Occupational Disorders From Exposure to Radiation By DR

Occupational Disorders From Exposure to Radiation By DR Nanees Ghareeb

Occupational Disorders From Ionizing Radiation: § Types & properties of ionizing radiation: -Ionizing radiation (electromagnetic & particulate) varies in natural source, energy, frequency and permeability but all share the ability to ionize incident materials. -The radiation disrupts chemical bonds, which causes molecular excitation and production of free ions & high reactive, free radicals, leading to disruption of cellular function. -The clinical presentation and severity of illness are determined by the dosage, body distribution and duration of exposure.

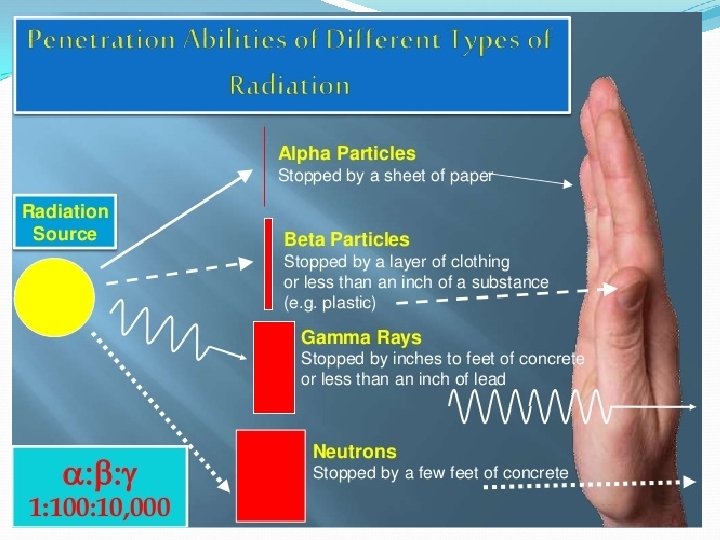
-Tissues with the most rapid cellular turnover are the most radiosensitive (e. g. reproductive, hematopoietic, gastro intestinal tissues). - Ionizing radiation consist of two types: ü Electromagnetic radiation (e. g. X-rays & gamma rays). They possess no mass, no charge and are characterized by extremely short wave length & high energy & frequency). ü The particulate radiations: consist of electrons, protons, neutrons, alpha particles, Beta particles, heavy charged ions and other atomic particles varying in nature & charge: - On external exposure, Beta particles can penetrate skin poorly, whereas alpha particles do not penetrate at all. - Internal exposure to alpha or beta particles by inhalation, implantation or ingestion cause acute or delayed injury.

-Within the body, the distribution and retention of each internally deposited radionuclides is governed by both its physical decay (its physical half life), (radioactivity level to the half) which vary from seconds to years, and its biological removal (its biological half life). - Radiation injuries include 2 types: ü Stochastic injuries which is assumed to lack dose threshold (e. g. mutagenic and carcinogenic injuries or effects), which are viewed as a probabilistic effects that can result from radiation induced changes in single cell within affected organs. ü Non stochastic injuries which cause acute and chronic tissue reactions that result from the killing of large numbers of cells in affected organ (e. g. erythema of skin, depression of blood count, oligospermia, cataract of the lens). Dose related.

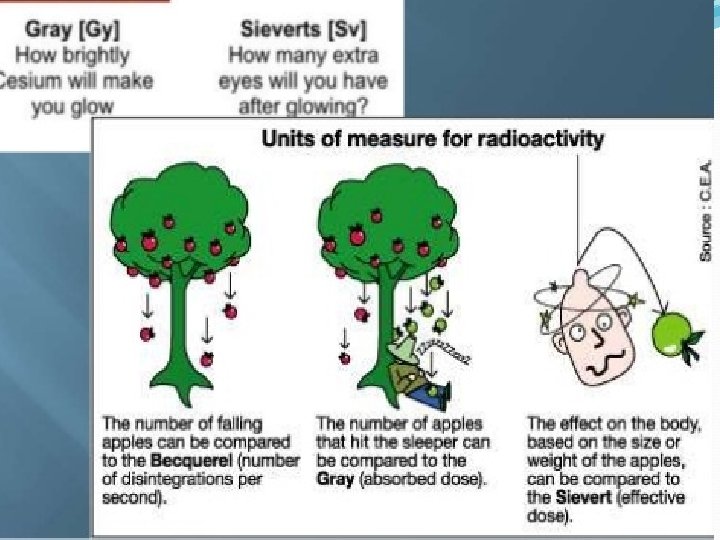
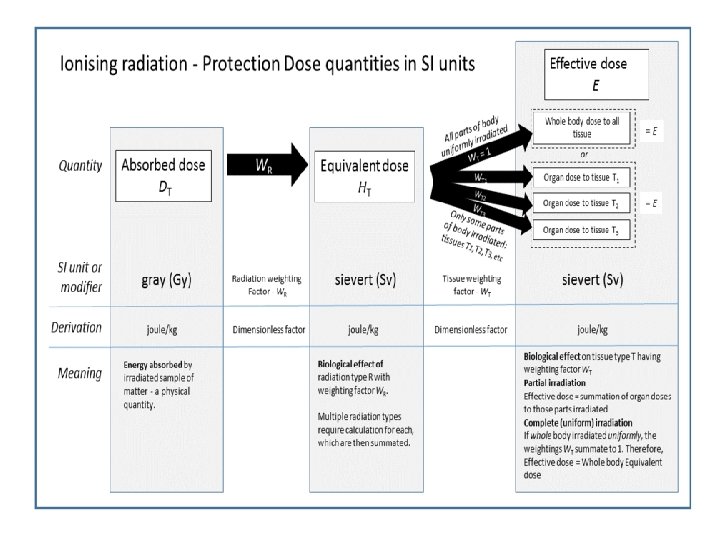
The maximum exposure limit for occupationally exposed worker is 50 m. Sv (5 rem) in any given year. Ionizing radiation are quantitively measured according to 2 systems: - The old centimeter-gram second (cgs) system (rad & rem) - The recent international system (SI): ü SI unite for radiation absorbed dose the gray (Gy) = 100 rad. ü SI unite for radiation equivalent dose the Sievert(SV)=100 rem ü SI unite for expressing the amount of radioactivity in a sample of matter is the Becquerel (Bq) Bq= quantity of radioactivity in which there is one atomic disintegration per second while cgs unites used for the same purpose is the Curi. I Curi= 3. 7 × 10 10 atomic disintegration per second = 3. 7 × 1010 Bq.

1 Rontgen = amount of X-ray that produces one electrostatic unite of charge in one cubic centimeter under standard condition of temperature and pressure. - Exposure of the skin to one Rontgen X-ray typically deposits a dose slightly <(1 rad) in underlying epidermis. v Sources and levels of ionizing radiation in the environment: - Ionizing radiation arise either from natural or artificial sources: A- Natural sources include three main sources: ü Cosmic rays which arise in outer space and its intensity varies with altitude by a factor of 2 or more than at sea level. ü Terrestrial radiation which emanates from radium, uranium and thorium in the earth’s crust which also varies markedly from one geographical region to another.

Radon exposure in indoor airs which affect the bronchial epithelium. ü Internal radiation which is emitted by potassium 40 (k 40) and other naturally occurring radionuclides normally present in the body B- Artificial sources include: X-ray diagnosis , nuclear medicine, consumer products e. g. (color TV, smoke detectors), occupational , atomic weapons fall out. v. High risk occupational groups are: Radiologists, uranium miners, radium dial painters, nuclear power plant operations, petroleum refinery workers.

q Acute effect of ionizing irradiation: - Generalized effect due to brief but heavy exposure of all or part of the body (acute radiation syndrome). - Localized effect: • Effect at cellular level (gene mutation, chromosome aberrations and cytotoxic effect). • Effect on tissues or organs, particular relevance to occupational or accidental irradiation (e. g. skin, blood forming tissues, reproductive organs, gastrointestinal tract and eye lens). ü Generalized effect of radiation exposure (acute radiation syndrome): - Exposure to whole body or major part of hematopoietic system, GIT, lung, brain is the cause of this syndrome. - Symptoms & prognosis depend on the degree of exposure & the equivalent absorbed dose.
 Exposure to < 1 SV, is unlikely to produce symptoms but laboratory abnormality")
1) Exposure to < 1 SV, is unlikely to produce symptoms but laboratory abnormality may be detected. Asymptomatic 2) Exposure to 1 - 6 SV is followed by: - Prodromal symptoms of vomiting & diarrhea 3 hours after exposure followed by a latent period of symptom free interval. - Leading organ effects: the hematopoietic tissue characterized by moderate leucopenia, thrombocytopenia & hair loss after 4 - 6 weeks - Therapy includes reassurance & hematologic follow up. - Prognosis good. - Convalescent period several weeks - 12 months. 3) Exposure to 6 - 10 SV induce: (acute pneumonitis) -Prodromal symptoms after a shorter period 1 - 2 hrs after exposure. - Leading organ affected (haematopoietic tissue, sharing severe leucopenia, purpura, hemorrhage & infection, hair loss also occur usually 4 - 6 weeks after exposure.

- Therapy : blood transfusion or bone marrow. - Prognosis: guarded. - Convalescent period long < 1 year. - Recovery up to 20%. 4) Exposure to 10 - 50 SV course: - Prodromal symptoms 30 minutes after exposure. - Leading organ affected: Gastrointestinal tissue leading to diarrhea, fever, disturbance of electrolytes & prostration usually occurs 1 - 2 weeks after exposure. - Therapy: maintenance of electrolytic imbalance & antibiotics. - Prognosis: hopeless. - Recovery: nil death within 2 weeks. 5) Exposure to 50 SV induce: - Prodromal symptoms immediate or within 30 minutes.

- Leading organ affected CNS characterized by convulsions, tremors, ataxia which occurs with 1 - 48 hours. - Therapy: sedatives. - Prognosis: hopeless. - Recovery: nil death occurs within 2 days. § N. B: -Exposure to (6 - 10 SV) can also cause acute radiation pneumonitis within 1 -3 months. If extensive the process may terminate in respiratory failure, pulmonary fibrosis and core-pulmonale , months - years later. - The prodromal period may be followed by a latent period of apparent well being which may be shortened or absent with exposure to higher doses.
Effects at cellular levels: v Gene mutation: -")
ü Localized effects of acute radiation: 1)Effects at cellular levels: v Gene mutation: - Radiation may alter DNA sequence within the cell even in a single gene and irreversibly alter or kill the cell. - Mutagenic effects of radiation have not yet been documented in germ cells but well demonstrated in somatic cells. v Chromosomal aberration (structure or number): two event chromosome aberration of lymphocytes resulting from interference of radiation with either chromosomal segregation during their cell division or by causing chromosomal breaking, v Cytotoxic effects: high dose of radiation may be able to kill any cell but a small dose can render most human cells
Effects on tissues & organs relevant to occupational exposure: v Effects on skin: -")
2)Effects on tissues & organs relevant to occupational exposure: v Effects on skin: - The earliest reaction is erythema. - Erythema become evident with 2 hours after rapid exposure to 6 Gy, lasts for few hours to be followed 2 - 4 weeks later by deeper and more persistent erythema. - Also the skin may become dry, smooth shiny, thin, sensitive and pruritic, and there are signs of telangiectasia, atrophy and diffuse pigmentation. The nails may appear white and striated. - The other effect is epilation. The threshold for temporary epilation is lower than that for erythema.

v Effects on blood forming organs: - Hematopoietic cells are highly sensitive to radiation and undergo degenerative changes within minutes after a dose of one SV. - Similarly lymphocytes are highly radiosensitive and a dose of 1 - 6 SV whole body irradiation is sufficient to cause prompt lymphopenia with profound depression in the immune response. v Effects on gastro intestinal tract: When a large part of the small intestine is exposed to dose > 10 SV, fulminant dysentery like reaction is produced due to ulceration of intestinal mucosa which may cause death from days to 2 weeks after exposure. v Effects on Reproductive organs: - Immature spermatogonia and oocytes are highly radiosensitive and a small dose (0. 15 SV) sufficient to depress sperm count temporarily. - Permanent sterility may result from a dose in excess of 4 SV.

v. Effects on Lens of the eyes: Posterior sub capsular opacity can be detected microscopically after a dose of 1 SV a single brief exposure. But the threshold for a vision, impairing cataract is estimated to vary from about 2 - 4 SV. q Delayed or chronic effect of radiation: ü Delayed general effects including: - Premature ageing - Shortening of life span ü Delayed Local effects (carcinogenic effects and scarring) which follows: - Whole body exposure (e. g. in atomic bomb survivors). - After localized organ exposure (e. g. lung cancer in uranium miners, liver cancer associated with thorium dioxide and scarring of tissues after receiving radiotherapy.

Ø The carcinogenic effects of radiation: leukemia, cancer of the breast and cancer of the thyroid. Ø The scarring effects in other tissues: High dose of radiation exposure has lead to endarteritis obliterans, intestinal stenosis, pulmonary fibrosis and cataract. § Maximum permissible doses for occupational exposures are: - For protection against stochastic effect: Annual (effective dose) 50 m. Sv. - For protection against non stochastic effects in individual organs: Annual effective dose for lens of the eye 150 m. Sv. Annual effective dose for all other organs 500 m. Sv.

§ In case of radiation accidents the following measures should be taken: - Clinical evaluation of workers including injuries other than radiation (e. g. burns, smoke inhalation or trauma). - Person who handles the worker should wear protective gloves or clothes. - The contaminated victim should be isolated &decontaminated by carefully rinsed with water & the rinsed water isolated as radioactive waste.

- If radioactivity are inhaled, oral &nasal cavities should be rinsed with water (avoid swallowing any). - Management of the victim should be followed and treated according to the degree of exposure as discussed before under acute whole body irradiation. - Good recording for signs & symptoms & environmental measures should be carefully done & kept. § Doses involved in medicine and dentistry must be limited as possible. this can be achieved by: - Limiting number of radiographs / patient. - Limiting size of the field exposed. - Limiting of use of fluoroscopy as possible. - Shielding tissues outside the field especially fetus & gonads.
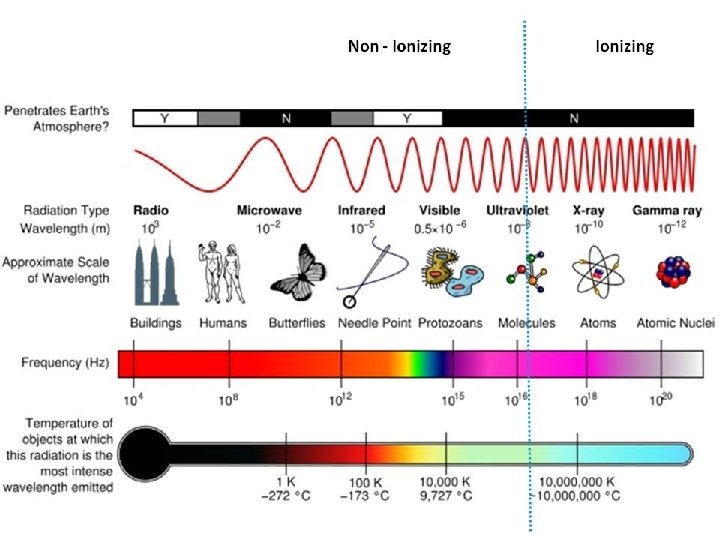
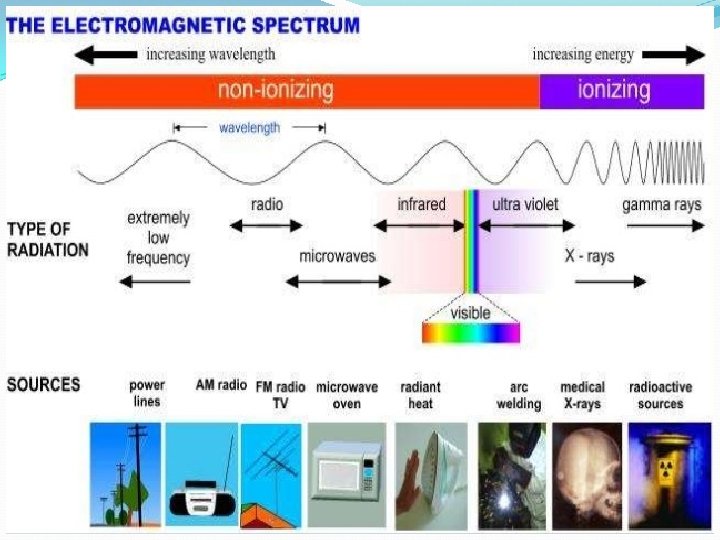

OCCUPATIONAL DISORDERS OF NON – IONIZING RADIATION The term non ionizing radiation designates a wide spectrum of electromagnetic radiation frequency (from 0 HZ- 1015 Hz) and therefore has potentially a variety of health effects. They include extremely low frequency and static electromagnetic fields, lasers, ultraviolet radiation, radiofrequency and microwave radiation and ultrasound. 1)Extremely low frequency and static electromagnetic fields (EMFs): They comprise frequencies between 1 to 3000 HZ but the ones of most interest are 50 to 60 HZ fields associated with alternating currents in electric power distribution systems , MRI and various electric appliances.

ü In vitro experiments suggest affection of cell function as follows: - Modulation of ion and protein flow across the cell membrane. - Chromosome damage and interference with DNA synthesis and RNA transcription. - Interaction with the cell response to different hormones and enzymes, - Interaction with the immune response of cells. - Interaction with cancerous cells. (Reproductive effect, Neurological effect and cancer effect) • 2)Radiofrequency & microwave radiation: - Radiofrequency (RF) µwave radiation consist of energy in wave form traveling in free space as the speed of light. - It is composed of separate electric &magnetic field victors, both are perpendicular to each other.

ü Exposed groups include: - Radio, TV and microwave transmitters. - Radar workers, cellular phones - Power transmission line workers & physiotherapists. ü Effects of RF & microwave radiation: A) A thermal effect which result from acute exposure to high levels and characterized by protein denaturation and tissue necrosis at the site of thermal exposure. 1) General effects: Irritability, headache, vertigo, watery eyes and gritty eye sensation, dysphagia, anorexia, abdominal cramps & nausea. Hypertension developed 1 - 3 months after exposure & resolves with treatment and posttraumatic stress disorder with emotional liability and insomnia persisting for as long as 1 year. (Gulf war)
Localized effects : Feeling of hotness, burning sensation of exposed skin, later within few")
2)Localized effects : Feeling of hotness, burning sensation of exposed skin, later within few days localized thermal induced masses occur due to interstitial edema and coagulation necrosis (thermal effect) accompanied by erythema & vesiculation. B) Effect of low dose exposure (Non- thermal effects): (still not confirmed). - Possible teratogenicity based on finding of chromosomal breaks in power station workers, - Some evidence of carcinogenicity (e. g. brain tumor, malignant melanoma & leukemia) - Cataract formation but no well documented studies
Injuries due to infrared radiation: - Infrared radiation covers the portion of the")
ü 3)Injuries due to infrared radiation: - Infrared radiation covers the portion of the electromagnetic radiation between radiofrequency and visible radiation. - Cause molecular excitation and vibration, resulting in heat that is absorbed by tissues and can cause thermal injury to skin (sunburn)and eye (cornea, iris and lens (cataract)), particularly among glass blowers, furnace workers, welding and the drying and baking of coatings on consumer products. ü 4)Injuries of visible radiation: - Visible radiation (light) covers the portion of the electromagnetic spectrum between infrared and ultraviolet radiation (750 - 400 nm). - Workers at risk are those exposed to o Sunlight o High intensity lamps, lasers, spotlights o Welding arcs.
 Retinal affection causing solar retinitis (eclipse blinding) and retinal aging and senile macular")
A) Retinal affection causing solar retinitis (eclipse blinding) and retinal aging and senile macular degeneration. B) Temporary visual loss after image resulting from short bursts of high intensity light (flash blindness). C) Insufficient lightening or reflected light (glare) eye strain (asthenopia), visual fatigue, headache & eye irritation. D) 5) Injuries due to ultraviolet radiation (UV): - UV radiation covers the portion of the electromagnetic spectrum between visual radiation and ionizing radiation , there is three types : o UV-A o UV-B o UV-C. A)A & B bands representing the longer wavelengths & producing the most biological effects. B)C mostly filtered by ozone layer and most dangerous.
Eye effects: - Photokerato conjunctivitis (welder's flash): 6")
Clinical findings of UV exposure: A)Eye effects: - Photokerato conjunctivitis (welder's flash): 6 - 12 hours after exposure symptoms resolve within 48 hours. - Cataracts: both cortical & anterior polar cataract - Pterygium. B) Skin effects: - A. Erythema (sunburn): UV-B reacts with photo active substances present in skin & can cause erythema and delayed tanning. - B. Photosensitivity reactions: 2 types: phototoxic & photo allergic The phototoxic reactions: Usually occur in association with use of medication. Characterized by pigmentary changes along the pattern of points of sun contact & bullae in severe cases. Photoallergic reactions: (eczema) Photoallergic reaction occurs in association with bacteriostatic agents and perfume ingredients.
 Photo aging of skin: UV-B damage to the skin cause photo aging characterized")
C) Photo aging of skin: UV-B damage to the skin cause photo aging characterized by: wrinkling, mottled pigmentation, coarseness, telangiectasia, laxity & skin atrophy. D) Premalignant & malignant skin conditions: a- Cutaneous malignant melanoma. b- Non melanotic skin cancer. Prevention: - Protection by adequate use of screening ointments routinely for children particularly those containing sun protective factor (SPF) of 15 or higher to protect against both UV-B & UV-A. - Avoid exposure solar UVR at their peak of exposure (60% of solar UVB reaches earth between 10 AM & 3 PM). - Duration of exposure should be limited to decrease sunburn.

Thank you
- Slides: 40