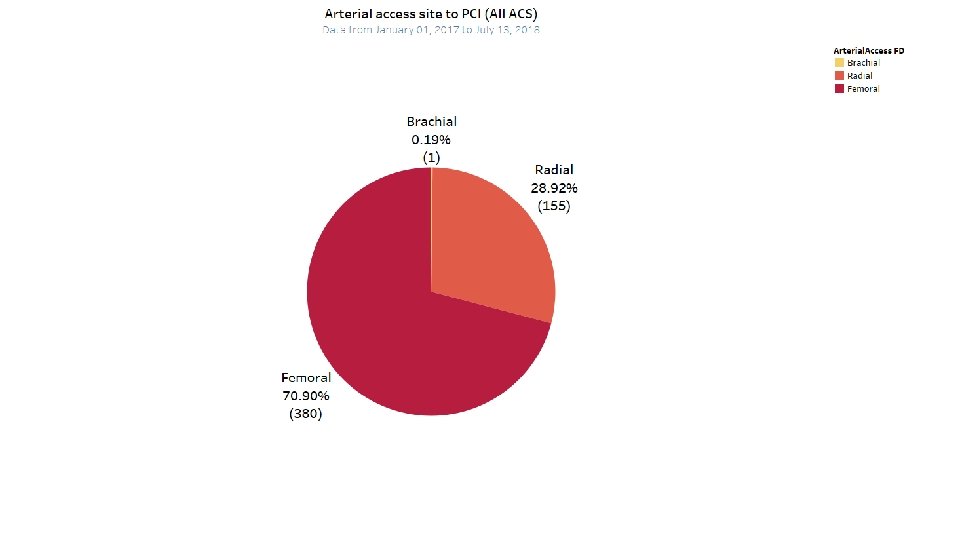
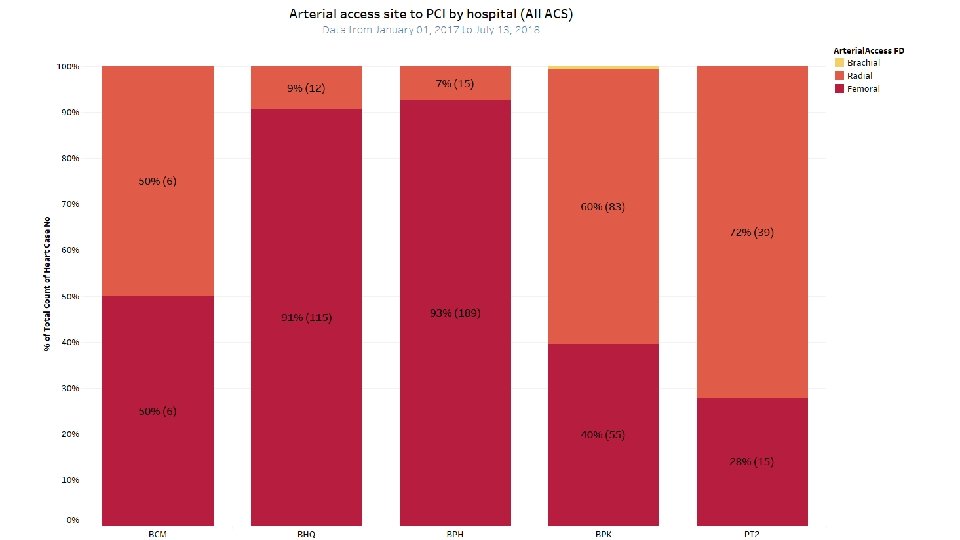
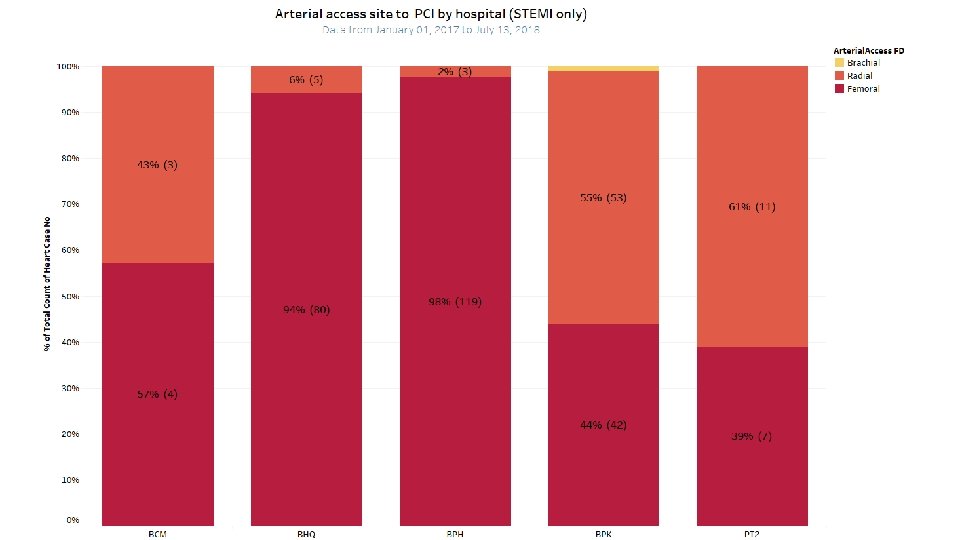
Registry / Radial Access

Thank you

- Slides: 26