Observation of the Ear Must inspect their size
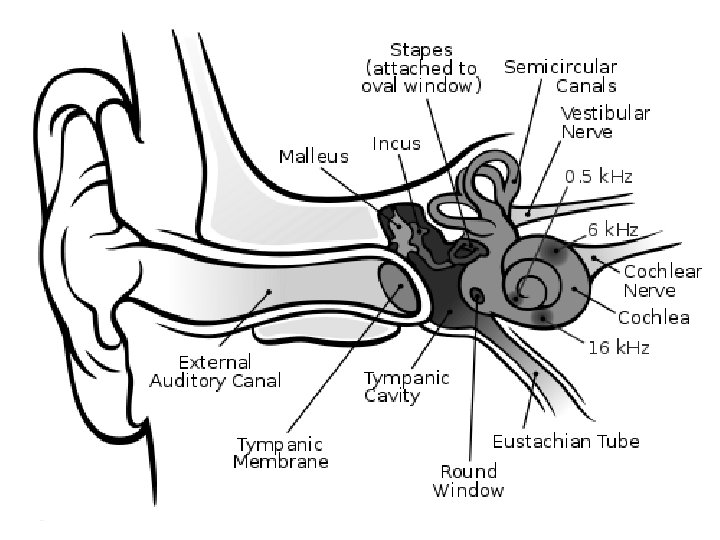

Observation of the Ear • Must inspect their size and shape, position, and the presence of skin tags, dimples, or other anomalies. • Otoscopic examination – Note the presence of cerumen, discharge, inflammation, or a foreign body in the ear canal. • Visualize the tympanic membrane. – Observe its color, landmarks, and light reflex, as well as presence of perforation, scars, bulging, or retraction.

Otoscopic Examination of Ear • Note presence of cerumen, discharge, inflammation or foreign body in ear canal • Visualize tympanic membrane for color, landmarks, and light reflex. Also for abnormalities like perforation, bulging, scars or retraction

Otitis Externa Inflammation or irritation of the outer ear and ear canal • Signs and symptoms – Itching – Pain, accentuated when pinna or targus are moved and when chewing – Feeling of pressure or fullness (may be either conductive or sensorineural) – Occasional hearing loss – Rare otorrhea, defined as inflammation with purulent discharge – Erythema and edema of ear canal – Cerumen may become whitish – Absence of fever

• Diagnosis Otitis Externa – Examination of ear – Occurrence of presenting symptoms, including positive history – On otoscopy, ear canal appears swollen and debris may be present – A culture may be done for bacteria or fungus when otitis externa does not appear to be improving • Nursing care – Manage pain through analgesics and warm compresses to affected ear – Treat infection – Antibiotic or antifungal eardrops may be prescribed • Education/discharge instructions – Educate family on strategies to prevent reinfection – Educate on proper dose and method of administration of eardrops

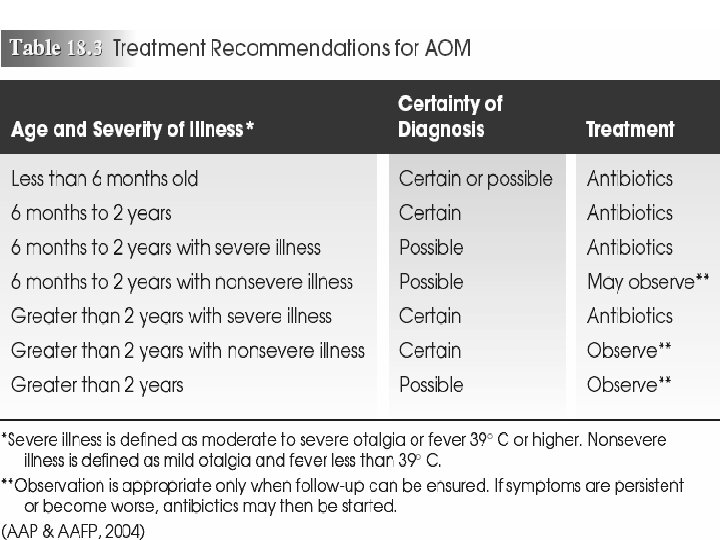
Otitis Media • Suppurative infection of the middle ear cavity – Pathophysiology : Bacterial or viral infection of fluid in middle ear – Peak incidence: 0 -2 years, especially 6 -12 months – Therapeutic management • Acute otitis media (AOM) – Nursing assessment • Health history • Physical examination and diagnostic testing
")
Otitis Media Signs and symptoms • Acute otitis media: – Otalgia (acute ear pain) – Irritability – Otorrhea – Fever, which may be as high as 104ºF (40ºC) – Poor feeding – Rubbing or pulling at the affected ear – Bulging tympanic membrane, air-fluid level, or visualization of purulent material on otoscopic examination – Postauricular and cervical lymph glands and lymph node enlargement
 • Otitis media with effusion (OME), or chronic")
Otitis Media Signs and symptoms (cont’d) • Otitis media with effusion (OME), or chronic otitis media: – Often asymmetrical and afebrile – Intermittent complaints of ear pain – Feeling of fullness in the ear, popping or a feeling of “talking in a barrel” – Complaint of hearing loss – Dizziness or impaired balance – Chronic vomiting and failure to thrive may be related to chronic OME

Otitis Media Diagnosis • Based on signs and symptoms and otoscopic examination • In acute otitis media (AOM), the intact membrane appears bright red and bulging, with no visible landmarks or light reflex • In OME, otoscopic examination reveals slightly injected dull gray membrane, obscured landmarks, and visible fluid level or meniscus behind the eardrum if air is present

Prevention of Hearing Loss • Treatment and management of recurrent otitis media – A common cause of conductive/middle-ear hearing loss – Medical tx: • Wait and see • Antibiotics Acute Otitis Media – note erythema and opacity of tympanic membrane
 (cont’d) – Nursing management • Control fever")
Otitis Media • Acute otitis media (AOM) (cont’d) – Nursing management • Control fever and pain with either acetaminophen or ibuprofen • Heat or cool compress: have child lay affected ear on compress • Warm compresses to affected ear • Narcotic analgesics like codeine for severe pain • Numbing eardrops like benzocaine (Auralgan) • Treat infection with antibiotic (amoxicllin) or antifungal eardrops • Surgical insertion of pressure-equalizing tubes remains a common treatment for persistent OME
 • Educating the family – Observe for S&S and call PCP")
Otitis Media (cont’d) • Educating the family – Observe for S&S and call PCP – Follow-up to check progress, test hearing – If antibiotics are prescribed, the full course of medication must be administered – Tell parents that if the child doesn’t respond to antibiotics within 48 to 72 hours, another assessment must be done to confirm acute otitis media and exclude other causes of illness or ineffective antibiotic response

• • • Preventing AOM Encourage breastfeeding 6 -12 months Avoid exposing child to individuals with upper respiratory infections DON’T EXPOSE TO SECOND HAND SMOKE Immunize child, including flu vaccines Xylitol, a sucrose substitute, taken in liquid or gum form, may prevent AOM

Prevention of Hearing Loss • Surgical treatment – Tympanostomy: placement of ear tubes – for children less than about 5 -6 years old, allow bathing, hair washing, surface swimming, or ocean exposure. . . without any precautions. – Diving deeper under water, or swimming in (dirtier) lakes and rivers is more likely to cause infections. – In those cases, the preventitive use of certain antibiotic ear drops (such as Floxin Otic) may help. Your ear doctor may be adamant about keeping your infant's ears dry. . . ENT docs like to see their tube patients every 3 -6 months, or until the ears are normal. – Adenoidectomy, with just myringotomies (making an incision, no tubes) may be appropriate in certain children. . . as might a laser myringotomy. • Prenatal preventive measures • Avoid exposure to noise pollution
 – Presence of fluid in middle ear")
• Otitis media with effusion (OME) – Presence of fluid in middle ear space without S&S of infection – Nursing assessment • Health history Otitis Media – Risk Factors: passive smoking, not breastfed, frequent upper respiratory infections, allergy, young age, male, congenital disorders • Physical examination – May be asymptomatic or experience popping or fullness behind eardrum – Otoscopic exam may reveal dull, opaque tympanic membrane that’s gray, white or bluish. Tympanometry may diagnose OME – Nursing management • Educating the family – Antihistamines, antibiotics and steroids usually don’t work – Teach NOT to prop infant with bottle • Monitoring for hearing loss and speech development • Providing postoperative care for the child with pressureequalizing tubes – Tubes inserted and remain a few months – May need to avoid water in ears, wear earplugs with baths and swimming
 • Small tubes(made of plastic, metal, or Teflon) • Surgically placed")
Myringotomy (Ear Tubes) • Small tubes(made of plastic, metal, or Teflon) • Surgically placed into child's eardrum by an ear, nose, and throat surgeon • Help drain fluid out of the middle ear in order to reduce the risk of infections • About one million children each year have tubes placed in their ears. • The most common ages are from 1 to 3 years old. • By the age of 5 years, most children have wider and longer eustachian tubes

Myringotomy – Pre and Post-Op Nursing Care * • Prepare child and parent for surgery: Assessment, VS • The operation usually takes 15 to 20 minutes. • Child will go home 2 -4 hours after surgery. • Post-Op Care and Teaching – Normal to have fluid 3 -4 days, grey/brown and slight smell Fluid may leak from your child’s ear – The tubes will stay in your child’s ears for several months – Do not put anything into your child’s ear – May have a bath. Ear plugs may or may not be recommended by surgeon. Consult surgeon about other water activities like swimming. • Medicines – Antibiotic ear drops: may or may not order antibiotic ear drops. Show parent how to put the antibiotic ear drops in child’s ear. – Pain medicine: Acetaminophen or Ibuprofen May return to day care or school the day after leaving the hospital, if your child is feeling well. First visit is normally 7 -10 days after surgery, then every 2 -4 months

Myringotomy – Pre and Post-Op Nursing Care * REASONS TO CALL SURGEON • Ears leak fluid for more than 4 days after the operation. • Your child has a fever over 38. 5°C (101°F). • Your child’s ears start to leak fluid again after they have stopped leaking, or the color of the drainage changes to thick greenish pus with a strong smell. • Your child’s ears become sore
 • Infection and inflammation of external ear canal • Bacterial")
Otitis Externa (Swimmer’s ear) • Infection and inflammation of external ear canal • Bacterial or fungal • Nursing assessment – Health history – Physical examination • Ear red, edematous, itchy, painful, may affect hearing • Nursing management – Managing pain – Treating the infection – Preventing reinfection – Recent studies recommend leaving ear wax in place as protection.

Types of Delayed-Onset Hearing Loss • Conductive hearing loss – Results when transmission of sound through the middle ear is disrupted, as in the case of OME • Sensorineural hearing loss – Caused by damage to the hair cells in the cochlea or along the auditory pathway • Mixed hearing loss – Occurs when the cause may be attributed to both conductive and sensorineural problem

Hearing Loss and Deafness • Nursing assessment – Health history – Physical examination and laboratory and diagnostic tests • Nursing management – Augmenting hearing – Promoting communication and education – Encouraging education – Providing support

Hearing Impairment • Ranges from mild to profound • Deaf: a person whose hearing disability precludes processing linguistic information with or without hearing aid • Hard of hearing: generally able to hear with hearing aid

Incidence in Children • One of the most common disabilities • Estimated 3 in 1000 well babies have some degree of hearing loss • Neonates in ICU: 2 -4 per 100 • In US about 1 million children from birth to 21 years have hearing loss – 1/3 of these children have other sensory or cognitive problems

Causes of Hearing Impairments • • • Anatomic malformation Low birth weight Ototoxic drugs Chronic ear infections Perinatal asphyxia Perinatal infections: – rubella, herpes, syphilis, bacterial meningitis • Cerebral palsy
 or")
Levels of Hearing Loss • Hearing loss may be unilateral (involving one ear) or bilateral (involving both ears) • Extent of hearing loss is defined based on the softest intensity of sound that is perceived, described in decibels (d. B) – 0 to 20 d. B: normal – 20 to 40 d. B: mild loss – 40 to 60 d. B: moderate loss – 60 to 80 d. B: severe loss – Greater than 80 d. B: profound loss
 – A unit of loudness –")
Symptom Severity • Measured in decibels (d. B) – A unit of loudness – Measured at various frequencies – Speech range is 2000 cycles/sec • Hearing threshold – Measurement of a person’s hearing threshold with audiometer – Degree of symptom severity as it affects speech

• • Pathology of Hearing Impairments Conductive hearing loss—middle ear Sensorineural hearing loss—nerve deafness Mixed conductive-Sensorineural loss—may follow recurrent otitis media with complications Central auditory interception: – Organic: defect involves reception of auditory stimuli along central pathways and expression of message (aphasia) – Functional: no organic lesion exists to explain central auditory loss (conversion hysteria, infantile autism, childhood schizophrenia)

Manifestations of Hearing Impairment in Infancy • • • Lack of startle reflex Absence of babbling by age 7 months General indifference to sound Lack of response to spoken word EARLY DETECTION, best within 3 -6 months, essential to improve language and educational outcomes

• Medical Therapeutic Management of Hearing Impairment – Antibiotic therapy for otitis media • Surgical interventions – Tympanostomy tubes for chronic otitis media • Hearing aid – – – Learn how to use hearing aid Teach child to manage when old enough Managing acoustic feedback • Reinsert aid • Check for hair • Clean ear mold or ear • Lower volume • Cochlear implants: May help children with sensorineural hearing loss

• The diagnosis of a significant disability can be extremely stressful for the family. • Encourage families to express their feelings and provide emotional support • The child with hearing loss should receive early intervention with hearing aids or other augmentative devices to minimize the psychosocial impact of sensory deficits.

Childhood Deafness • Profound deafness likely to be diagnosed in infancy • Entry into school • Concerns with speech development – One reason number of words and speech assessed at PCP’s visit

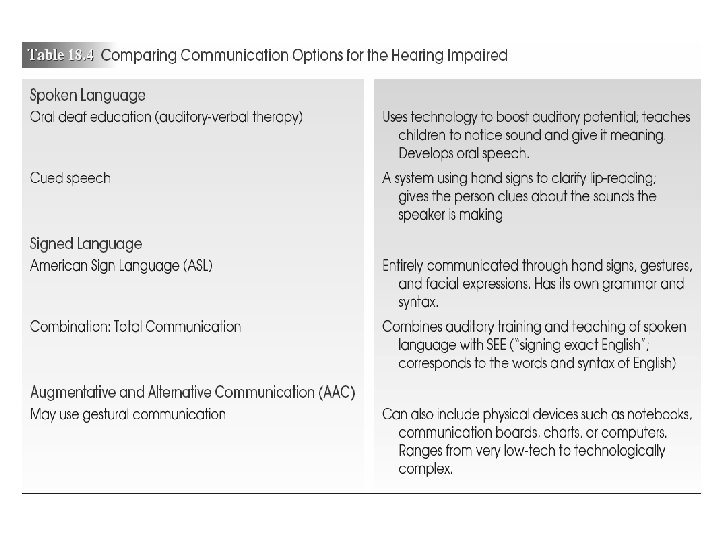
• • Promoting Communication Lipreading Cued speech Sign language Speech language therapy Socialization Additional aids Cochlear implant – A cochlear implant is a small, complex electronic device that can help to provide a sense of sound to a person who is profoundly deaf or severely hard-of-hearing. The implant consists of an external portion that sits behind the ear and a second portion that is surgically placed under the skin

Care for Hearing Impaired Child During Hospitalization • Reassess understanding of instructions given • Supplement with visual and tactile media • Communication devices: – Picture board – Common words and needs (food, water, toilet) – Sign language (need an interpreter) – Computer

Deaf-Blind Children • • • Profound effects on development Motor milestones usually achieved Other development often delayed Finger spelling Developing future goals for the child
- Slides: 36