OBSTETRIC ANESTHESIA In the Rural Setting and Whats

+ OBSTETRIC ANESTHESIA In the Rural Setting. . . and What’s New in Obstetric Anesthesia

+ Sarah Bergakker CRNA, MSN “Director” of Obstetric Anesthesia Spectrum Health Gerber Memorial sabergak@gmail. com

+ My Morning Traffic Jam n (The traffic isn’t the only thing that is different when practicing as a CRNA in the rural setting)

+ CASE STUDY n n CRNA on call notified in the evening Adolescent G 1 P 0, 34 wks gestation female to ER by ambulance n To Radiology for trauma scans n Returns to OR for uncontrolled bleeding in abdomen and pelvis n Massive transfusion n Run over and dragged by motor vehicle n Obstetrician and General Surgeon achieve hemostasis n From ER to OR for Emergency C-section n Transported intubated by helicopter to tertiary care center n Mother becomes hemodynamically unstable in PACU

+ Why do small hospitals even provide obstetric care? “Currently, approximately 34% of hospitals providing obstetric care have fewer than 500 deliveries per year” ACOG Comm Opinion No. 344

+ Why do small hospitals even provide obstetric care? “When geographic factors require the existence of smaller units, these units should be part of a well-established regional perinatal system” ACOG Comm Opinion No. 344

+ Critical Access vs. Community Hospital Critical Access n 25 or less licensed inpatient beds n Located 35 miles drive from any hospital (or 15 miles in rugged terrain) n “Be located in a rural area or an area treated as rural” n Community Hospital n No restriction on number of licensed inpatient beds n Located in any community, anywhere Average inpatient LOS 96 hrs (4 days) or less n No restriction on LOS n Provide 24 hr ER service n Bills medicare at regular rate n Can bill Medicare patients at 101% n Cannot be located in: Connecticut, Delaware, Maryland, New Jersey, Rhode Island

+ Critical Access Hospitals Nationwide

+ Nursing Education Loan Repayment Program http: //goo. gl/Dm. TJdf

+ Nursing Education Loan Repayment Program n “The Nursing Education Loan Repayment Program will pay 60 percent of the participant’s total qualifying loan balance in two years and an additional 25 percent of the original balance for an optional third year. In order to qualify, NURSE Corps members must fulfill a service obligation at any one of the thousands of nonprofit hospitals, clinics and other facilities located in designated primary medical care or mental health Professional Shortage Areas across the U. S. ”
 Chart graphic")
+ Who’s Doing What Where (Does not have to be an anesthesiologist) Chart graphic source: http: //goo. gl/no 92 Pb

+ Who’s Doing What Where

+ The American Congress of Obstetricians and Gynecologists (and why they get to suggest how to do our job) n n ACOG issues opinions that are used nationally as guidelines for obstetric care Because safe delivery of the baby, or resuscitation of the mother may require anesthesia care, CRNA practice guidelines are influenced by ACOG n Examples n n ACOG committee opinion http: //goo. gl/EUjwlj VBAC http: //goo. gl/j 35 HNq There should be “availability of anesthesia and surgical personnel to permit the start of a cesarean delivery within 30 minutes of the decision to perform the procedure” VBAC guidelines “Women and their physicians may still make a plan for a TOLAC in situations where there may not be “immediately available” staff to handle emergencies, but it requires a thorough discussion of the local health care system, the available resources, and the potential for incremental risk”

+ !! IMMEDIATELY AVAILABLE !! “The Definition of immediately available personnel and facilities remains a local decision based on each institution’s available resources and geographic location. ”

+ Obstetric Hemorrhage and Massive Transfusion
 n Goal")
+ Obstetric Hemorrhage and Massive Transfusion CALIFORNIA MATERNAL QUALITY CARE COLLABORATIVE (CMQCC) n Goal is to standardize monitoring for and care of the hemorrhaging obstetric patient n Identify patients at increased risk for obstetric hemorrhage n QUANTIFY BLOOD LOSS via standardized system n Stage 1 of hemorrhage protocol activated at > 500 ml blood loss for vaginal delivery and > 1000 ml blood loss for cesarean delivery n includes ordering Type and Cross of 2 units PRBCs) n Includes calling for additional help
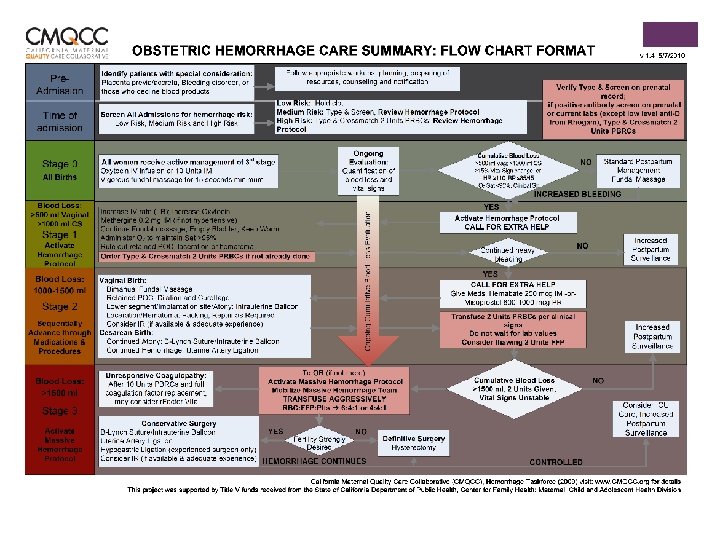

Obstetric Hemorrhage and Massive + Transfusion Specific Management Challenges for the Rural Setting n EARLY recognition of hemorrhage and well coordinated response critical due to limited resources n Limited practitioners available for “extra hands” response n n n Know who and what your resources are Limited blood products available n Most rural hospitals will not have platelets available in house n Some will not have cryoprecipitate Structure should be in place for smooth transfer to tertiary care center when indicated

+ Cardiac Arrest in Pregnancy n Extremely low frequency, extremely high acuity event n Rate of 1: 12, 000 of hospitalizations for delivery n n Lower rate of occurrence in institutions with < 1000 deliveries/yr. Common causes: hemorrhage, heart failure, amniotic fluid embolism, and sepsis

+ Reasons to Prepare for Cardiac Arrest in Pregnancy n n n Cause can be directly anesthesia related and reversible: Local anesthetic toxicity, high spinal, failed intubation, aspiration n Hard to achieve goal of incision in 4 minutes and delivery in 5 without prior practice simulations n Facility factors associated with 75% of fatal outcomes n Difficult to successfully resuscitate mother until baby is delivered n Annual drills foster teamwork between involved departments Double the mortality for failed response/resuscitation Preparation and drills will help identify overall ability of obstetric and anesthesia departments to respond to emergencies in various locations
")
+ Cardiac Arrest in Pregnancy What’s Different? n Perform manual left uterine displacement (LUD) n Remove internal and external fetal monitoring equipment n Prep the abdomen n For third trimester patients place hands higher on sternum (2 -3 cm higher) n If patient receiving magnesium stop infusion and give calcium IV n Defibrillation guidelines the same and safe for fetus What’s Different? n IV access above diaphragm n At 4 minutes post arrest proceed to emergent ON LOCATION C-section if no return of spontaneous circulation (ROSC) n Goal is delivery of baby within 5 minutes of cardiac arrest of mother in absence of ROSC n DO NOT move patient to the OR n Time is lost n Compressions and management interrupted n Remove LUD after delivery

+ The Difficult Airway and Obstetrics Any obstetric unit can quickly become “rural” in the sense of location in the hospital and immediately available resources n Induction of general anesthesia in the obstetric population will result in failed intubation via direct laryngoscopy 1: 300 n Induction of general anesthesia may be necessary for: n Emergent c section n Failed spinal or epidural n Prolonged duration of operative procedure

+ The Difficult Airway and Obstetrics n Should always have a full airway setup ready to go in the obstetric OR n n n n 6. 5 ETT and stylet n Various sizes of ETT Syringe for ETT cuff inflation Two working handles n One short n One long Miller 2 and Mac 3 blade LMAs Suction Oral airways (avoid Nasal airways)

+ The Difficult Airway and Obstetrics The cost of obstetric unit dedicated airway devices is minimal when compared to adverse outcomes associated with lack of immediately available resources

The Difficult Airway and Obstetrics IF UNABLE TO INTUBATE OR VENTILATE DO NOT PROCEED TO CSECTION DELIVERY!!!! Copyright © 2014 International Anesthesia Research Society. Published by Lippincott Williams & Wilkins. 25

+ The Difficult Airway and Obstetrics STOP THINK COOMUNICATE • ASSESS PATIENT, SITUATION STATUS, AND RESOURCES • THINK ABOUT WHAT YOU PLAN TO DO NEXT • TELL THE TEAM WHAT YOU PLAN TO DO NEXT

+ CASE STUDY n 24 yr. old G 1 P 0 in active labor n CRNA called in on a weekend evening shift for urgent C section for failure to progress n n Pt medical hx: 2 siblings have died from “genetic cardiomyopathy” n Sibling one at age 2 n Sibling two at age 6 First female of affected cousins to have pregnancy n Refused all maternal cardiac testing n Refused all fetal cardiac testing n Refused MFM workup n Patient has cardiac Mets > 4 activity tolerance n In labor and cannot be transferred n How would you proceed ? ? ?
 and why you should care to know about it Provides")
+ TRANSTHORACIC ECHO (TTE) and why you should care to know about it Provides a noninvasive, real-time method of assessment superior to physical assessment alone. TTE is not intended to replace transesophageal echocardiography. The purpose is provide an immediately available, rapid assessment tool in the perioperative setting.
 VIDEO Video 1: 18 4: 04 6: 16 https: //www.")
+ TRANSTHORACIC ECHO (TTE) VIDEO Video 1: 18 4: 04 6: 16 https: //www. youtube. com/watch? v=Gcj. Fy. RPl. ISw

+ TRANSTHORACIC ECHO n Increased image quality and decreased cost of ultrasound technology making TTE more and more available n “Goal Directed Therapy” n n n Addresses the “I wish I had an ECHO” problem n Anesthesia is late to the party that ER and ICU started Minimal technical training required for successful technique n Non-invasive method to assess hemodynamic status Can be used any time during the perioperative period to aid decision making n “Pocket Ultrasound will likely replace your stethoscope” Dr. J. T. Sullivan n Qualitative assessment of valve disorder severity Assessment for intra operative cardiovascular collapse Rapid assessment in PACU of new onset hemodynamic instability

+ Other Applications of Ultrasound in Obstetric Practice Identification of landmarks when placing epidural in patients with a high BMI ( Video ) 2: 25, 3: 10, 3: 36 https: //www. youtube. com/watch? v=M 4 hi. P 46 YMuc

+ Other Applications of Ultrasound in Obstetric Practice n n Pulmonary ultrasound n Pulmonary edema n Pneumothorax n Pulmonary Effusion Trans-ocular ultrasound n Assess intracranial pressure n Placement of cricothyrotomy n Assessment of airway anatomy Image Credit
")
+ “Call the Midwife” (and get the nitrous)
")
+ “Call the Midwife” (and get the nitrous)
 n Used as early as 1881")
+ “Call the Midwife” (and get the nitrous) n Used as early as 1881 in Poland for labor analgesia n United Kingdom 60% use n In 1934 self administration method increases use n Australia 50% n 1 % or less of U. S. births currently using n Finland Canada about 50% n *Data for home birth rates in these countries would be of interest n *Data for midwife delivery rates also of interest n Two major centers n University of California, San Francisco (> 30 yr. hx) n Vanderbilt University Medical Center n Entonox® in Europe n Nitronox® in United States

+ N 2 O use in the labor suite is out there and happening!
 “CONS” n Epidural decreases VAPS by")
+ “Call the Midwife” (and get the nitrous) “CONS” n Epidural decreases VAPS by 5 pts or to around 3/10 “PROS” n Not significantly higher rate of N&V n Less sedating than Remifentanyl infusion n Not as effective as Remifentanyl infusion for analgesic effects n Patients “like” it and would use it again – less invasive n What is scavenging system? n Little/no negative neonatal effect n Does not change uterine contractility n Anti anxiety effects n Patient can still ambulate n Can be administered by nursing personnel n Do not need continuous pulse oximetry – “minimal sedation” n Repeated staff exposure n Maternal hypoxemia n Studies do not show effective at decreasing pain during labor n May require CRNA resources to manage
 n Take Away: If Nitrous Oxide")
+ “Call the Midwife” (and get the nitrous) n Take Away: If Nitrous Oxide implementation occurs at your facility the anesthesia department does not need to necessarily manage daily setup and administration in labor and delivery. However, the anesthesia department should be a key player in the development of policies and procedures surrounding use and implementation in labor and delivery.

+ References: n Department of Health and Human Services critical access hospital PDF http: //goo. gl/Sxd 8 rt n CMS. gov Centers for Medicare & Medicaid Services Critical Access Hosptials http: //goo. gl/o. Ug. QFv n Nursing Education Loan Repayment Program http: //goo. gl/Dm. TJdf n CMS Manuel System Pub 100 -07 State Operations Provider Certification http: //goo. gl/no 92 Pb n Critical Access Hospitals map and Statistics http: //goo. gl/l. Kd. ZQf n ACOG committee opinion Optimal Goals for Anesthesia Care in Obstetrics http: //goo. gl/EUjwlj n ACOG Today Aug 2010 New VBAC Guidelines http: //goo. gl/j 35 HNq n California Maternal Quality Care Collaborative http: //goo. gl/Sc. C 9 Tf n ASA Opinion Nitrous oxide for Labor http: //goo. gl/sek. MMM n Nitrous Ocide for Labor Analgesia: Expanding Analgesic Options for Women in the United States M. R. Collins et al. Reviews in Obstetrics & Gynecology Vol. 5, No. ¾, 2012

+ References: n Limited transthroacic echocardiography assessment in anaesthesia and critical care. J. G. Faris et al. Best Practice and Research Clinical Anaesthesiology 23 (2009) 285 -298 n Obstetric Hemorrhage Care Guidelines: Flow Chart Format http: //goo. gl/Fues. BT n California Maternal Quality Care Collaborative https: //cmqcc. org/ob_hemorrhage n The Society for Obstetric Anesthesia and Perinatology Consensus Statemetn on the Management of Cardiac Arrest in Pregnancy. S. Lipman et al. Anesthesia and Analgesia. May 2014, Volume 118, number 5. n Cardiac Arrest during Hospitalization for Delivery in the United States, 1998 -2011. J. M. Mhyre et al. Anesthesiology. 120: 810 -8. n The Unanticipated Difficult Intubation in Obstetrics. J. M. Mhyre and D. Healy. Anesthesia and Analgesia. March 2011. Volume 112. Number 3.
- Slides: 40