Office Based Geriatrics Assessment Mariana B Dangiolo MD

Office- Based Geriatrics Assessment Mariana B Dangiolo, MD Associate Professor of Internal Medicine and Geriatrics

Objectives Understand how to assess a new complex older patient in the office Understand the importance of overall function, including activities of daily living (ADL and IADL) Discuss validated tools for depression and cognitive assessment Discuss medication review

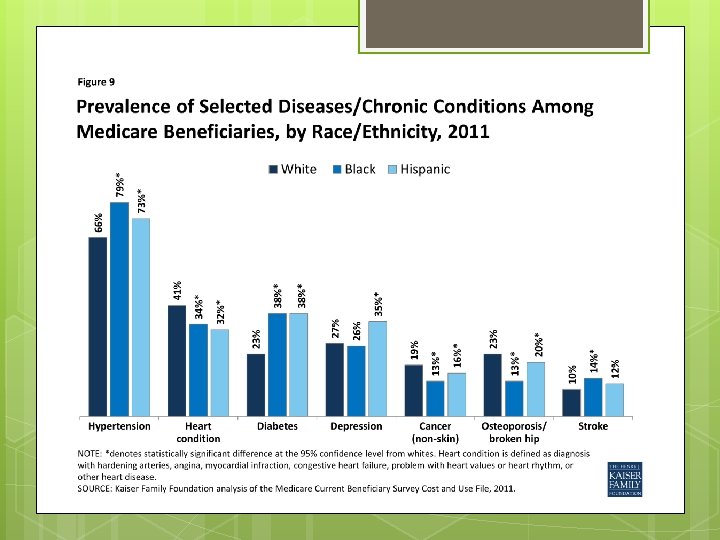
Why is Assessment Important? Americans o o o are aging! 1998: Age 65+ numbered 34 million 2030: Age 65+ will number 72 million Largest increases in those ≥ 85 y old 80% of ≥ 85 have ≥ 2 chronic illnesses Older population more ethnically diverse Most older adults will be cared for by internists and family practitioners

Disease Cascade in Older Persons Young Adults 1 Disease Pathophysiology Symptoms Older Persons Multiple Pathologies Interacting cascade of problems Pure Aging Syndrome Socioeconomics and Environment Habits, Lifestyle, Behaviors Symptoms Functional Loss Disabilities Rx

Your New Patient JB is a 79 yo woman coming to your office to establish care. She recently moved from another state to a 55+ community in Lake Nona to live close to her daughter following the death of her husband.

JB -Past Medical Hx: HTN, CAD w/stent placement 10 years ago, hyperlipidemia, depression, insomnia, UI, osteoarthritis and mild cognitive impairment. -Medications: Aspirin 81 mg, pravastatin 40 mg, donepezil 5 mg, amlodipine 5 mg, solifenacin 5 mg, amitriptyline 10 mg, Tylenol PM. -Past Surgical Hx: cataracts, hysterectomy and cholecystectomy.

JB Lab work done 1 year ago Normal CBC, CHEM 7, TSH Lipid profile with LDL 95, HDL 45 JB is accompanied by a daughter You have 30 min.

Challenges Delivering Geriatrics in Primary Care Short visit times Low reimbursement rates Low numbers of geriatricians Multiple co-morbidities Needs of the patient and caregiver Cross cultural communication

What is Geriatric Assessment? Different models and definitions exist Multidimensional: medical, cognitive, psychological, social, functional, affective, spiritual Best practiced as an interdisciplinary team approach Includes caregiver and environment Emphasis on optimization of function and increase in active life expectancy Evidence that improves detection and documentation of problems. Aging Clinical and Experimental Research (2020) 32: 197 -205

Geriatric Assessment: Components History of current problems Past medical history Specialty physicians involved in care Past surgical history Medication review Social history Family history Current use of community resources Caregiver status and level of support Functional history: ADLs and IADLs ROS to include Geriatric Syndromes

Geriatrics Syndromes Dementia Polypharmacy Delirium Pressure Falls/ Sensory Immobility Incontinence Nutritional Compromise Ulcers Impairments Frailty Dizziness

Why Screening? Underreporting of geriatric syndromes is common Many elderly patients attribute treatable symptoms to “aging” Atypical presentation of disease ( Pneumonia, acute abdomen, MI, depression, etc. ) Geriatrics. 1998 Feb; 53(2): 50 -2, 58 -60

Who Gets Screening? Anyone over age 75 Anyone between 65 and 74 with problems of mind or body ( MSK and cognitive issues) Any - one with Frailty= at least 3 of : weakness low energy slow walking speed low physical activity weight loss

American Geriatrics Society 2016
:")
The Medicare Annual= An Opportunity for Assessment Am Fam Physician. 2018 Jun 15; 97(12): 776 -784.
 Am Fam Physician. 2018 Jun 15; 97(12): 776 -784.")
Medicare Annual (cont. ) Am Fam Physician. 2018 Jun 15; 97(12): 776 -784.
 as functional impairments Functional")
Assessment of Function Medical conditions may present first (or only) as functional impairments Functional loss highly impacts quality of life leading to further disability & institutionalization Functional losses impact patient and caregiver Many older adults spend some time dependent prior to death But…majority of older people live independently Lawton, MP et al (1969) Gerontologist, 9 (3), 179 -186

Functional Impairments ADLs IADLs Bathing Dressing Toileting Transfers Continence Feeding Using telephone Shopping Food preparation Housekeeping Laundry Transportation Medications Managing money Ask: Do you have any problems with ______? Who helps you with it? Lawton, MP. (1988 ). Psychopharmacol. Bull, 24 (4) pp 609 -614 Katz S. (1983) JAGS, 31 (12), 721 -726

AADLs Patient specific activities that can be used to detect subtle functional losses in high functioning patients Can be job or recreation oriented Ex. - Socializing, playing bridge, working, playing golf, playing music, dancing, practicing law, flying a plane, gardening, quilting

Getting Started Watch the patient walk into the room Watching the patient disrobe Climbing up the exam table Picking up a pen Removing hearing aids, tie shoes, etc.

Functional Exam “Put both hands behind your head. ” § “Put both hands behind your back. ” § “Touch your foot with your opposite hand. ” § “Squeeze my fingers. ” § “Pinch this paper. ” § Gait: The “Get up and Go Test” §

Quick Screening for Falls “Have you fallen to the ground in the last 12 months? ” “Get up and go” test: – Have patient sit in chair Rise and walk 10 feet Turn Walk back and sit down Observe for ataxia, hesitancy, stumbling, staggering. If abnormal, further evaluation needed Timed- Get up and Go: – – – - Cut Off >12 secs Predicts: >10 sec = risk of ADL impairment >12 sec= increased FALLS risk > 30 sec= ADL dependence

Tandem and Semi -Tandem

Geriatric Syndromes- Falls Maladaptive Disorders of gait and equipment ADL impairment Past fall Mental –dementia, depression Hearing, vision Medical ( acute and chronic) balance Orthostatic Hypotension Medications Low vit D Environment Ethanol Multiple causes

Sensory • Eyes Ask: “Do you have difficulty watching TV or reading? ” Test with Snellen eye chart while patient wears glasses � Inability to read greater than 20/40 on Snellen chart � Ears Whisper test Ø • Ø Sen 80 -100% Spec 82 -89% Audioscope- set at 40 Db • • • 4 tones 500, 1000, 2000, 4000 Inability to hear 1000 or 2000 Hz Sen 87 -90% Spe 80 -100% The USPSTF recommends routine annual visual and hearing screening for adults after the age of 65 years (a "B" recommendation)

Whispered Voice Test Explain that you will whisper some numbers Ask senior to close eyes 12 -18 inches apart You exhale and then whisper 4 random single numbers at 1 sec intervals Fail Screen if senior cannot hear at least 2 numbers Sen/Sp. 80 -100%/ 82 -89%

Tips for Sensory Impairment Many patients may have difficulty hearing: Lower the tone of your voice Do not shout Use well- lit room Eliminate extraneous noise Face patient May use amplification device Write questions in large print

Incontinence Ask: “In the last year have you ever lost your urine and gotten wet? ” Affects 12% of independent older adults and 50% in NH Medications: alcohol, caffeine, narcotics, tranquilizers, alpha antagonists, beta agonists, Ca channel blockers, antispasmodics, anticholinergics.

Nutritional Assessment “Have you lost 10 lbs over the last 6 months without trying to do so? ” Evaluate if: -Unintentional weight loss 5% or more in 6 months or Low BMI -No evidence that the use of appetite stimulants or high- calorie supplements improve survival or QOL (AGS) Discontinue medications that may contribute to weight loss

Assessment of Cognitive Status v Prevalence of dementia increases exponentially with age. It is 45% -50% at 85 y old. v Sixth leading cause of death in USA v Cognitive impairment increases risk of accidents, delirium, nonadherence, disability, hospitalization v Physicians fail to chart dementia in 80% of mild dementia, 60% -70% in Pts with moderate dementia v Required by CMS in Annual Wellness Exam.

Differential Diagnosis Dementia D- Drugs, Delirium E- Eyes, Ears, ETOH M- Metabolic E- Endocrine N- Nutrition T- Trauma I- Infection A- Affective S- Surgery, Subcortical

Dementia Screen during Annual Wellness Visit “During the past 12 months have you experienced confusion or memory loss that is happening more often or is getting worse? ” cognitive “During past 7 days did you need help from others to perform everyday activities such as eating, dressing, grooming, bathing, walking or using the toilet? ” ADL “During past 7 days did you need help from others to do laundry, housekeeping, banking, shopping using the phone, food preparation , transportation, or taking your own medications? ” IADL

Dementia Screen During Annual Wellness Follow up with structured assessment of cognitive status if any of the following: A- Deficit in ADL cannot be attributed to any physical limitation OR B- Any patient or informant reported concerns C- Positive responses to conventional queries: “Have you noticed any changes in your memory or ability to complete routine tasks such as paying bills or preparing a meal? “
 MMSE: Longer time to")
Office Assessment Cognition Mini-Cog test Verbal fluency test (Animal naming) MMSE: Longer time to administer v Limited by age, education and ethnicity v Most accurate in whites with at least high school v Over 90% sensitive for AD v Only 70% sensitive for other dementias v Copyright fees MOCA: better for early dementias www. mocatest. org v Meulen et al. J Neurol Neurosurg Psychiatry 2004; 75: 700 -705 Holsinger et al. JAMA. 2007; 297 (21)

Animal Naming Useful screening tool for dementia Less than 18/min is abnormal. Scoring equals number named in 1 min Correlates well with MMSE scores ( r= 0. 77) Worsens with time in AD Measures verbal fluency and semantic memory Neurology 1989; 39: 1159 -1165

Mini-Cog 3 item recall: name 3 items, ask to repeat, divert and recall Clock drawing test (CDT) -Recall =0, or -Recall 1 -2 AND CDT abnormal Administration time: 3 min vs 10 min MMSE Sensitivity/Specificity = to MMSE Free of language, education, and cultural bias Borson et al. , JAGS 2003; 51: 1451 -1454 Borson et al Int J Geriatr Psychiatry 2000; 15: 1021 -1027.

Dementia Screen 4: Four IADL Score for Risk of Dementia One Year Later Money Management Medication Management Telephone Use Transportation use PAQUID 2012 Geriatr. Psychol. Neuropsychiatr. Vieil, 2012
 v “Over the past 2 weeks,")
Depression: Patient Health Questionnaire PHQ-2 (sen/spe-. 85/. 65) v “Over the past 2 weeks, have you felt down, depressed, or hopeless? " v "Over the past 2 weeks, have you felt little interest or pleasure in doing things? ” if “yes” to either question proceed with… PHQ-9 : Can confirm diagnosis of chronic depression and be used for follow up on treatment Kroenke, Medical Care 2003 ; 41: 11; 1284 -1292

Review Medications! One Person’s Drugs…

Review Medications Older adults use 3 X more medications than younger patients Drug distribution, elimination, excretion, & pharmacodynamics altered in elderly ADRs and drug interactions increase markedly with # drugs used Medications linked to “reversible dementias”, falls, incontinence, hospitalizations, death Use START, STOPP and Beers list potentially inappropriate prescribing tools. O’ Mahony D. STOPP/START criteria for potentially inappropriate medications/potential prescribing omissions in older people: origin and progress. Expert Rev Clin Pharmacol. 2019, 13 (1): 15 -22

Reviewing Medications Have patient bring in all medications, including OTC’s, herbs, dietary supplements Ask about other providers Consider home health visit if high risk Eliminate questionable medications Simplify regimens and involve caregiver For new medications, start low and go slow

“Avoid Anticholinergics” 1 st generation Antihistamines Muscle relaxants Antipsychotics TCA Antidepressants GI antispasmodics Beers, Arch Intern Med, 2003

Summary Focus on function Consider caregivers Review medications Screen for geriatric syndromes: o falls, incontinence, dementia, depression, hearing, vision, pain Use assessment tools when possible Consider a multidisciplinary team

Thank You!
- Slides: 45