OCCIPITOPOSTERIOR FACE AND BROW PRESENTATION BY DR TAMER

OCCIPITO-POSTERIOR, FACE, AND BROW PRESENTATION BY DR. TAMER M. ABDEL-AZIZ, M. D. , LECTURER OBSTETRICS AND GYNECOLOGY, FACULTY OF MEDICINE, ALEXANDRIA UNIVERSITY

OCCIPITO-POSTERIOR POSITION

DEFINITION • The vertex presentation in which the back of the fetus and the occiput are directed posteriorly; either directly, or right or left.
. • During early period")
INCIDENCE • During antenatal period the incidence is high (40%). • During early period of labor (30%). • Right occipito-posterior is higher than left: Due to the sigmoid colon is in the left oblique diameter.
 I. Passenger (fetal) 1. 2. 3. 4. 5. 6. 7.")
ETIOLOGY (for all malpresentations) I. Passenger (fetal) 1. 2. 3. 4. 5. 6. 7. 8. 9. Prematurity Large fetus Congenital abnormalities Multiple pregnancies IUFD Placenta praevia Polyhdyrmanios Long cord Short cord II. Power (uterine) 1. Congenital abnormalities in the uterus 2. Pendulous abdomen 3. Tumours (fibroids) III. Passage (pelvis) Contracted pelvis (anthropoid pelvis android pelvis)

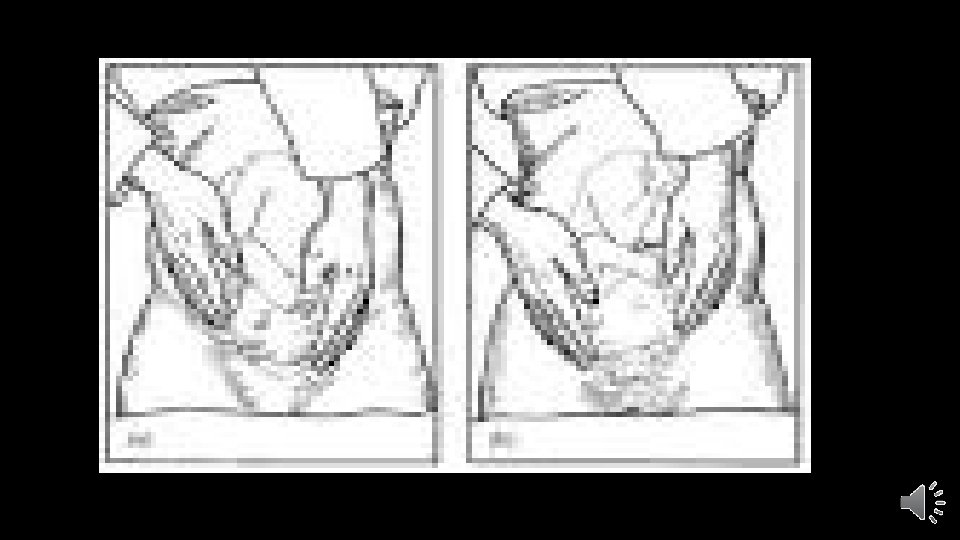
DIAGNOSIS • INSPECTION: 1. Loss of normal abdominal contour with flattening and lower part shows a bulge 2. A groove is seen across the abdomen below the umbilicus due to depression between the trunk and forehead. 3. Fetal movements seen allover the abdomen.

• PALPATION: 1. FUNDAL LEVEL: • Higher than normal, due to delay engagement of head. 2. FUNDAL GRIP: • BREECH occupying the fundus 3. LATERAL GRIP: • FETAL LIMBS are felt near the midline • FETAL BACK is felt far away form the midline on the flanks and difficult 4. PELVIC GRIP: • Head shows a degree of deflexion and not engaged 5. PAWLICK GRIP: • Head feel smaller and recedes from the examining hand which grasping its sincipital end and not its occipital end.

• AUSCULTAION: • Localization of the fetal heart sounds are difficult because fetal limbs are between the fetal chest and abdominal wall. • VAGINAL EXAMINATION: (during labour) • Posterior fontanelle is felt with difficulty towards the sacro-iliac joint (deflexion) • Anterior fontanelle is felt with ease towards the ilio-pectineal eminence • SONOGAPHY: much easier and simpler
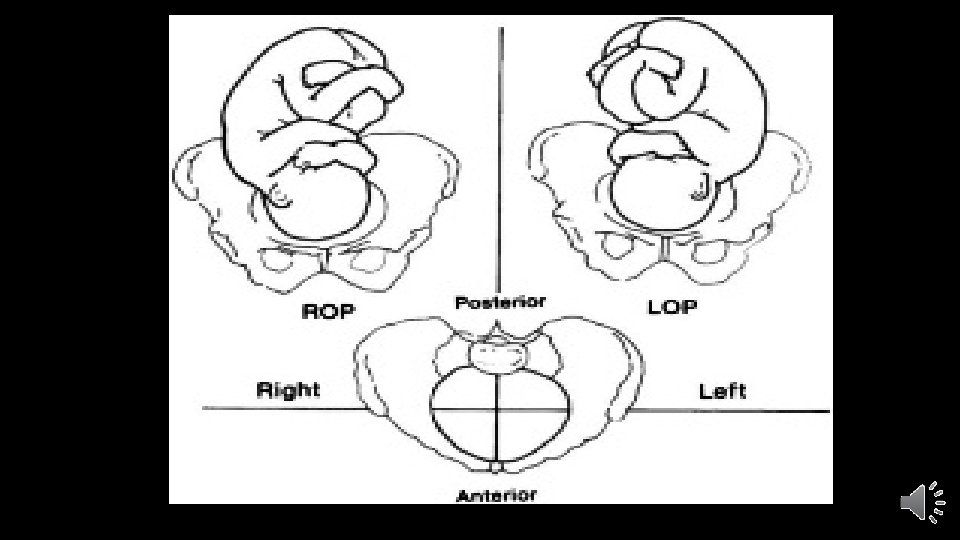

MECHANISM OF LABOUR • The head engages through the right oblique diameter in ROP and left oblique diameter in LOP. • The engaging transverse diameter of the head is biparietal (9. 5 cm) and that antero-posterior diameter is either sub-occipito-frontal (10 cm) or occipito-frontal (11. 25 cm) • Because of the deflexion, engagement is delayed.

• FACTORS GOVERNING THE MECHANISM OF DELIVERY IN OP: 1. The position of the head with the occiput posterior 2. The deflexed attitude of the head which caused by: 1. Opposition of the back of the fetus against the convexity of the maternal spine interfering with the flexion of the head. 2. The large biparietal diameter is entering the small sacro-cotyloid diameter of the pelvic brim (9 cm); while the small bitemporal diameter is entering in the opposite wide oblique diameter and hence the sinciput decscends more readily leading to deflexion. 3. 4. 5. 6. The cause of the posterior position The shape and type of pelvis The uterine action and time of rupture of membranes The size of the fetal head
 • The head")
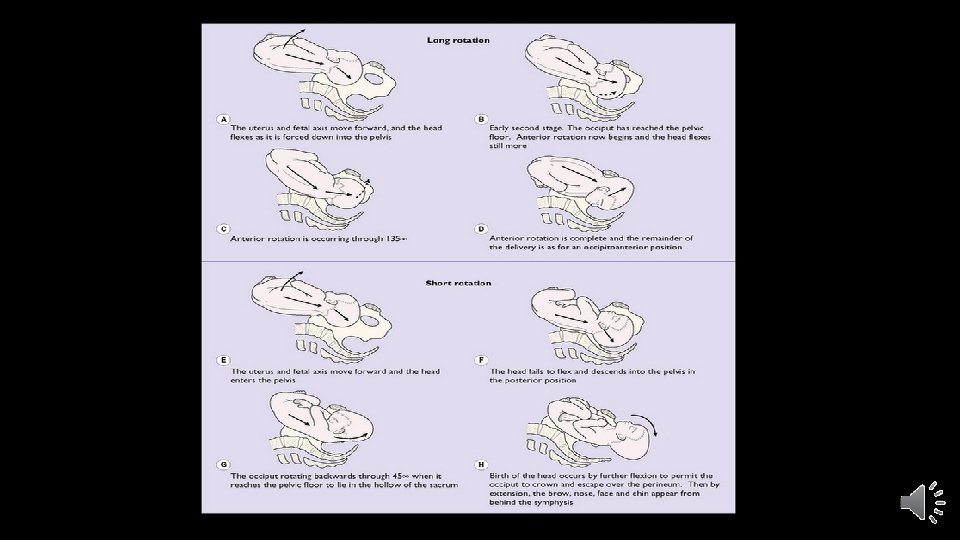
FATE OF OCCIPITO-POSTERIOR PRESENTATION 1. Long anterior rotation of occiput (90%) • The head rotates 3/8 th of a circle anteriorly and becomes occiptioanterior position. • Favorable circumstances • The head becomes fully flexed.

2. Short posterior rotation of occiput • the head rotates 1/8 th of a circle posteriorly and becomes face to pubis • Becomes direct occipito-posterior • Flexion occurs and extension of the face will be delivered.

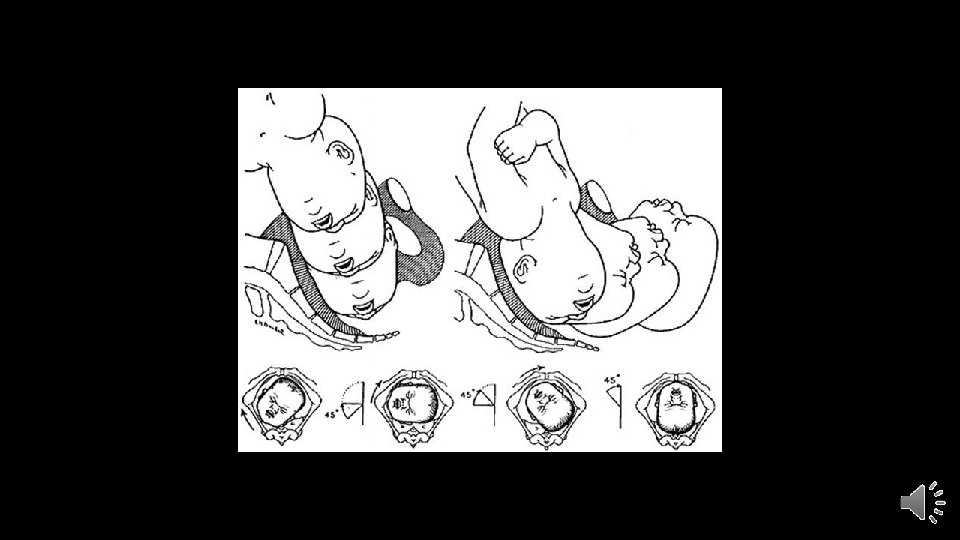
3. Incomplete anterior rotation of the occiput: • • • The head rotates 1/8 th of a circle anteriorly and becomes transverse (deep transverse arrest) not deliverable. The anter-posterior diameter of deflexed head is 11. 25 c, while the interschieal spinous diameter 10. 5 cm

4. Non-rotation of the occiput: • The head does not rotate and stays persistent occipitoposterior, • not deliverable

• The good omens of spontaneous anterior rotation of the occiput: 1. 2. 3. 4. Good uterine action Intact membranes Full flexion of the head Good shape and size of the pelvis
 3. Injuries")
COMPLICATIONS • MATERNAL: 1. Prolonged labor and/or maternal distress 2. Infection (PROM) 3. Injuries in birth canal 4. Atonic and traumatic postpartum hemorrhage 5. Obstructed labor 6. Lacerations and damage of soft tissue 7. Puerperal sepsis • FETAL: 1. 2. 3. 4. 5. 6. Fetal asphyxia Fetal intra-cranial injuries Excessive moulding of fetal head Cord prolapse Fetal and neonatal infections Fetal injuries due to instrumental delivery

MANAGEMENT • PRINCIPLES: 1. Early diagnosis 2. Strict vigilance with watchful expectancy hoping for descent and anterior rotation of the occiput 3. Judicious and timely interference, if necessary.

• DURING FIRST STAGE OF LABOR: WATCHFUL EXPECTANCY: 1. Prevent PROM by: a. minimizing vaginal examination, b. avoid straining and keeping patient in bed. c. If PROM occurs, vaginal examination must be done to exclude cord prolapse 2. Maintain physical condition of patient by proper nourishment and assure psyche by assurance and sedation 3. Keep the bladder and rectum empty. 4. Close observation of the mother and fetus for signs of distress.

• DURING SECOND STAGE OF LABOR: • Look for good omens for anterior rotation of the occiput. • If not; 1. MANUAL ROTATION FOLLOWED BY FORCEPS EXTRACTION: • Pelvis adequate • Baby size average • Good liquor 2. FORCEPS ROTATION AND EXTRACTION (by expert using KEILLAND FORCEPS) 3. VENTOUS (Vacuum extraction) 4. C. S. ; indications: • • • Pelvic contraction Old primigravida Fetal distress Cord prolapse Non-engagement of the head.

Scheme of management of OP EARLY DIAGNOSIS CAREFUL MONITROING OF LABOR TIMELY INTERFERENCE WATCHFUL EXPECTANCY ANTERIOR ROTATION (90%) EARLY C. S POP • Spontaneous • Ventouse • Forceps SHORT ANTERIOR NON-ROTATION SHORT POSTERIOR ROTATION (DTA) ASSISTED DELIVERY (FORCEPS/VENTOUSE), if adequate pelvis CS, if pelvis no adequate face to pubis delivery if arrest above ischial spines, CS

FACE PRESENTATION

DEFINITION • The head is completely extended and hence the face lies lower most.

TYPES • PRIMARY FACE PRESENTATION: • Rare • Head is completely extended before the onset of labor • SECONDARY FACE PRESENTATION: • Much commoner • During descent of head, it becomes more and more deflexed
 1. First position (right mento-posterior) 2.")
POSITIONS • The denominator is the chin (mentum) 1. First position (right mento-posterior) 2. Second position (left mento-posterior) 3. Third position (left mento-anterior) 4. Fourth position (right mento-anterior)

DIAGNOSIS • INSPECTION: • MPP; bulge in suprapubic region and groove blow the umbilicus, owing to the depression between the bulk of the head and back of the fetus. • MAP; multiple small irregularities (limbs) and fetal movements allover the abdomen.

• PALPATION: • FUNDAL GRIP: • Breech occupying the fundus • LATERAL GRIP: • MPP; back is concave, so not felt • MAP; limbs felt with un ease. • PELVIC GRIP: • Occipital end higher level than chin • Cephalic end on same side of the back • PAWLICK GRIP: • Characteristics of head

• VAGINAL EXAMINATION: • The following can be felt: • • • Orbital margins Alae nasi Alveolar margins Mouth Chin • SONOGRAPHY: confirms diagnosis

ENGAGEMENT OF HEAD IN FACE PRESENTATION • The engaging diameters of face presentation are: • Submento-bregmatic (9. 5 cm) • Bitemporal (8. 5 cm) • The head in face presentation is said to be engaged only when the biparietal diameter enters the pelvic inlet • The chin may be quite low in the pelvis, yet the head is not yet engaged, which is much higher than the bitemporal, is still above the pelvic brim.

MECHANISM OF LABOUR • MENTO-ANTERIOR: 1. 2. 3. 4. 5. 6. Descent Increased extension Internal rotation Flexion Restitution External rotation • MENTO-POSTERIOR: • FATE AS OCCIPITO-POSTERIOR: 1. 2. 3. 4. Long anterior rotation to become mento-anterior Short anterior rotation to become deep transverse arrest non deliverable Non-rotation to stay mento-posterior non deliverable Rotates posteriorly to direct mento-posterior (non –deliverable)

MANAGEMENT SAME AS OPP

BROW PRESENTATION

BROW PRESENTATION • DEFINTION: • The head in brow presentation is mid-way between flexion and extension i. e. deflexed. • DENOMINATOR: frontal bone • IF transient wait • If persistent: C. S.

THANK YOU
- Slides: 37