OBTURATOR NERVE BY DR VINEETA WALDIA ASSISTANT PROFESSOR

OBTURATOR NERVE BY DR. VINEETA WALDIA ASSISTANT PROFESSOR DEPARTMENT OF SHARIR RACHNA H. A. M. C. H. , DEHRADUN, UK. CONTACT NO. 8006969188

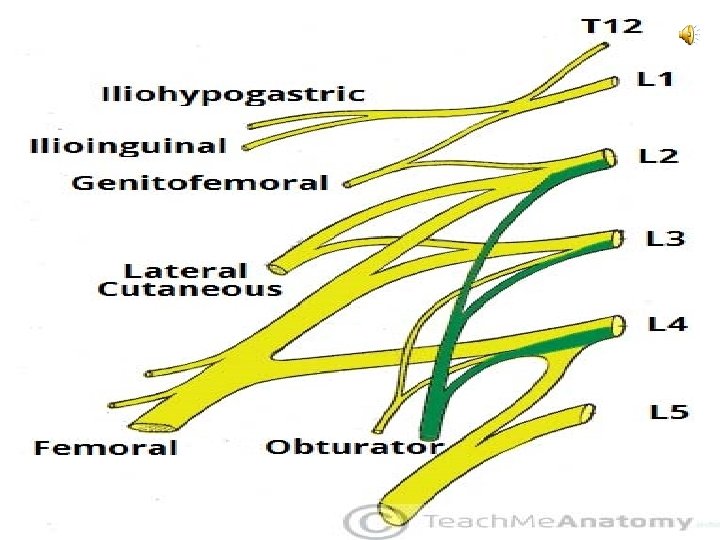
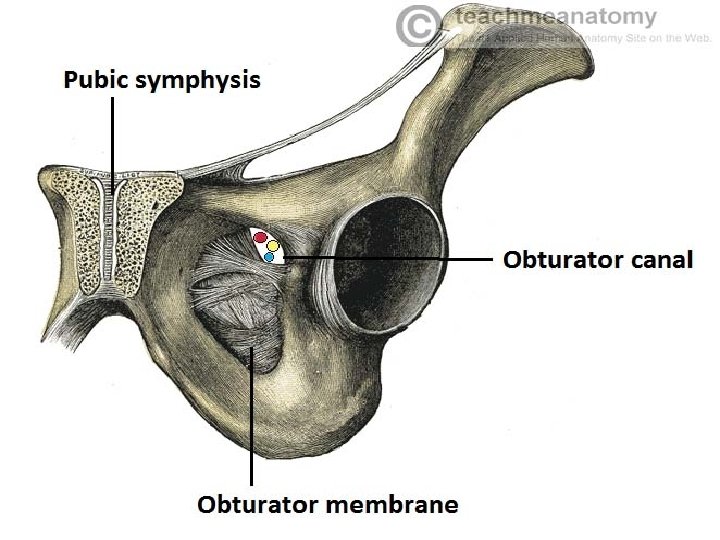
INTRODUCTION, ORIGIN AND ROOT VALUE • Chief nerve of the medial compartment of the thigh • The obturator nerve is formed from the lumbar plexus. It receives fibres from the anterior divisions of L 2, L 3 and L 4. • After its formation, the obturator nerve descends through the fibres of the psoas major and emerges from its medial border. It then travels posteriorly to the common iliac arteries and laterally along the pelvic wall – towards the obturator foramen of the pelvis. • The obturator nerve enters the medial thigh via the obturator canal (formed within the obturator foramen by the obturator membrane). It then divides into anterior and posterior branches.

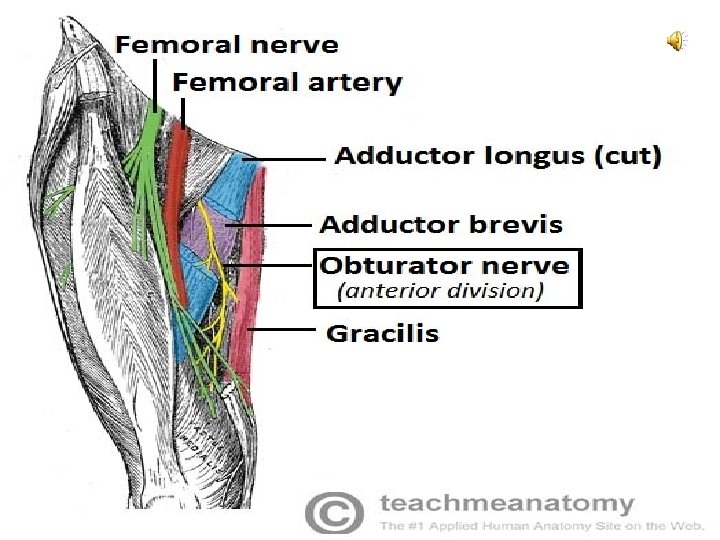
COURSE, BRANCHES AND INNERVATION ANTERIOR DIVISION: Passes downwards in front of the obturator externus being seperated from the posterior division by few fibres of this muscle and then descends behind the pectineus and adductor longus and in front of the adductor brevis Supplies: 1. Pectineus 2. Adductor longus 3. Gracilis 4. Adductor brevis; if not supplied by posterior division Also supplies the hip joint and ends in the subsartorial plexus

Posterior division: Passes through the obturator externus muscle and then travels behind the adductor brevis and infront of the adductor magnus. Supplies: 1. Obturator externus 2. Adductor magnus 3. Adductor brevis; if not supplied by the anterior division Ends in a genicular branch that supplies the capsule and cruciate ligaments of the knee joint.

SENSORY INNERVATION The cutaneous branch of the obturator nerve supplies the skin of the middle part of the medial thigh.

CLINICAL ANATOMY DAMAGE TO THE OBTURATOR NERVE • The obturator nerve can be damaged during surgery involving the pelvis or abdomen. • Symptoms include numbness and paraesthesia on the medial aspect of the thigh and weakness in adduction of the thigh. • Alternatively, the patient could present with posture and gait problems due to the loss of adduction.
- Slides: 9