Ocular Surface Disorders Ophthalmology department of the second

 n Intrductions n OSD n Treatment of OSDs n Dry")


: retard water evaporation Water (Lacrimal glands): contains")

 p Injured normal functions and structures of conjunctiva and kerativa")
 Causes Trauma (especially chemical or thermal burns) Auto-immune diseases (e.")




 Rose")

 Measure of tear film stability Mucin deficiency or epithelial")











、subacute、chronic(>3 w) appearance: Papillar")
 Ø “Foreign body” sensation, 异物感 Ø Scratching or")
 ØHyperemia 充血")

 origin position appearance mobility ciliary congestion( 睫状充血) conjunctival posterior arterys anterior")






, when")




 acute mucopurulent or subacute(several hours to days)")







.")















 v Cause is not clear, it is thought to be an irritative")


- Slides: 83
Ocular Surface Disorders Ophthalmology department of the second affiliated hospital, Chongqing medical university Dr. Jian. Jia (简嘉) M. D
(ocular surface diseases, OSD) n Intrductions n OSD n Treatment of OSDs n Dry eye
The Ocular Surface The surface of the area between upper and lower lid margins, including the cornea and conjunctiva Normal function relies on: Normal anatomical ocular structure Normal corneal and conjunctival stem cells �Loss of limbal stem cells leads to failure of corneal epithelialization Normal tearfilm Intrductions
Tear Film 40μm thick, covering cornea and conjunctiva Functions Smoothing out epithelial irregularities for good optic property Moistening cornea and conjunctiva Inhibiting growth of microorganism Providing nutrition Intrductions
Tear Film 3 layers Lipid (Meibomian glands): retard water evaporation Water (Lacrimal glands): contains water-soluble salts and proteins Mucin (Goblet cells): provides hydrophilic surface for aqueous tear Dry eye Deficiency in any components Epithelial abnormalities causing tear film instability Intrductions
正常泪膜构成 Lipid Water Mucin Intrductions
(ocular surface diseases, OSD) p Injured normal functions and structures of conjunctiva and kerativa u Squamou metaplasia u Limbal stem cells deficiency Intrductions
Ocular Surface Disorders (OSD) Causes Trauma (especially chemical or thermal burns) Auto-immune diseases (e. g. , Steven-Johnson Syndrome) Major OSDs Limbal stem cell failure Dry eye Intrductions
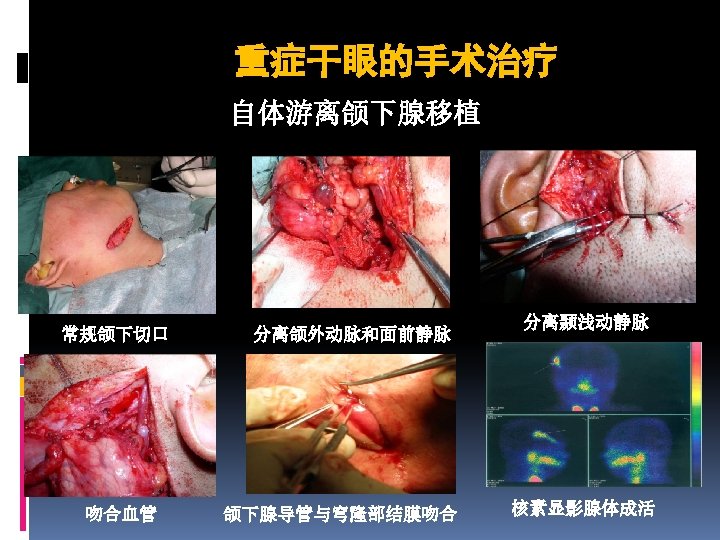
Treatment for Stem Cell Failure Chemical or thermal burns Limbal stem cell transplants from the fellow eye or a donor eye Pre-op Post-op Intrductions
V e r y Dry Eye c o m m o n c o n d i t i o n Intrductions
Causes of dry eye multiple factors interaction p p p immuno-inflammation decrease of sex hormone cell apoptosis environmental factors(dust、smoke、 air-condition et al) ocular surface alterations that secondarily cause tear film instability Intrductions
Classification of dry eye Dry dye Secretion decline Sjögren Syndrome Non-Sjögren syndrome Dry eye research group in U S (1995) rapid evaporation MGD exposure Abnormal blink Contact lens
Clinical Tests for Tear Film Evaluation Schirmer’s test Tear film break-up time (BUT) Rose Bengal staining Fluorescein staining Other tests Tear Lysozyme Assay Tear osmolality Ocular Ferning test Impression cytology Lactoferrin
Schirmer’s Test Measure of aqueous production Insert a filter paper strip into the lower conjunctival sac Without anesthesia – main lacrimal gland secretion With anesthesia – accessory lacrimal glands Measure the moistened exposed portion after 5 min Normal > 10 mm (w/o anesthesia), >5 mm (anesthesia) False positive/negative results
Tear Film Break-up Time (BUT) Measure of tear film stability Mucin deficiency or epithelial abnormalities leads to rapid break-up Examination Fluorescein Blink and hold Observe under colt-blue light Measure the time that elapses before first dry spot appears Normally > 15 seconds Influenced by environment and observer first dry spot appears
Corneal Staining Fluorescein Stains eroded or denuded epithelium Rose Bengal & Lissamine green Stains nonvital epithelial cells More sensitive for conjunctiva
diagnostic of Dry Eye p Clinical finds Scratchy or sandy sensation , itching, excessive mucus secretion, inability to produce tears, a burning sensation, photosensitivity, redness, pain, difficulty to moving the eye lids. p instability of the tear film BUT p defects of the corneal and conjunctiva epithelial Staining p Tear Osmolality
Dry Eye Epithelial erosion Steven-Johnson Syndrome Severe chemical burn Corneal vascularition
Treatment of Dry Eye A chronic condition and complete relief is unlikely unless in mild cases Artificial tears is the mainstay of treatment Fluid replacement Mucin simulation Prolonged surface wetting Corneal toxicity of preservatives Punctal plug Temporary or permanent Androgen Immune supressors Treatment of concurrent infections Chronic blepharitis Rosacea
Punctal plug Smart-Punctal plug
Prevention � � l l of Dry Eye Prevention of VDT syndrome How to use computer rightly stay space to screen sight line superior to screen
Conjunctival disease
1. General introduction
1. 1 Summary palpebral conjunctiva conjuctiva bulbar conjunctiva fornix conjunctiva conjunctivitis : the most common conjunctival disease
1. 2 Etiological factor Microorganisms infection Physical or chemical damage Allergic factors Malnutrition, etc
1. 3 Classification Etiological: infectional、immune、chemical、secondary、 system、no reason speed : hyperacute、acute(<3 W)、subacute、chronic(>3 w) appearance: Papillar hypertrophy 、Follicle、Membranes or pseudomembranes 、 scar、Granulomas
1. 4 Clinical manifestation v. Symptom(症状) Ø “Foreign body” sensation, 异物感 Ø Scratching or burning sensation, 烧灼感 Ø Itching, 痒 If cornea be involved in Ø eye ache , 眼痛 Ø Tearing , 流泪 Ø Photophobia, Ø Blur 畏光 视物模糊
v. Signs (体征) ØHyperemia 充血
Three type: conjunctival congestion mixed congestion ciliary congestion
conjunctival congestion (结膜充血) origin position appearance mobility ciliary congestion( 睫状充血) conjunctival posterior arterys anterior cilliary artery zone of the fornix Corneal limbus Reticulate, more vascular radiate、less vascular branch, bright red branch, dark red Movable with conjunctiva Reponse to Extinct fast AD Non-movable with conjunctiva Extinct mildly
Ø Chemosis 水肿
Øsubconjunctival hemorrhage 结膜下出血
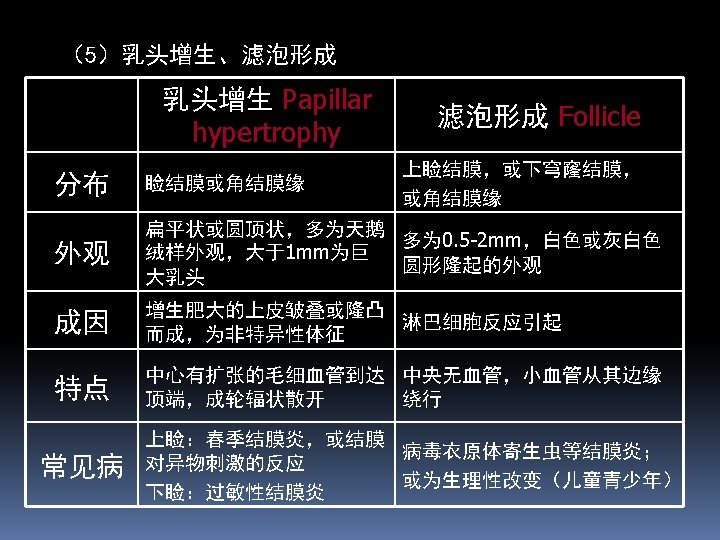
ØPapillar hypertrophy 乳头增生 Nonspecific ØFollicle 滤泡 Focal lymphoid hyperplasia, rounded avascular white or gray structure
ØMembranes 膜or pseudomembranes假膜: pseudomembranes n formed by fibrious exudation and cohere with palpebral conjunctiva, the former binding with conjunctiva strongly and can be stripped difficultly , but the latter loosely and easily. Membranes
Ø Conjunctival scar: n 结膜瘢痕 onset only when conjunctival matrix was damaged. Ø Granulomas 肉芽肿 Ø Preauricular lymphadenopathy 耳前淋巴结肿大 n usually appear in viral conjunctivitis, Ø Pseudoptosis infiltration of Muller’s muscle 假性上睑下垂
1. 5 Checking and diagnosis v Clinical examination v Cytological examination Bacterial conjunctivitis : polymorphonuclear leukocytes, Viral conjunctivitis: mononuclear and lymphocyte, Chlamydial(衣原体性) conjunctivitis: neutrophil and lymphocyte, Allergical and vernal conjunctivitis: Eosinophilia and basophil
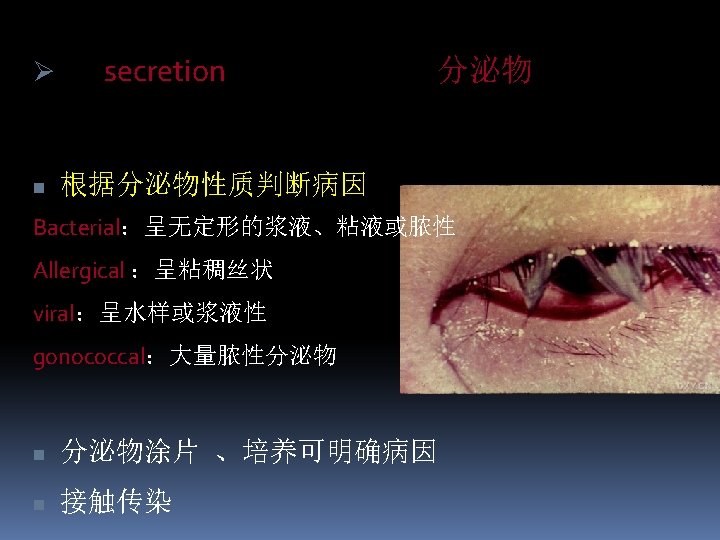
v. Etiological examination • the microscopic examination of conjunctival secretion smear and scrapings(分泌物涂片、结膜刮片), when necessary, fractional cultivation and antibiotic sensitivity tests are desirable
1. 6 Treatment v Depending on microbiologic agent. Topical therapy is capital and assists with systemic therapy v Topical therapy Eye drops: The capital route of administration。It should be used frequently in acute time and decreased frequency when state improving 。 Eye ointment : a persistent therapeutic action, but it can make patient feel fogged vision –medication at bedtime
Conjunctival sac flushing : when conjunctival secretion is copious, flushing is necessary with non-stimulate rinse, such as 3% boric acid solution、 1 -2 times everyday. Wrapping is inhibitted in acute conjunctivitis v systemic drugs It is not necessary in common conjunctivitis, but in gonococcal (淋菌性)and chlamydial(衣原体) conjunctivitis it’s necessary
1. 7 Prognosis and prevention v Most conjunctivitis can be cured and has no sequelae, in some severe or chronic cases, symblepharon (睑球粘连) or dry eye can occur. v Medical members shoud wash hands after checking patients, the washing utensil of patients should be separated and steriled, in addition, healthful administration of public place should be strengthened
2. Bacterial conjunctivitis
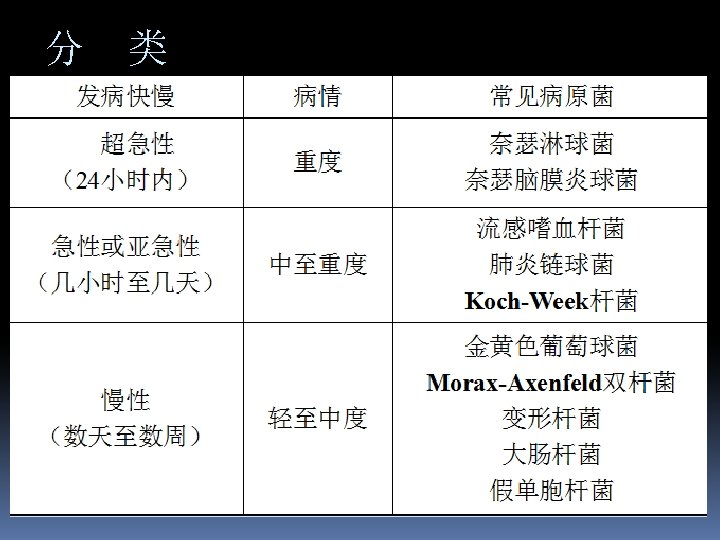
v inflammation and purulent exudation hyperacute---purulent(<24 h) acute mucopurulent or subacute(several hours to days) chronic(several days to weeks)
Hyperacute v Pathogenisis : Neisseria gonorrhoeae淋球菌 or meningococcus 脑膜炎球菌 v Characteristic: strong infectivity, Destructiveness; profuse purulent exudate v incubation peroid rapidly several hours,2 -3 days, develop
v. Clinical symptoms and signs symptoms: pain, photophobia, tearing signs: n eyelids edema , n conjunctival hyperemia n chemosis conjunctiva can protrude out of lid fissure when chemosis strongly
Secretion: from serous or hematodes to purulent, and flow from lid fissure continually。After 10 days or several weeks, purulent exudate decrease gradually。 Severe corneal damage, perforation or loss of eye Preauricular lymphadenopathy 耳前淋巴结肿大 Septicemia 败血症 or meningitis 脑膜炎。
Acute or subacute conjunctivitis v Pathogenic bacteria v streptococcus pneumoniae, Koch-weeks bacillus, hemophilies influenzae, staphylococci, etc。流感嗜血杆菌, Koch-Week杆 菌, 肺炎链球菌 v characteristic often occurs in epidemic form and is called “pinkeye”; acute onset; both eyes invasion or separated by 1 -3 days; symptoms: tearing, foreign body sensation, burning sensation
Signs: l Secretion is copious , so the lids are often firmly stuck together on waking l Hyperemia: especially in fornix and bulbar conjunctiva l Pseudomembrane or membrane
Chronic Hyperemia mildly and little mucous secretion Symptoms: Itching, foreign body sensation, eyestrain (眼疲劳). Signs: hyperemia, little papillary hypertrophy and follicle
Treatment Systemic therapy is as important as topical therapy Topical therapy: n conjunctival sac flushing frequently with saline or 1: 10000 liquor potassic permanganate (高锰酸钾)or 3%boric acid when conjunctival secretion is profuse. n Eyedrops and eye-ointment:proper antibiotic application can shorten course of disease, eyedrops application frequently
Systemic therapy: systemic antibiotic application is emphasized in Neisseria bacteria
Prevention Hygiene 卫生 Patients in acute phase separated 隔离 Cleanse 消毒 Protect healthful eye, etc. 保护健眼
3. Chlamydial conjunctivitis 衣原体性结膜炎
Trachoma A chronic infective keratoconjunctivitis Epidemic before the 1950 s in our country, and it is the first cause of blindness Drop obviously after the 1970 s and only appear in remote area now. l Etiological factor – chamydia (antigenic type A、B、C、or Ba)
4. Viral conjunctivitis
Adenovirus conjunctivitis v Acute follicular conjunctivitis v Strong infective v Appear in 2 types Epidemic keratoconjunctivitis Pharyngoconjunctival fever
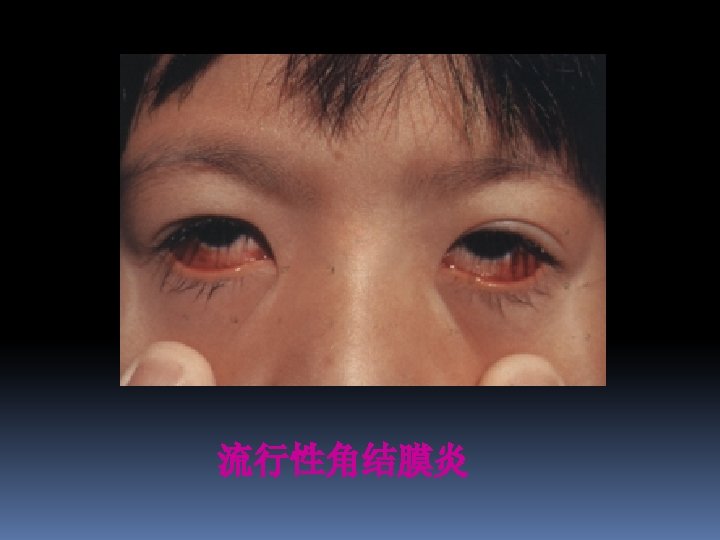
Epidemic keratoconjunctivitis Caused by adenovirus types 8, 19, 29 and 37(subgroup D of the human adenoviruses) Clinical manifestation Incubation peroid: 5 -7 days, usually bilateral, the whole course continue 3 -4 weeks Syptoms: foreign body sensation, pain, photophobia, tearing
Signs: � eyelids edema, obvious hyperemia, chemosis, �much follicles and subconjunctival hemorrhage often appearing within 48 h, �pseudomembrane, �Preauricular lymphadenopathy is characteristic, �Corneal: epithelial keratitis, round subepithelial opacities.
v. Treatment v there is no specific therapy at present, topical administration is main method, such as antiviral eyedrops v. Cold compresses(冷敷) and angiotonica(血管收缩) will relieve some symptoms.
Epidemic hemorrhagic conjunctivitis Caused by enterovirus type 70, self-limited Strong infective, epidemic widely in 1971 in our country Clinical manifestion symptoms: pain, photophobia, tearing, red, foreign body sensation Signs: hyperemia, chemosis, copious follicles, subconjunctival hemorrhage(onset from the upper conjunctiva), preauricular lymphadenopathy Treatment: same to epidemic keratoconjunctivitis
5. Immunologic conjunctivitis
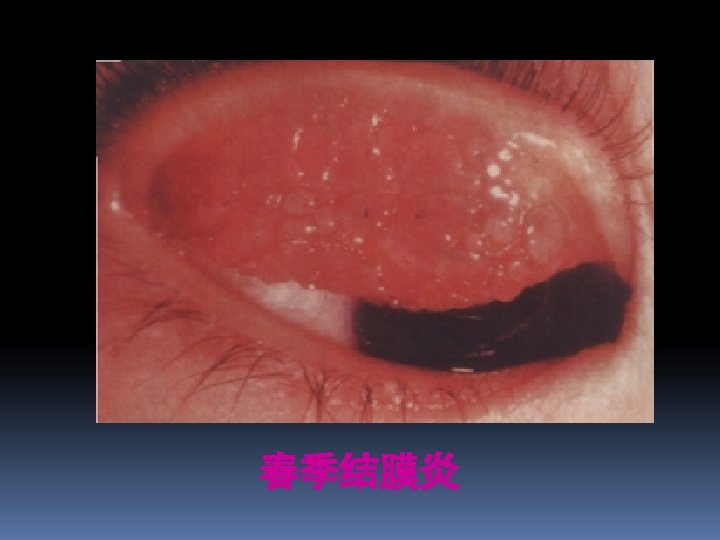
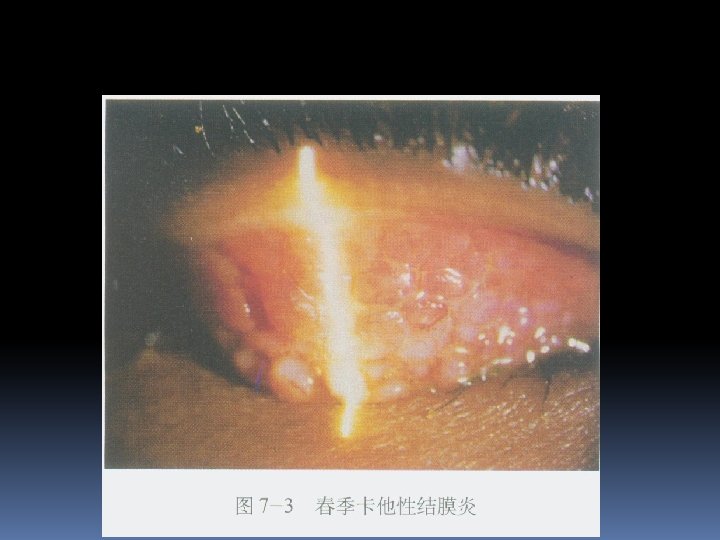
Vernal conjunctivitis v it’s a bilateral allergic disease that usually begins in the prepubertal years (青春期)and lasts for 5 -10 y, more oftener in boys than in girls. seasonal, repeated v Clinical manifestion v symptom: extreme itching v Signs: deviding into 3 types according to diseased region as following:
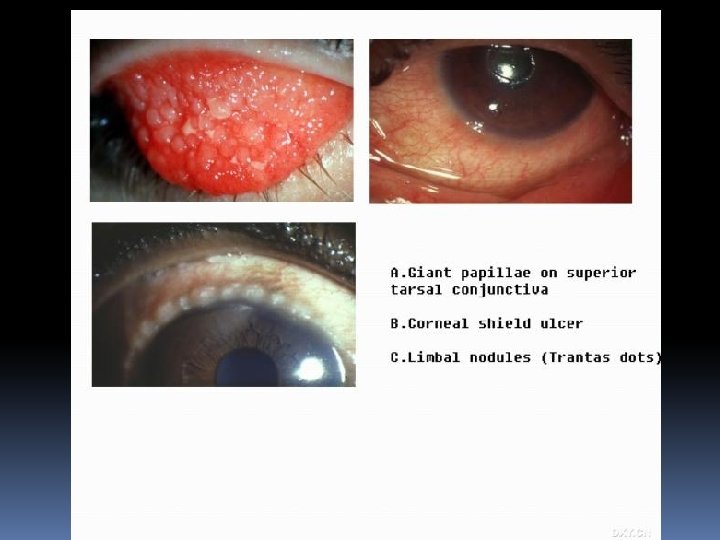
Tarsal conjunctival type Giant papilae on the upper conjunctiva that give a cobblestone appearance Stringy conjunctival discharge Fine, fibrinous pseudomembrane(Maxwell-Lyons sign) Self-limited Corneal limbus type Dark red gelatinous swellings (papillae) at the limbus Mixed type
v. Treatment Self-limited disease General treatment: avoid of propable sensitinogen, cold compresses, ice packs Drug administration v. Cell membrane stabilizer v. Vasoconstrictors v. Steroid eye drops
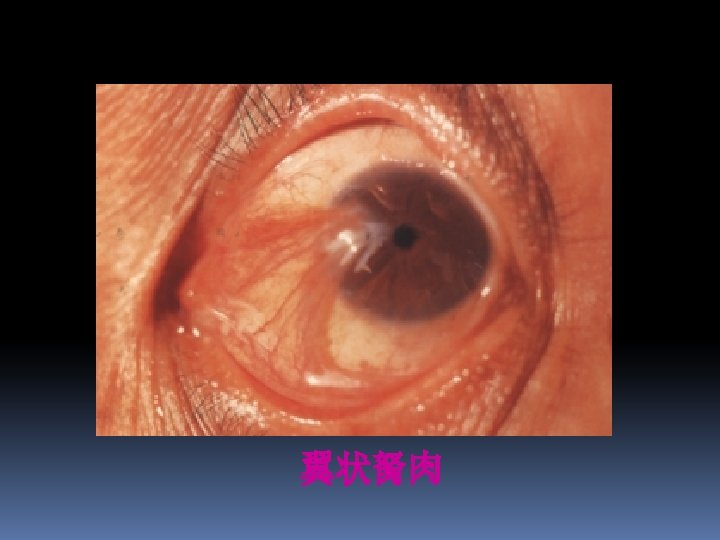
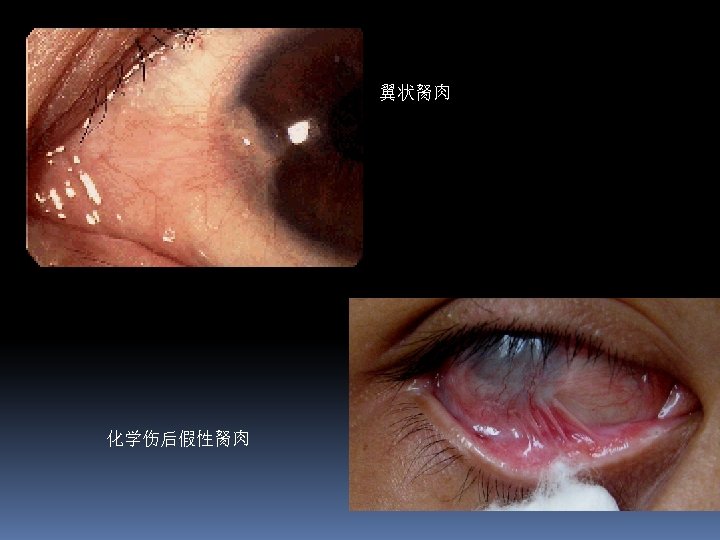
Pterygium( 翼状胬肉) v Cause is not clear, it is thought to be an irritative phenomenon due to ultraviolet light, drying and windy environments. v Signs: fleshy, triangular encroachment of a pinguecula onto the cornea, ususlly on the nasal side bilaterally. v Treatment:removed surgically when encroach to pupil area or cause clear astigmatism(散光)
Importance 1. Symptoms and signs of conjunctivitis 2. Diagnosis and treatment of acute conjunctivitis. 3. different of conjunctival congestion and ciliary congestion.
Thank you