Obsessive Compulsive Disorder and OC Spectrum Disorders J

Obsessive Compulsive Disorder and OC Spectrum Disorders J. Hancey, MD Dept. of Psychiatry Oregon Health Sciences University

The many faces of OCD • Dermatologist: Chapped hands, eczema, Trichotillomania • Oncologist/Infectious disease: Hypochondriasis (Cancer, AIDS) • Neurologist: OCD associated with Tourette’s or other neurologic disorders • Obstetrician: OCD during pregnancy or postpartum • Pediatrician: Compulsive behavior, OCD secondary to Sydenham’s chorea, difficulty in school • Plastic surgeon: Body dysmorphic disorder • Dentist: Gum lesions from excessive teeth bleeding • Family practitioner: Report of family member washing or checking excessively, comorbid affective or anxiety disorders, all of the above.

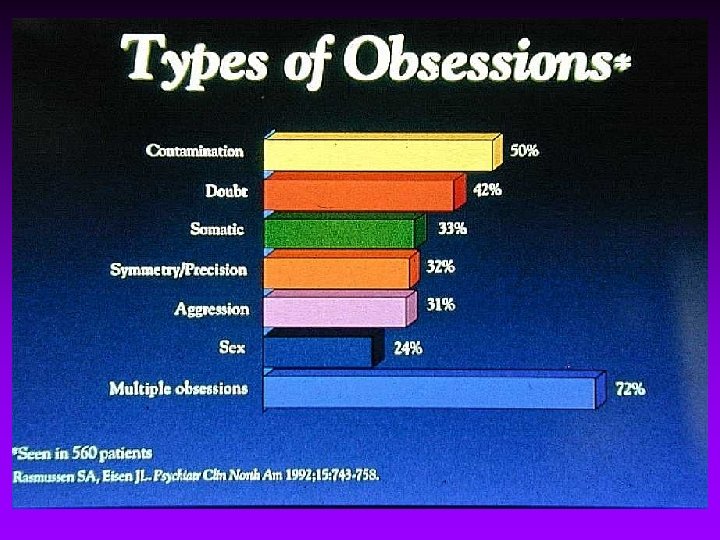
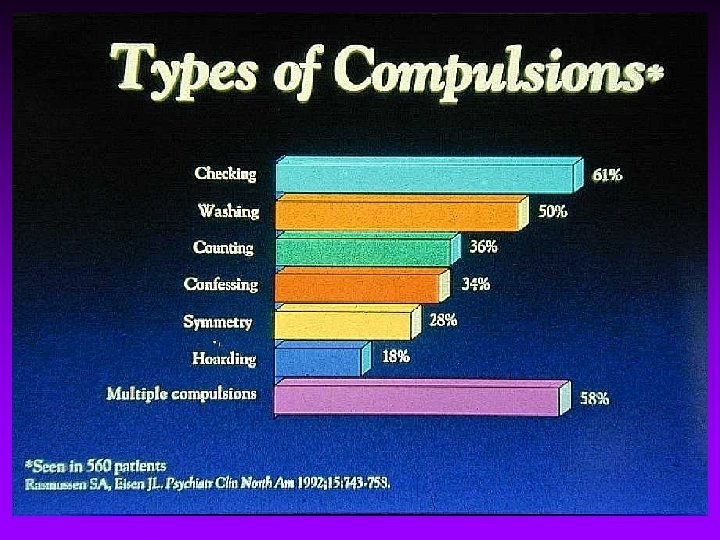
Definitions of OCD An anxiety disorder characterized by: Obsessions Recurrent and persistent ideas, impulses, thoughts, images that are intrusive and sometimes senseless Compulsions Repetitive, seemingly purposeful behaviors performed in response to an obsession (e. g. , ritualistic or stereotypic behavior) Anxiety arises around resistance to obsessions and/or compulsions Anxiety may or may not be the primary feature of OCD

Diagnostic Criteria for OCD • Either obsessions or compulsions • Recognized by patients as excessive or unreasonable • Obsessions or compulsions cause marked distress, are time consuming, or significantly interfere with functioning DSM-IVtm 1994: 417 -423

Obsessive-Compulsive Spectrum Disorders Preoccupations with bodily sensations or appearance Body Dysmorphic Disorder Depersonalization Anorexia nervosa Hypochondriasis OCD Impulsive disorders Sexual compulsions Trichotillomania Pathological gambling Kleptomania Self-injurious behavior Hollander et al, J Clin Psychiatry, 1966 Tourette’s syndrome Sydenham’s chorea Torticollis Neurologic Autism disorders ADHD

Epidemiology of OCD • 6 -month point prevalence: 1. 6% • Life-time prevalence: 2. 5% • An estimated 3. 9 million Americans had OCD in 1990 • 4 th most common psychiatric disorder • Double that of panic disorder or schizophrenia

Biological Differences of OCD • Anatomy • decreased caudate nucleus volume • Biochemistry • increased CSF 5 -HIAA • Physiology • increased frontal and pre-orbital glucose utilization

Precipitating Factors • 25%--depression and/or anxiety accompanied the initial symptoms • 50% - 60%--stressors around the time of onset of symptoms --pregnancy --childbirth --sexual problems --death in family • Streptococcal pharyngitis

The Streptococcal Connection • Increasing evidence for an autoimmune etiology • Group A beta hemolytic streptococcus • Antineuronal antibodies • Genetic vulnerability D 8/17 positivity as a marker

PANDAS • • • Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections

Treatment • Medications • Cognitive Behavioral Therapy

COGNITIVE THERAPY

Cognitive Therapy • • Re-label Re-attribute Re-focus Re-evaluate Schwartz, J. Brain Lock Pearl: Use a “mental garbage can”.

BEHAVIOR THERAPY

Behavior Therapy Effective behavior therapy involves • Exposure: facing feared or avoided object, thought, situation, or place, preferably in vivo • Response or ritual prevention: delaying and diminishing anxiety-reducing compulsions
 • • • List compulsive behaviors Assign SUD’s")
SUD’S List: (Subjective Units of Distress) • • • List compulsive behaviors Assign SUD’s value to each (0 -100) Rank order from top to bottom Begin at the bottom of the list Best source: Baer, Lee. Getting Control. Pearl: Break up complex rituals into various parts

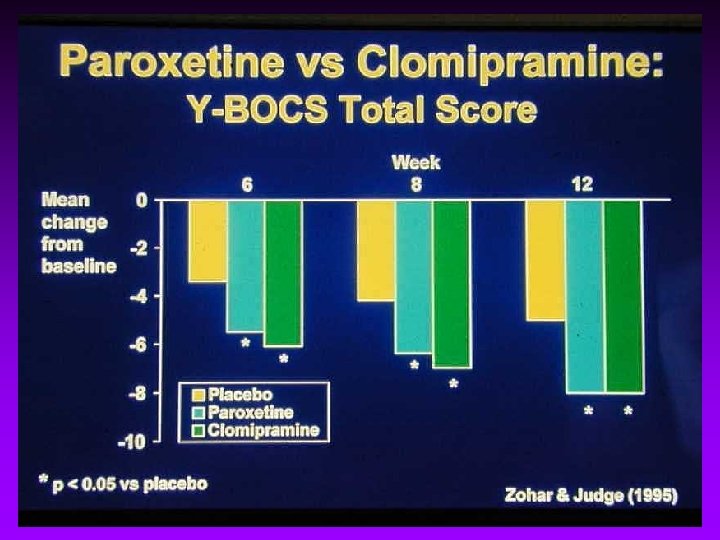
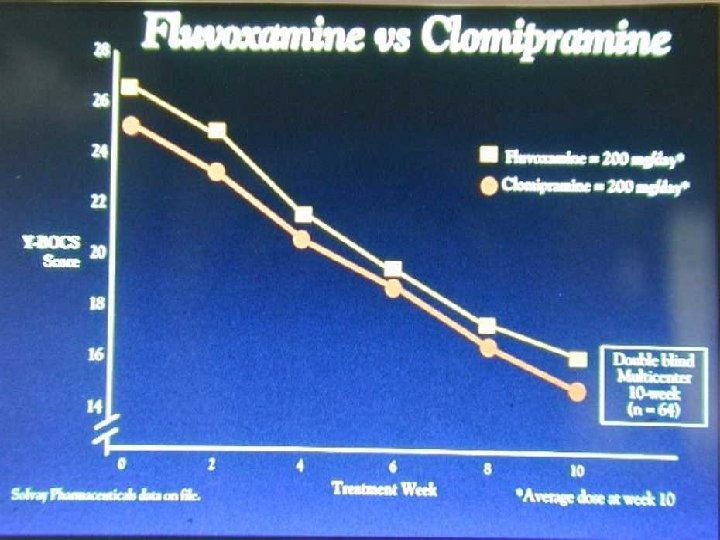
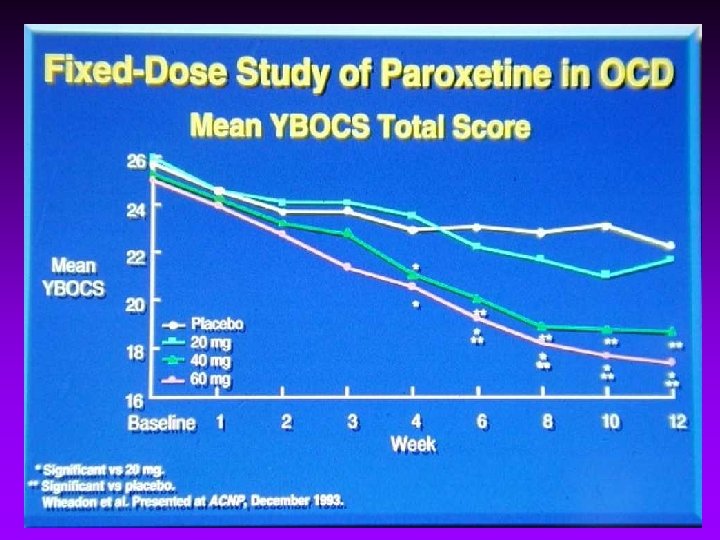
Serotonin Reuptake Inhibitors in the Treatment of Obsessive Compulsive Disorder
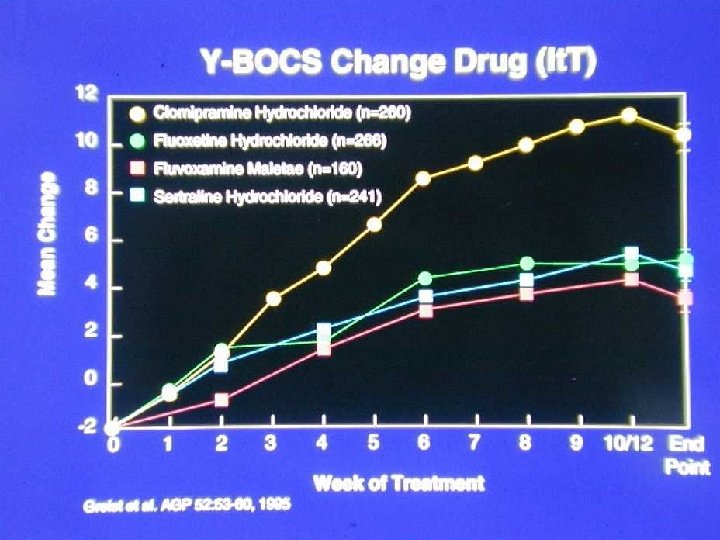

Fluoxetine vs Clomipramine • 20 week crossover • No difference between Y~BOCS • Delayed response to 2 nd drug • Relapse occurred during washout • <ADR with fluoxetine ADR = adverse drug reaction Pigott et al. Arch Gen Psychiatry, 1990; 47: 926 -932.

Factors Affecting Serum Drug Levels • • Absorption Protein binding Metabolism Elimination

Utilizing P 450 Inhibition 1 A 2 CMI 2 D 6 Desmethyl CMI inactive

The Role of Anxiolytics When, What, and When to Worry • Initial stages of treatment, prn • BZD’s - the long and short of it • abuse, dependence and addiction

Benzodiazepine Issues • Abuse • Physical dependence • Addiction

Treatment Strategies • SSRI beginning at low doses, gradually increasing to maximum doses • minimum 10 week trial • switch SSRIs • augmentation – – clonazepam atypicals opioid agonism/antagonism acamprosate • cognitive-behavioral therapy • surgery
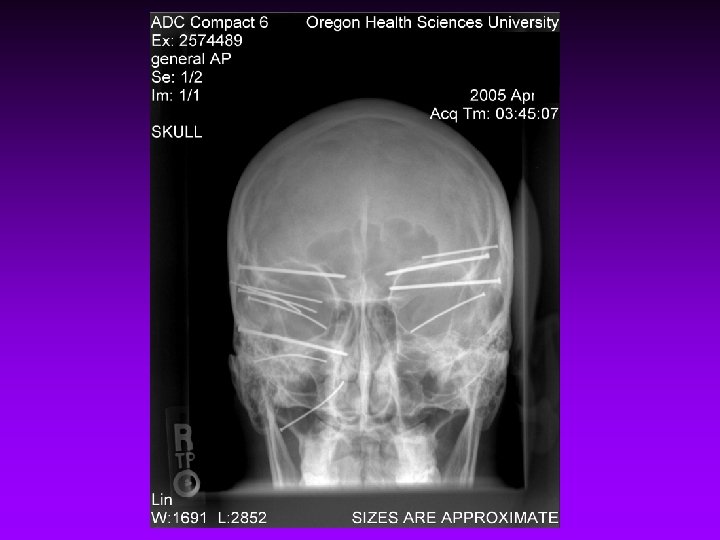

Gamma Knife
- Slides: 33