Obstetrics part 2 Gemma Adams Gabrielle Zealand What

Obstetrics part 2 Gemma Adams & Gabrielle Zealand

What we are going to cover Normal labour Premature & post-maturity Puerperium Complications – multiple pregnancy, abnormal fetal presentations, instrumental & operative delivery • Emergencies – prolapsed cord, shoulder dystocia, uterine rupture, pre-eclampsia • • The Peer Teaching Society is not liable for false or misleading information…

Normal labour • What is normal labour? – Spontaneous onset – Low-risk – Vertex position – Between 37 and 42 weeks – Good condition after birth – (without induction of labour, spinal/epidural/general anaesthesia, forceps/ventouse/ caesarean delivery or episiotomy) The Peer Teaching Society is not liable for false or misleading information…

Normal labour • General care in labour: • • • Low BP? Maternal positioning? Hydration/ eating? Pyrexia? Urinary tract? Psychological well-being The Peer Teaching Society is not liable for false or misleading information…

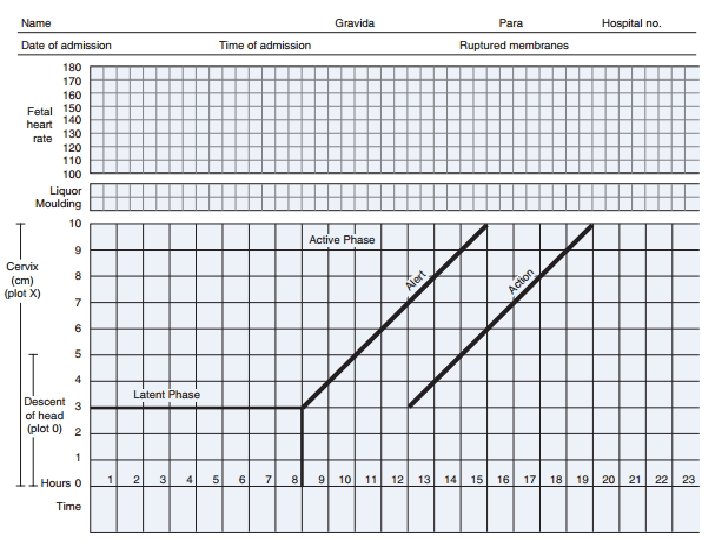
Normal labour • Phases of labour? – 1 st stage • Latent phase • Active phase • Transitional phase – 2 nd stage • From full cervical dilatation to birth – 3 rd stage • After the foetus is expelled until just after the placenta is expelled The Peer Teaching Society is not liable for false or misleading information…

Normal labour • • 3 Ps? Powers – – • Too little – nulliparous, amniotomy, oxytocin Too much – oxytocin, placental abruption, tocolytics Passage – Cephalopelvic disproportion, pelvic mass, cervical incompetence The Peer Teaching Society is not liable for false or misleading information…

Passenger/ fetal presentation Normal presentation? The Peer Teaching Society is not liable for false or misleading information…

Abnormal fetal presentation • Other abnormal presentations? The Peer Teaching Society is not liable for false or misleading information…

Abnormal fetal presentation • Risk factors? • Prematurity, multiple pregnancy, abnormalities of uterus, fetal abnormality, placenta praevia, smoking, polyhydramnios/oligohydramnios, IUGR, prev. breech • Breech • Confirm with USS • ECV • C-section The Peer Teaching Society is not liable for false or misleading information…

Mechanism of labour • • • Do frogs in Canada ride in a pink limo Descent Flexion Internal rotation Crowning Restitution Internal rotation of shoulders Anterior shoulder Posterior shoulder Lateral flexion The Peer Teaching Society is not liable for false or misleading information…

3 rd stage • Active/physiological • Active – uterotonic drugs, early clamping and cutting, controlled cord traction • Lower risk of PPH with active management • Retained placenta • Perineal trauma The Peer Teaching Society is not liable for false or misleading information…

Pain relief • Pain relief methods in labour? – Non-pharmacological – Entonox – Opioids – Pudendal nerve block – Epidural The Peer Teaching Society is not liable for false or misleading information…

Instrumental delivery • Most commonly due to prolonged second stage 1 hour of pushing has failed to deliver the baby • Maternal exhaustion • Fetal distress in 2 nd stage Level 1 Level 2 • Intermittent auscultation • Continuous CTG Level 3 • Fetal blood sampling The Peer Teaching Society is not liable for false or misleading information… Level 4 • Delivery by quickest route

Instrumental/ operative delivery The Peer Teaching Society is not liable for false or misleading information…

Contraindications to vaginal delivery • • • Multiple previous c-sections Vertical uterine scar Placenta praevia Severe antenatal fetal compromise Uncorrectable abnormal lie Gross pelvic deformity The Peer Teaching Society is not liable for false or misleading information…

C-section • • • IV fluids, consider crossmatch Ranitidine if elective section Catheterisation Lower uterine segment incision Abx prophylaxis Thromboembolism prophylaxis The Peer Teaching Society is not liable for false or misleading information…
 twins • Two or more ova")
Multiple pregnancy • Single fertilised egg divides (monozygotic) twins • Two or more ova fertilised (dizygotic) twins • In dizygotic each fetus has its own placenta, amnion & chorion • In monozygotic this depends on timing of division of ovum The Peer Teaching Society is not liable for false or misleading information…

Multiple pregnancy • Risk factors? • Previous multiple pregnancy, FH, assisted conception • Presentation? • Ultrasound, hyperemesis, enlarged uterus, polyhydramnios • Twin to twin transfusion syndrome • Monochorionic twins • Disproportionate bloody supply • Serial amniocentesis, laser therapy The Peer Teaching Society is not liable for false or misleading information…

Prematurity Born <37 weeks- 70% are spontaneous, 30% due to medical/obstetric disorder. Risk factors? - APH, multiple pregnancy, previous preterm, cervical weakness, smoking, genital infection (BV). Diagnosis - Persistent uterine activity and a change in cervical dilation and/or effacement. - Fetal fibronectin, cervical length scanning. The Peer Teaching Society is not liable for false or misleading information…

Prematurity Management Progesterone and antibiotics Tocolytic drugs- nifedipine and atosiban- can delay labour for up to 7 days - Allows time to give corticosteroids (increase surfactant) and make plans for post delivery. The Peer Teaching Society is not liable for false or misleading information…

Postmaturity & induction • Beyond 41 weeks, placental function may decline and become insufficient • Risk factors? • Previous post-term pregnancy, high maternal BMI, primigravidity • May be reduced fetal movements • Increased risk of meconium aspiration, neonatal hypoglycaemia, fetal macrosomia The Peer Teaching Society is not liable for false or misleading information…

Induction of labour • • CTG Bishop’s score Offer induction at 41 weeks Methods of induction? • Sweep of the membranes, prostaglandin gel/pessary, ARM ± oxytocin • Complications? • Uterine hyperstimulation, uterine rupture, infection, prolapsed cord, amniotic fluid embolism The Peer Teaching Society is not liable for false or misleading information…

Puerperium • 6 week period following giving birth • Lochia • Problems? • • Perineal pain Urinary & bowel problems Mastitis ± infection Endometritis Psychiatric PPH – primary/secondary Thromboembolism Contraception The Peer Teaching Society is not liable for false or misleading information…

Obstetric emergencies • • Uterine rupture Eclamptic seizure Haemorrhage Cord prolapse Sepsis DIC Amniotic fluid embolism • • Fetal distress Uterine inversion Shoulder dystocia PE Placental abruption Adrenal haemorrhage HELLP syndrome The Peer Teaching Society is not liable for false or misleading information…

Cord Prolapse The Peer Teaching Society is not liable for false or misleading information…

Cord Prolapse Risk Factors? 2 nd twin, breech, polyhydramnios, unengaged head, abnormal lie, artificial amniotomy, low lying placenta. If in the Overt presentation there is intermittent cord compression and fetal asphyxia. Signs? Cord seen at vaginal entrance on examination Fetal bradycardia and variable decelerations. The Peer Teaching Society is not liable for false or misleading information…

Cord Prolapse Management • If occult or funic haven’t corrected- C section. • In Overt- Stop the presenting part pressing on the cord with manual upward pressure. • Patient in the knee-chest position. • If cord outside of the body keep warm and moist • Give Tocolytics- to delay contractions. • Proceed to Surgery The Peer Teaching Society is not liable for false or misleading information…

Shoulder dystocia Inability to deliver the shoulders after delivery of the head, after the shoulder becomes stuck behind the pubic symphysis Risk factors? - Previous shoulder dystocia, maternal diabetes, fetal macrosomnia, BMI >30, induction of labour, prolonged early labour, assisted vaginal delivery. The Peer Teaching Society is not liable for false or misleading information…

Shoulder dystocia Complications Fetal • Brachial plexus injury- Erb’s palsy. • Hypoxia- cord compression, reduced ability for chest expansion. • Fractured clavicle. Maternal • Post partum haemorrhage • 3 rd and 4 th degree perineal tears The Peer Teaching Society is not liable for false or misleading information…

Shoulder dystocia Management • Stop the mother pushing • Mc. Roberts position with suprapubic pressure and gentle downward traction • Episiotomy • Internal manoeuvres • Symphisiotomy • Zavanelli manoeuvre – firm pressure on fetal head to reverse and allow C section The Peer Teaching Society is not liable for false or misleading information…

Uterine Rupture Risk factors? - Previous C sections, scarred uterus, uterine abnormalities, oxytocin use. Presentation? - Constant pain and tenderness over uterus, small amount of vaginal bleeding, maternal tachycardia and signs of shock, cessation of contractions, fetal hypoxia. Management - Stabilise mother with IV fluids and cross match bloods. - Delivery via C Section. The Peer Teaching Society is not liable for false or misleading information…

Preeclampsia Pregnancy induced hypertension in association with proteinuria with/without oedema Risk factors? - 1 st pregnancy, previous preeclampsia, over 40, BMI >35, FH, underlying HTN, renal disease, diabetes. Presentation? - BP >140/90 in 2 nd half of pregnancy with proteinuria Severe frontal headache, sudden swelling (hand , feet , face), visual disturbance, fetal distress, liver tenderness and deranged LFTs, epigastric pain, papilloedema. Eclamptic Seizure- occurs in less than 1%, Grand Mal seizure, risk of fetal hypoxia and maternal death. The Peer Teaching Society is not liable for false or misleading information…
 Fluid balance Delivery")
Preeclampsia Management - Conservative monitoring Anti HTN Magnesium sulphate (seizure prevention) Fluid balance Delivery Eclampsia Management - Resuscitation Magnesium sulphate Anti HTN Fluid therapy Delivery The Peer Teaching Society is not liable for false or misleading information…

Preeclampsia Complications? - HELLP- haemolysis, elevated liver enzymes, low platelet count. DIC Renal Failure ARDS The Peer Teaching Society is not liable for false or misleading information…

Any questions? The Peer Teaching Society is not liable for false or misleading information…
- Slides: 36