OBSTRUCTIVE SLEEP APNEA effects on the body Charles

OBSTRUCTIVE SLEEP APNEA effects on the body Charles R. Davies, MD, Ph. D Carle Sleep Disorders Center
 Recognize")
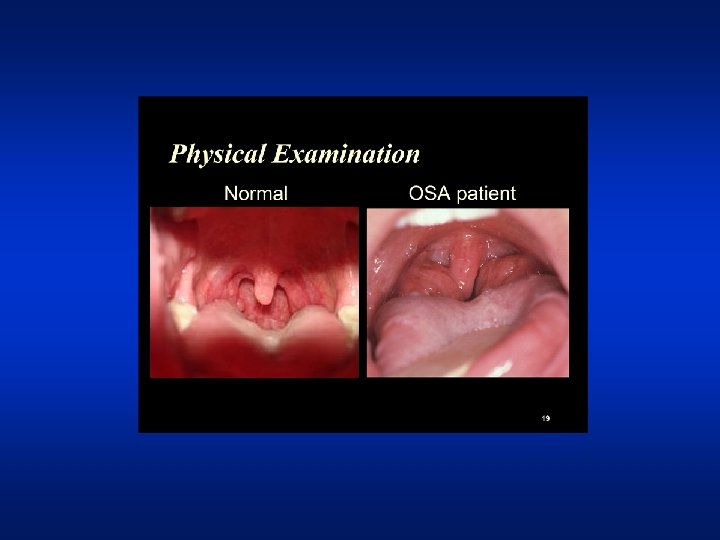
Objectives • Describe features and prevalence of • • obstructive sleep apnea (OSA) Recognize conditions associated with OSA Discuss OSA as an important risk factor for hypertension, CAD, stroke, and MVAs Identify persons at risk for OSA using a simple screening tool Be familiar with treatment options for OSA

OSA definitions • Apnea: cessation of airflow for >10 seconds • Hypopnea: reduction of airflow >30% for at • • least 10 seconds with a desaturation >4% Obstructive sleep apnea (OSA): repetitive interruption of ventilation during sleep caused by collapse of the pharyngeal airway Apnea-hypopnea index (AHI): number of apneas & hypopneas per hour of sleep (normal <5/hr)

Partial and complete airway obstruction

Pathophysiology of OSA

Normal Sleep Hypnogram

Snoring

Obstructive apnea

OSA 4 -minute segment

Epidemiology of Mod-Severe OSA • General Population – – 10 -17% of men* 3 -9% of women* ~2% of children increase with age & BMI in adults – 2 to 3 times risk in CVD • Hospital population – Increased risk factors imply increased prevalence, esp. age, obesity, CV disease – ~80% of bariatric surgery patients – “Latent” cases can become manifest in a hospital setting *Peppard et al. Am J Epidemiol 2013; 177(9): 1006 -14

Impact of Obesity

Obesity 2016 Source: CDC

OSA Risk Factors • Obesity; Neck circumference • Post menopausal state • Craniofacial abnormalities • Nasal deformities • Narrow posterior pharynx • Late night alcohol, sedatives

Conditions associated with OSA • Hypertension • Coronary artery disease • Cardiac Arrhythmias • LV Dysfunction • CHF • Nocturnal sudden death • Obesity • Stroke • GERD • Depression • Diabetes • MCI or Dementia

Prevalence of OSA in those with cardiovascular and cerebrovascular disease JACC 2003 41, 9; 1429 -37

SNA inc. with OSA SNA dec. With CPAP Rx Somers VK et al. J Clin Invest 1995; 96: 1897 -1904

Dose Response relationship between the severity of OSA based upon AHI and the adjusted odds ratio of HTN OR Adjusted for baseline HTN status, age, gender, habitus and weekly ETOH consumption NEJM 2000; 342: 1378 -84

OSA activation of CV disease mechanisms
: •")
Fatal Heart Attacks and Strokes in OSA • Untreated severe sleep apnea (AHI>30): • • • 1. 06/100 person-years Simple snorers (AHI<5): 0. 34/100 person-years Treated with CPAP: 0. 35/100 person-years Healthy pts: 0. 30/100 person-years Marin et al. Lancet 2005; 365: 1046 -1053

Cardiovascular Disease in OSA • Retrospective study of 6424 persons • 16% reported MI, angina, bypass surgery, heart • • • failure, or stroke Minimal OSA: 0. 98 (. 77 -1. 24) CVD odds ratio Mild OSA: 1. 28 (1. 02 -1. 61) CVD odds ratio Moderate OSA: 1. 42 (1. 13 -1. 78) CVD odds ratio Shahar E, et al. AJRCCM 2001; 163: 19 -25

Effects of Hypoxemia • Nocturnal angina • Arrhythmias • Impaired myocardial contractility • Coronary endothelial dysfunction • Pulmonary HTN

Coronary Endothelial Dysfunction • Vasoconstriction • Inflammation • Endothelial growth • Platelet proliferation • Increased adhesion molecules

Arrhythmias • Tachy-bradycardia • PACs/PVCs • SVT • A-V block • Atrial fibrillation

Atrial Fibrillation • 8. 9% in OSA* vs. 2% overall • 82% vs. 42% 12 month recurrence for untreated • vs. treated OSA Increased risk of Afib after CABG with OSA *Erdogan et al. Somnologie 2009; 13: 211

Negative intrathoracic pressure • Increased transmural wall stress • Increased myocardial O 2 • consumption Flash pulmonary edema

Systolic heart failure • LV Ejection fraction 53% in severe OSA vs. 61% • • • in control subjects 2. 5 fold increased risk of heart failure for OSA LV systolic dysfunction not due to ischemic disease Cor pulmonale due to pulmonary HTN

Diastolic heart failure • 36% impaired relaxation in OSA compared with • • • 27% in gen. pop. Increased pulmonary capillary pressure Increased left ventricular mass LVH
: • • odds ratio")
Stroke and OSA • Moderate to severe sleep apnea (AHI>20): • • odds ratio 4. 33 (1. 32 -14. 24) of having had a stroke Moderate to severe sleep apnea (AHI>20): odds ratio 3. 08 (0. 74 -12. 81) of having a first stroke over 4 yrs Adjusted for age, gender, and body-mass index Arzt et al. Am J Resp Care Crit Care Med 2005; 172(11): 1447 -1451.

Obesity, diabetes & OSA Decreased leptin & increased ghrelin

OSA Association With Diabetes • 1453 non-diabetic subjects with OSA • Followed for 13 yrs • Severe OSA was associated with 71% increased • • risk of incident DMII Dose dependent association noted Adjusted for age, gender, body mass index, smoking, alcohol use, and physical activity Nagayoshi et al. Sleep Med. 2016; 25: 156 -161

Intermittent hypoxia Effect on Glucose and Insulin • 13 subjects • Int. hypoxia to ~70% • for 8 hrs Glucose and insulin given IV Louis & Punjabi J Appl Physiol. 2009; 106: 1538 -1544

OSA severity and Glycated Hgb • 1599 patients having sleep • • study Patients with diabetes were excluded Oxygen desaturation associated with greater risk for Hgb. A 1 c >6. 0 Priou, Le Vaillant et al. Diabetes Care epub 2012
: • • relative")
Motor Vehicle Accidents • Mild sleep apnea (AHI 5 to <15): • • relative risk 2. 6 (1. 7 -2. 9)* Moderate sleep apnea (AHI 15 to 30): relative risk 1. 9 (1. 2 -2. 8)* Severe sleep apnea (AHI >30): relative risk 2. 0 (1. 4 -3. 0)* *compared with controls (AHI<5) Mulgrew et al. Thorax 2008; 63(6): 536 -41.

Increased Risk of Depression • Minimal OSA: • • 1. 6 (1. 2 -2. 1) odds ratio for depression Mild OSA: 2. 0 (1. 4 -2. 9) odds ratio for depression Moderate or worse OSA: 2. 6 (1. 7 -3. 9) odds ratio for depression Peppard et al. Arch Intern Med. 2006; 166: 1709 -15

Mild Cognitive Impairment or Dementia • Prospective study of 194 women avg age 82. 3 yrs • Compared those with AHI>15/hr vs. <15/hr • Followed with cognitive evaluation for 4. 7 yrs • 44% developed MCI or dementia vs. 31% Yaffe K et al. JAMA 2011; 306: 613 -19
 odds ratio • •")
Risk of MCI or Dementia • Oxygen desaturation index (>15/hr) odds ratio • • • 1. 71 (1. 04 -2. 83) Percentage of sleep time in apnea >7% odds ratio 2. 04 (1. 10 -3. 78) Wake after sleep onset: no significant association Sleep duration: no significant association Yaffe K et al. JAMA 2011; 306: 613 -19

OSA reduces brain activation • Sustained attention task • f. MRI imaging • Precentral gyrus, insula, parietal lobe, cingulate gyrus, affected Ayalon et al. Sleep 2009; 32(3): 373 -81
: 373 -81")
Ayalon et al. Sleep 2009; 32(3): 373 -81

OSA Mortality Young T et al. SLEEP 2008; 31: 1071 -1078

Young T et al. SLEEP 2008; 31: 1071 -1078

OSA screening • Primary care health maintenance • Specialty – esp. Cardiology, Neurology • Pre-operative & Hospital admission • A simple to use screening tool has been developed
: 812 -821")
Chung F et al. Anesthesiology 2008; 108(5): 812 -821
: 812 -821")
Chung F et al. Anesthesiology 2008; 108(5): 812 -821
 • Weight loss • Treat")
OSA treatment options • Continuous positive airway pressure (CPAP) • Weight loss • Treat nasal airway congestion • Avoid supine sleep • Oral appliance • Surgical approaches have a limited role

Continuous Positive Airway Pressure CPAP devices: dependable, quiet. Heated humidity & improved interfaces have been major advances in this technology

Comfort Gel nasal mask

Latest CPAP advances • Use and performance • • tracking communication with health care system Remote setting adjustment

CPAP improves CVD markers • Severe OSA randomized to CPAP vs no Rx • After 4 months on CPAP: – Significant decrease in: • Carotid intima-media thickness • C-reactive protein • Catecholamines Luciano et al. Am J Respir Crit Care Med 2007; 176: 706 -12.

CPAP reduces CV risk • In mild to moderate OSA • Median follow-up of 6 yrs • Adjusted for other risk factors • Endpoints: MI, stroke, cardiac revasc, death • Event-free survival 51. 8 vs 80. 3%, on CPAP • # needed to treat to prevent one event over 10 years: 3. 5 Buchner et al. Am J Respir Crit Care Med 2007; 176: 1274 -80.

CPAP reduces CV risk in mildmod OSA Buchner et al. Am J Respir Crit Care Med 2007; 176: 1274 -80.
 and DMII •")
CPAP Treatment Effect on Glucose • 20 patients with OSA (AHI>15) and DMII • • • (Hgb. A 1 c: 7. 1) Continuous glucose monitoring during initial sleep study and after ~ 6 weeks of CPAP treatment Mean sleeping glucose decreased from 122 mg/dl to 102. 9 (p=0. 03) Hgb. A 1 c did not change Dawson, Abel, et al. J Clin Sleep Med v 4(6); 2008: 538 -542

CPAP Treatment effect on Cognition • 110 patients with mild-moderate OSA tested • • • before and after CPAP 3 months and compared to controls Verbal fluency and psychomotor function normalized with CPAP Mood improved Vigilance and working memory did not return to controls Jackson et al. J Clin Sleep Med vol 14(1); 2018: 47 -56

Health care utilization and OSA • In 10 years prior to dx of OSA: – ~Twice as many health care services • $3972/patient vs. $1969/patient • 6. 2 hosp days/patient vs. 3. 7 hosp day/patient • In 2 years after dx & rx of OSA: – Significant reduction in health care costs • 33% mean reduction in physician claims • Decrease hosp days: 1. 27 to 0. 54/pt/yr Ronald et al. Sleep 1999; 22: 225 -9. Bahammam et al. Sleep 1999; 22: 740 -7.

CPAP reduces hospital days Bahammam et al. Sleep 1999; 22: 740 -7.

Oral appliance

Treatment adherence rates • Antidepressants~65%* • Antihypertensives~50%** • Insulin~63%*** • CPAP~70% *Cramer et al. Psych Svcs. 1998; 49(2): 196 -201 **Vrijens et al. BMJ 2008; 336: 1114 ***Cramer Diabetes Care 2004; 27(5): 1218 -1224

Factors which improve CPAP adherence • Heated humidity • Good mask fit • Improvement in symptoms • Close followup

Conclusions • OSA is a relatively common, treatable • • • condition There is substantial evidence for OSA having a causal role in HTN & CAD In addition, OSA is a risk factor for stroke, cognitive impairment, obesity, depression, motor vehicle accidents, and death CPAP can reduce these risks
- Slides: 60