Ocular Rosacea Effect of treating small intestinal bacterial

Ocular Rosacea Effect of treating small intestinal bacterial overgrowth Leonard Weinstock, MD Associate Professor of Clinical Medicine Washington University in St. Louis Specialists in Gastroenterology

Disclosures Speaker’s Bureau: Salix Actavis Entera Health Romark I am a gastroenterologist

Review • Small intestinal bacterial overgrowth • Enteric infections lead to diseases • Rifaximin for facial rosacea-SIBO • Rifaximin for ocular rosacea-SIBO

Rosacea and the Gut • • • Alcohol & obesity – 13 th century (Chaucer) Dyspepsia – 1895 Food intolerance/allergies – 1926 -1966 Achlorhydria – 1935, 1941 Gastritis – 1941 Celiac/jejunal diseases – 1965, 1970 Chronic pancreatitis – 1982 H. pylori – 1990’s IBD – UC 1989; CD 2000 Small intestinal bacterial overgrowth – 2008

Normal host prevents SIBO Stomach Colon bacterial balance, integrity & immunity 0 - 1000 Mucosal absorption Pancreas Colon 100, 000, 000 coliforms (bacteroides, firmicutes, bifidobacter, clostridium) Acid Motility ICV Distal ileum 100, 000 -1, 000, 000 coliforms oral bacteria Immunity (streptococcus, lactobacillus) Duodenum & Jejunum 1, 000 oral bacteria Proximal ileum 10, 000 oral bacteria Mondot. Dig Dis 2013; 31: 278 -85.

SIBO syndrome • Definition – >105 colony forming units/m. L in jejunum – Sx and/or signs of malabsorption • Treatment – 1 o small bowel abnormality – Antibiotics – Motility – Intestinal permeability Gregg CR, Toakes PP. In Sleisenger and Fortran. Gastrointestinal and Liver Disease.

SIBO Syndromes Scleroderma * Small intestinal pseudo-obstruction Achlorhydria * Diabetes * Pancreatic insufficiency * Radiation enteritis Jejunal diverticulosis Immunodeficiency: CLL, Ig. A def. , T-cell def. * Associated w rosacea Billroth, Blind-loop ICV resect. , J-pouch

New SIBO Syndromes • • Crohn’s dis. * Celiac dis. * Irritable bowel synd. * Chronic liver dis. * • • • Restless legs synd. Rosacea Parkinson’s dis. * • • Renal failure Hypothyroidism Acromegaly Post-chemotherapy Fibromyalgia Rheumatoid arthritis * Interstitial cystitis Chronic prostatitis * Associated with rosacea Weinstock. Dig Dis Sci 2010; 55: 1667 -73. ; Weinstock. Inflam Bowel Dis 2010; 16: 275 -9. ; Pimentel. N Engl J Med 2011; 364: 22 -32. Walters, Weinstock. Sleep Med 2011; 12: 610 -3. ; Bellot. Liver Int 2013; 33: 31 -9. ; Parodi. Clin Gastroenterol Hepatol 2008; 6: 759 -764. ; Fasano. Mov Disord 2013; 28: 1241 -9. ; Weinstock. Dig Dis Sci 2008; 53: 1246 -51. ; Geng. Can J Urology 2011; 18: 5826 -30.
 w Gram-pos & neg;")
Rifaximin is Ideal Antibiotic for SIBO w Non-systemic (<0. 4%) w Gram-pos & neg; aerobes & anaerobes w Bile > water soluble – kills more bacteria in small intestine than colon w Kills C. difficile Huang DB, Du. Pont HJ. J Infection 2005; 50: 97 -106.

Post-infectious IBS & Associated Syndromes Infection in gut Motility leads to SIBO Genetic phenotype (low IL-10) for IBS Pi-IBS, Rosacea, FMS, RLS, CPPS

42 F s/p dysentery followed by: – E/F/Phyma & ocular rosacea – IBS-c – Cognitive dysfx – Fatigue – RLS 45 40 35 30 25 H 2 20 CH 4 15 Dx of SIBO by LBT 10 5 0 0 30 45 60 75 90

Rifaximin 1650 -mg/d/14 d: Day 0 and Day 45 Eyes, RLS, fatigue, & memory Improved

Inflammation in SIBO • Interleukins – IL 1ß, 6, 8**, 12 • TNF-α • LPS • T- and B-lymphocytes • Mast cells** infiltration in gut • Increased histamine, tryptase and serotonin • Substance P • ** In rosacea Riordin. Scand J Gastroenterol 1996; 31: 977 -84. Lin. JAMA 2004; 292: 852 -8. Hughes et al. Am J Gastroenterol 2013; 108: 1066 -74. Martinez et al. Gut 2013; 62: 1160 -8.
 • Genoa, Italy: 46% of 113 consecutive rosacea clinic")
SIBO in Rosacea: Prevalence (LBT+) • Genoa, Italy: 46% of 113 consecutive rosacea clinic pts • St. Louis, MO: 51% of 63 consecutive GI clinic pts with rosacea • St. Louis, MO: 66% of 176 consecutive GI clinic pts with rosacea Parodi et al. Am J Gastroenterol 2008; 6: 759 -764. Weinstock, Steinhoff. J Am Acad Dermatol 2013; 68: 875 -6. Weinstock. EMR review of records 2008 -2013.

Rifaximin for Rosacea: Italy • 52 LBT+ randomized for Rx • Rif 1200 -mg/d/10 d vs. Placebo • Rifaximin (N=32) • 71% GA score 0 • 21% GA score 1 • Placebo (N=20) • • 10% worse 90% unchanged Parodi et al. Am J Gastroenterol 2008; 6: 759 -764.

Rifaximin 1200 -mg/d/10 d: Day 0 & 1 mo later Courtesy of V. Savarino: Paroldi et al. Clin Gastroenterol Hepatol 2008; 6; 759 -6.

Rifaximin 1200 -mg/d/10 d: Day 0 & 1 mo later Courtesy of V. Savarino: Paroldi et al. Clin Gastroenterol Hepatol 2008; 6; 759 -64.

Rifaximin for Rosacea: St. Louis • N=63 pts • E/T in 50, PP in 9, Ocular in 4 (3 had E) • LBT+ 32/63 (51%) vs. 3/30 (10%) controls (RR, 5. 0; 95% CI, 1. 7 -15. 1; P<0. 001) • 28 of 32 LBT+ pts were treated • Rifaximin 1200 -mg/d/10 d open label Weinstock, Steinhoff. J Am Acad Dermatol 2013; 68: 875 -6

Improvement: self-assessed % Responders 50 45 40 46% 35 30 25 25% 20 15 18% 10 11% 5 0 Cleared/marked Cleared or Marked Moderate Mild Unchanged Weinstock, Steinhoff. J Am Acad Dermatol 2013; 68: 875 -6.

Rifaximin 1200 -mg/d/10 d: Day 0 & 1 mo later Significant change in nose & pruritic rash over right eyebrow – patient seen 1 year later & both areas were clear

Rifaximin 1200 -mg/d/10 d: Day 0 & 1 mo later

Improvement: self-assessed All 4 of those with ocular disease improved Weinstock, Steinhoff. J Am Acad Dermatol 2013; 68: 875 -6.

Ocular Rosacea SIBO Study Methods • Refractory ocular rosacea pts referred by four ophthalmologists • Open-label, rifaximin 1650 -mg/d for 10 -14 d in LBT+ • Global assessment 10 d & 20 d after ending rifaximin: marked, moderate, mild improvement, or unchanged Weinstock 2016
, age 59 • Facial rosacea")
Ocular Rosacea SIBO Study • N=24 (21 F/3 M), age 59 • Facial rosacea in 4 • LBT+ in 9/24 (38%) • GI sx in 63% LBT+ vs. 33% LBTWeinstock 2016

Ocular Rosacea SIBO Study Global assessment in 7 pts 4 marked improvement 1 moderate improvement 2 mild improvement » Two did not take Rx • Insurance denied the prescription in one subject • One subject was lost was to follow up Weinstock 2016

Rifaximin 1200 -mg/day/10 d: Day 0 & Day 30

Rifaximin 1650 -mg/day/14 d: Day 0 & Day 14 Less edema, redness and foreign body symptoms after Rx

Rifaximin 1650 -mg/day/14 d: Day 0 & Day 14 Less injection of conjunctiva, decreased lid margin inflm, no symptoms

Rifaximin 1650 -mg/d/14 d: Day 0 & Day 30

Rifaximin for Ocular Rosacea Conclusions • Rifaximin led to improvement in this small open-label study • Dysregulation of innate immune system d/t GI inflammation could increase systemic cytokines and microbial antigens/antibodies affecting eyelids and meimobian glands


Standard of Care Rx • Increase ambient humidity • Omega-3 fatty acid • Eyelid hygiene: eyelid warming then massage and expression of MG secretions • Topical emollient lubricant or liposomal spray • Topical azithromycin • Bedtime lubricant • Oral tetracycline or doxycycline • Anti-inflammatory therapy (cyclosporine)
")
Ocular Rosacea Prevalence: up to 58% of rosacea pts (more in older age group) Symptoms: dry eyes, foreign body sensation, burning, decreased tears, watering, pain, photosensitivity Signs: eyelid erythema and vascularization, lymphedema, blepharitis, and corneal ulcers

Rosacea Multiple disorders & triggers Interacting disorders Altered local immunity Vascular and neural disorders Cutaneous disorders Inflammation SIBO TLR 2 & calthelicin Mites & bacteria Inflammation & immunity SIBO Triggers Environmental Food

Rifaximin for rosacea: 1 st study • N=113 pts seen in Rosacea Clinic • 83 F, 31 M, age 52 • 52/113 (46%) LBT+ • 24/113 H. p. + (7 had SIBO) • 7 pts treated for H. p. 1 mo after SIBO Rx (clinical response occurred with SIBO Rx) • GI sx response analyzed Parodi et al. Am J Gastroenterol 2008; 6: 759 -764.
 (97% fecal excretion) w Gram-pos & neg;")
Rifaximin properties: benefits w Non-systemic (<0. 4%) (97% fecal excretion) w Gram-pos & neg; aerobes & anaerobes w Bile > water soluble – kills more bacteria in the small intestine than colon w Kills C. difficile Huang DB, Du. Pont HJ. J Infection 2005; 50: 97 -106.
 • Rifaximin 1200")
Rifaximin for rosacea • N = 52 LBT+ (H 2 excretion) • Rifaximin 1200 mg/d/10 d vs. Placebo • Randomized, blinded only to pts • IGA scoring • 2 dermatologists (Kappa = 0. 97) • Additional studies • Cross-over for placebo group • Open label used for SIBO-negative pts • Subtype rosacea evaluated Parodi et al. Am J Gastroenterol 2008; 6: 759 -764.

Additional study results • X-over: placebo group treated open-label • 17/20 LBT normalized • 15 of the 17 had rosacea cleared • 45/52 total eradication with rifaximin • 35/45 cleared • Improvement maintained in 96% at 9 mo • 2 w pap/pust returned & Re-Rx worked • LBT- group treated (see next) Parodi et al. Am J Gastroenterol 2008; 6: 759 -764.
 Rifaximin 1200 mg/d/10 d (N=20) Parodi et al. Am J Gastroenterol 2008; 6:")
(N=32) Rifaximin 1200 mg/d/10 d (N=20) Parodi et al. Am J Gastroenterol 2008; 6: 759 -764.
 SIBO positive Eradicated (LBT better) Rosacea cleared Flush")
Rifaximin for subtypes Patient type (N) SIBO positive Eradicated (LBT better) Rosacea cleared Flush (2) 2 2 2 Fl/Erythosis (27) 0 - - Papules (8) 6 5 4 Fl/Pap (34) 11 9 9 Fl/Ery/Pap (8) 7 6 3 Pap/Pustules (7) 4 4 4 Fl/Pap/Pust (16) 13 11 8 All four types (11) 9 8 5 Pap/Pust groups had SIBO > non P/P (p<0. 001) Parodi et al. Am J Gastroenterol 2008; 6: 759 -764.

Activating factors • Intestinal permeability Mast Cells – in gut • Seen with SIBO • Bacteria and byproducts • Food allergies (Ig. E- & non-Ig. E-mediated) • Neuropeptides • Bile acids Mediators • Histamine • Tryptase • Lipid mediators • Cytokines ? Cathelicidin initiated skin inflammation Mast Cells – in skin Could a trigger cause the bone marrow to produce mast cells? Muto. J Invest Dermatol. 2014; 134: 2728 -36 Barbara. Neurogastroenterol Motil. 2006; 18: 6 -17.

Systemic Cytokines in Rosacea • 60 rosacea pts vs. 25 controls • IL-18: 163 vs. 16 pg/ml (P<0. 01) • • • IL-6 lower in rosacea TNF-alpha numerically higher IL-8 not measured Salamon. Przegi Lek 2008; 65: 371 -4.
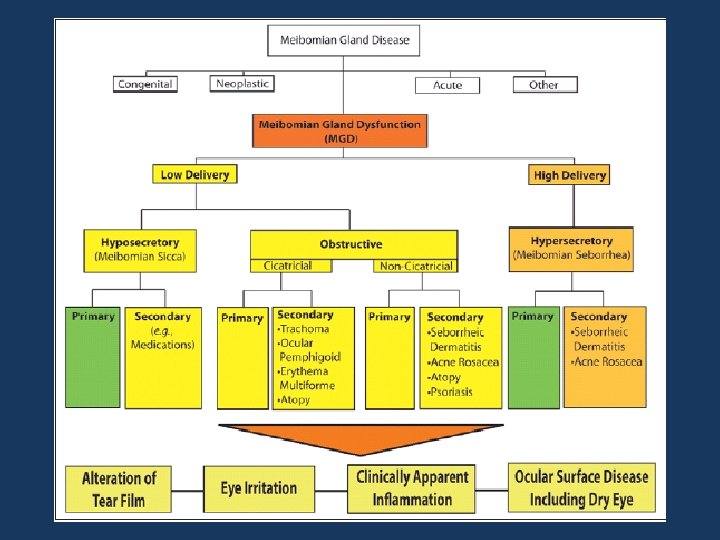

Clinical Summary of the MGD Staging Used to Guide Treatment Stage MGD Grade Symptoms Corneal Staining 1 + (minimally altered expressibility and secretion quality) None 2 ++ (mildly altered expressibility and secretion quality) Minimal to Mild None to limited 3 +++ (moderately altered expressibility Moderate and secretion quality) Mild to moderate; mainly peripheral 4 ++++ (severely altered expressibility Marked and secretion quality) Marked; central in addition “Plus” disease Co-existing or accompanying disorders of the ocular surface and/or eyelids Geerling G, Tauber J, Baudouin C, et al. The international workshop on meibomian gland dysfunction: report of the subcommittee on management and treatment of meibomian gland dysfunction. Investigative ophthalmology & visual science. Mar 2011; 52(4): 2050 -2064.

Diabetes • Meibomian gland dysfunction study in a general population • N=619 people with and without eye sx • Asx MGD in 22% • Diabetes OR = 2. 2 2013 study: Viso et al. Invest Opthalmol Vis Sci 2012; 53: 2601 -6. Spoendlin et al. J Invest Dermatol 2013; 133: 2790 -3.
 • Sx MGD in 8. 6% of")
Rheumatoid arthritis • MGD study (cont. ) • Sx MGD in 8. 6% of population • Facial rosacea pts: OR = 3. 5 • Rheumatoid arthritis pts: OR = 16. 5 Keratoconjunctivitis common eye disease in RA RA seen in some neurogenic rosacea pts Viso et al. Invest Opthalmol Vis Sci 2012; 53: 2601 -6. Hamideh. Semin Arthritis Rheum 2001; 30: 217 -41. Scharshmidt et al. Arch Dermatol 2011; 147: 123 -6.

Crohn’s disease – Incidence of 5/60 consecutive CD clinic pts – 3 active rosacea: treated with rifaximin: 1 partial and 2 complete response – 2 not active (for both conditions) – Cases included: • 60 y. o. F w 40 yr ileitis on no Rx CD flares assoc w nasal rosacea – Rx - cleared • 46 y. o. M 26 yr CD s/p IC resection on 6 -MP CD flares assoc w facial rosacea – Rx - cleared • 32 y. o. F – see next Weinstock. J Clin Gastroenterol 2011; 45: 295 -297.
 Rosacea ?")
Theoretical links in pathophysiogy SIBO Systemic IL-8 (or IL-6/TNF, IL-18 in NASH) Rosacea ? Upregulates local immune & inflm. LPS, IL-8 and integrin B-7 ? Increases dermal vascular permeability Systemic substance P ? Neurogenic inflam. or incr. in collagenase and bacterial virulence* FODMAPs/bacterial activity Histamine foods and mast cells ? Food triggers *Miljouin. PLo. S One 2013

Role of Mast Cells in IBS Normal IBS Abdominal pain and severity correlated with the number of mast cells <5µm Proximity to nerves Elevated tryptase and histamine Barbara. Gastroenterology. 2004; 126: 3.

Rosacea food triggers • Direct • Hot temperature • Histamine foods • Indirect • FODMAPs • Spicy food • History • 1926 – Carbohydrate intolerance (Kendall) • 1966 – GI sx but Nl mucosal enzyme activity • 2008 -13 – SIBO link and risks of FODMAPs

Food triggers: GI perspective • Spicy food • Increase capsaicin • Hot drinks • Release vasoactive proteins • Histamine foods • Activation of mast cells • FODMAP foods • • • Increase fermentation & inflammation Substance P Hydrogen sulfide
 • Fruit (13%) – – – Citrus fruits Red plums")
• Alcohol (52%) • Fruit (13%) – – – Citrus fruits Red plums Raisins & figs Tomatoes Bananas • Dairy (8%) – Aged cheese – Yogurt • Vegetables – – Broad-leaf beans & pods Avocado Eggplant Spinach Wilkin J, National Rosacea Society Survey. • • • Spicy food (45%) Hot drinks (36%) Histamine foods – – – Red wine Aged cheese Yogurt Beer Bacon • Other triggers – – – Chocolate Vanilla Soy sauce Yeast extract Vinegar Liver

H. pylori controversy • Local gastric infection with systemic immune changes • Cag-A more virulent – prevalent in Poland & China • A possible “coincidence” H. pylori Rx also treats SIBO and also rosacea – which one explains phenomenon observed in H. p. pts? the

H. pylori: “plausible study” • N=60, 31 -72 y. o. Polish pts with P/P/E/F • 60 age- & gender-matched NUD pts w/o rosacea • Hp prevalence in rosacea 88% vs. 65% in NUD • Rosacea pts: 67% were cytotoxin-associated gene A (CAG-A) positive vs. 32% of controls pts • OCM Rx: 51/53 rosacea pts became Hp • Within 2 -4 wks rosacea disappeared in 51, markedly declined in 1 and remained unchanged in 1 subject • Rx decreased IL-8 (65%) and TNF-alpha (72%) Szlachcic et al J Physiol Pharmacol. 1999; 50: 777 -86.
- Slides: 54