Objectives Discuss differences between pediatric and adult sepsis

Objectives �Discuss differences between pediatric and adult sepsis �Discuss the three stages of sepsis �Review symptoms and causes of sepsis in both pediatric and adult patients populations

Sepsis �System updates �Dr. Cichon video

Definition �The word sepsis comes from the Greek meaning “decay” or “to putrefy” �Defined as the “the presence of pathogenic organisms or their toxins in the blood and tissues. ” �Physicians draw from a list of signs and symptoms to make the diagnosis

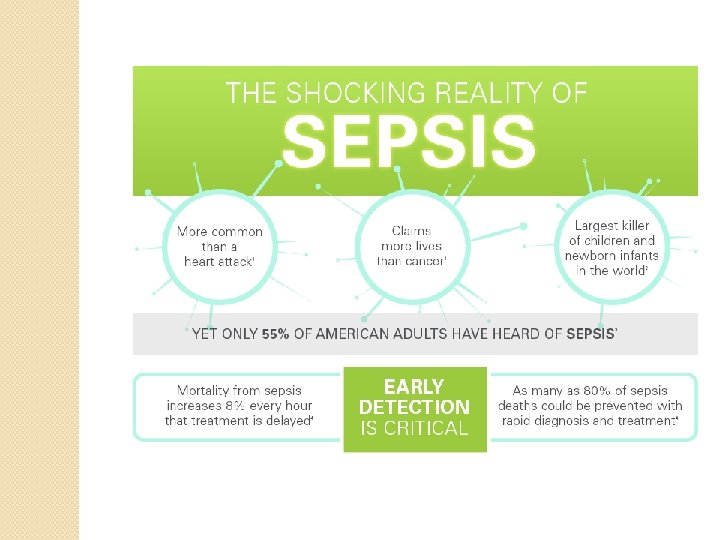
Sepsis �Kills 258, 000 Americans each year �Named as the most expensive inpatient cost in American Hospitals (24 billion) � 40% of patients diagnosed with severe sepsis do not survive �Listed as one of top ten diseases leading to mortality in the United States

Causes �Aging population ◦ Americans living longer ◦ Highest risk group people older than 65 �Drug resistant bacteria ◦ Root cause of the infections that trigger sepsis �Weakened Immune Systems ◦ More Americans living with weakened immune systems caused by HIV, Cancer treatments or transplant drugs

Risk Factors �Sepsis is more common and more dangerous if you: �Are very young or very old �Have a compromised immune system �Are already ill, often in an ICU �Have wounds or injuries, such as burns �Have invasive devices

Prevention �Get vaccinated: against the flu, pneumonia, and any other infections that could lead to sepsis �Prevent Infections: cleaning of wounds and scrapes and practicing good hygiene �Time matters: If you have an infection look for the signs of sepsis

Differential Diagnosis �Syndromes ◦ ◦ ◦ ◦ that mimic sepsis include Hypovolemia Acute blood loss Pulmonary embolus Acute myocardial infarction Acute pancreatitis Diabetic ketoacidosis Adrenal insufficiency

Sepsis

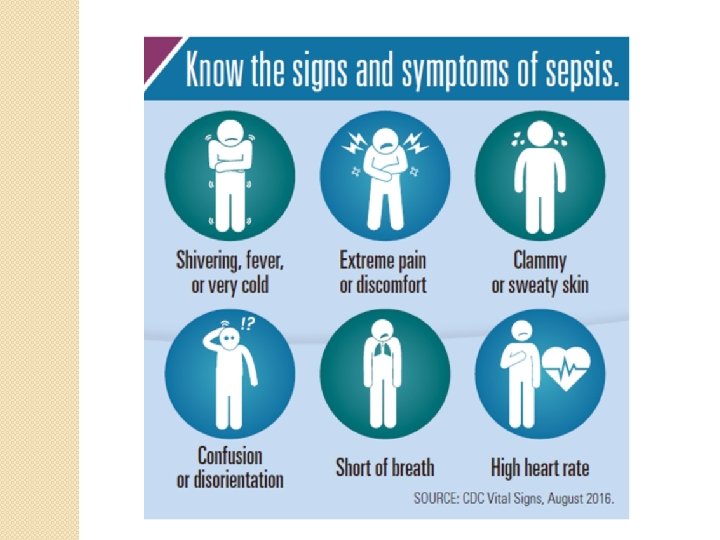
SIRS �Clinical response to a non specific insult of either infectious or noninfectious origin �SIRS is defined as two or more of the following ◦ Fever of more than >100. 4 or less than <96. 8 ◦ Heart rate of > 90 bpm ◦ Respiratory rate of >20

SIRS �Non specific and may be caused by: �Ischemia �Inflammation �Trauma �Infection �Or several of these combined �SIRS is not always related to infection

Sepsis �Life threatening condition that arises when the body’s response to infection injures its own tissues and organs �Sepsis is caused by an immune response triggered by an infection �Most common cause is bacterial �May also be caused by fungi, viruses or parasites

Sepsis �Defined as severe when the finding occur in association with signs of ◦ ◦ ◦ Organ dysfunction Hypoxemia Oliguria Lactic acidosis Elevated liver enzymes Altered cerebral function

Sepsis �Common locations for the primary infection include: �Lungs �Brain �Urinary Tract �Skin �Abdominal Organs

Sepsis �In the very young, old and people with weakened immune systems there may be no symptoms of a specific infection and the body temperature may be low or normal rather than high. �Sepsis is a medical emergency

Sepsis �Vulnerability to sepsis is becoming more widespread due to �More opportunities for infections to become complicated due to: ◦ More people having invasive procedures and transplants and taking immunosuppressive drugs and chemotherapies ◦ Rising antibiotic resistance-microbes becoming immune to drugs that would otherwise control infections

Sepsis ◦ Is the patient’s presentation suggestive of any of the following infections? �Pneumonia (cough/thick sputum) �Urinary Tract Infection �Acute AMS/ change in mental status �Indwelling Catheter related �Abdominal pain or diarrhea �Wound Infection �Skin/Soft Tissue infection

Severe Sepsis �Indications if you exhibit one or more of the following signs and symptoms which indicate an organ may be failing ◦ ◦ ◦ Significantly decreased urine output Abrupt change in mental status Difficulty breathing Abnormal heart function Abdominal pain

Septic shock �Primary cause is bacteria �Fungi and viruses may also be a cause �Release of toxins from the bacteria and fungi cause tissue damage, hypotension and poor organ function �Researchers believe septic shock causes the formation of tiny clots that block nutrients and oxygen from reaching the vital organs

Septic Shock � Primary symptoms include: ◦ ◦ ◦ Skin discoloration or rash Tachycardia Confusion Lethargy Chills Shortness of breath

Septic Shock �People ◦ ◦ ◦ ◦ ◦ at higher risk include: Lymphoma Leukemia Immune system diseases Diabetes HIV Recent infection or surgery Bone marrow and solid organ transplant Recent use of steroid medication Long term antibiotic use

Jim Henson �Began to feel flu like symptoms on Saturday �Was admitted to the hospital on Tuesday with trouble breathing diagnosed with sepsis �Developed septic shock caused by Group A streptococcus (multiple abscesses in lungs) �Died on Wednesday May 16, 1990 at age 53
 � Mother Theresa (infected pacemaker) �")
Sepsis and Celebrities � Casey Kasem (infected wound) � Mother Theresa (infected pacemaker) � Christian Brando (pneumonia) � Robin Gibb (cardiac complications from sepsis) � Corey Haim (pneumonia) � Bernie Mac (pneumonia) � George Michael (pneumonia) � Prince Ranier of Monaco (pneumonia) � Leslie Nielson (pneumonia) � Wayne Rogers (pneumonia) � Pope John Paul II (UTI)

Scenario � You are called to the local high school for the 17 year old student not feeling well. Upon arrival you are taken to the school nurse’s office where you find him lying on a cot with his left foot elevated on a pillow. � You begin your assessment and the student tells you he cut his foot at practice a few days ago and now his foot is red, tender, hot to touch and hurts when he tries to walk. � He also tells you he feels warm and weak and tired.

Scenario �S- hurts when he walks, warm, red and hot �A- none �M- Albuterol inhaler �P-cut to the bottom of foot �L- toast and juice �E- pain increased with ambulation and feeling weak

Scenario �Vital Signs �Pulse - 100 �BP – 98/54 �RR -26 �Skim warm, flushed , dry �You examine the foot and note yellow purulent drainage from the wound on the bottom of the foot

Scenario �Does this patient have 2 or more Systemic Inflammatory Response criteria? �If yes, what criteria �Is there an actual or potential infection? �If so what is the source? �Treatment?
 �Sepsis ◦ ◦")
Early Recognition in Pre Hospital Setting (Loyola/Edward EMS Systems: Adult Patients) �Sepsis ◦ ◦ ◦ Criteria for EMS (3 or more) Suspected infection Respiratory Rate >20 Breaths per minute Heart rate > 90 Beats per minute Systolic Blood pressure <90 mm Hg Documented Fever or history of temp >100. 9 or <96. 8 ◦ New onset mental status change ◦ O 2 saturation LESS than 90%
 �If Sepsis field")
Early Recognition in Pre Hospital Setting (Loyola/Edward EMS Systems: Adult Patients) �If Sepsis field criteria are present, proceed: � 1. Administer oxygen to titrate pulse oximetry to a saturation >92%. � 2. If there is no concern of fluid overload, and lungs are clear, initiate a 0. 9 NS 500 m. L fluid bolus. � 3. If there is concern of fluid overload, and the patient is a normotensive, initiate fluid of 0. 9 NS at 20 m. L/hr. � Notify ECRN of Sepsis criteria during communication and immediately upon arrival in the emergency department.

Capnography and Sepsis �Clinical indicator of metabolic distress is lactate monitoring �Quantitative waveform capnography reliable for lactate monitoring in detecting metabolic distress in sepsis patients �Lactate levels rise when organ hypo perfusion occurs �Patient becomes lactic acidotic

Capnography and Sepsis �Body’s response is to increase respiratory rate to account for the acidosis �As lactate rises, carbon dioxide levels fall �ETCO 2 levels accurate predictor of mortality in patients with severe sepsis or septic shock

Capnography �Severe sepsis is characterized by poor perfusion leading to build up of serum lactate and resulting in metabolic acidosis �This results in lower Et. CO 2 levels �Increased respiratory rate “blows off” CO 2 and lowers Et. CO 2


Pediatric Sepsis �Leading cause of illness and death among U. S. children and worldwide �>42, 000 cases annually increasing by 13% per year � 4 th leading cause behind asthma, appendicitis, and poisonings � 7 -9% of all childhood deaths are due to sepsis more common than cancer

Pediatric Sepsis �EMS is likely encountering septic pediatric patients more often than we recognize �Challenge due to the low frequency of pediatric patients encountered �Severity of septic shock is often masked in infants and children due to strong compensatory mechanisms

Pediatric Sepsis �Recognize ◦ ◦ signs of poor perfusion Decrease in mental status Cold extremities Delayed capillary refill Weak pulses, different central and peripheral pulses ◦ Low urine output ◦ Hypotension or low BP

Pediatric Sepsis �Progression in children from simply ill to severely sick to organ failure can happen rapidly �Initial presentation is often non specific especially in younger patients. �Subtle changes in vital signs can be difficult to recognize �Use reference devices for age appropriate vital sign ranges

CHART Mnemonic �C- Complaint �H- History �A- Assessment �R- Red Flags �T- Treatment �Common initial pediatric complaints that should cause an EMS provider to think sepsis include infections of the ear, respiratory or urinary tract)

Pediatric Sepsis �Complaints in pediatric patients that classically point to infection include ◦ ◦ ◦ Runny nose (yellow/green drainage) Fever Rash Vomiting/diarrhea, Discharge or pus Concentrated foul smelling urine

Pediatric Sepsis �Small patients may not be old enough to complain of anything �They may only experience vague non specific complaints such as ◦ Extreme sleepiness ◦ Lethargy or irritability ◦ May have no history or obvious signs of infection
 is considered to be an integral part")
Pediatric Sepsis �The Pediatric Assessment Triangle (PAT) is considered to be an integral part of the general assessment of a sick child. It is used by PALS, APLS, Pediatric Education for Prehospital Professionals (PEPP), and the Emergency Nursing Pediatric Course (ENPC). Apr 17, 2016

Pediatric Assessment Triangle
 �Bone marrow transplant �Central or")
High Risk Patients �Malignancy �Asplenia (including sickle cell disease) �Bone marrow transplant �Central or indwelling line/catheter �Solid organ transplant �Severe Mental Retardation/ Cerebral Palsy �Immunodeficiency, immunocompromised or immunosuppressed

Assessment Criteria �Consider sepsis or septic shock if child has suspected or proven infection and at least two of the following ◦ Altered mental Status �Extreme or unexplained irritability, delirium, lethargy or floppiness �AVPU = V, P, or U �GCS <11 or recent change >3
 �Body temperature: ◦ < 97 degrees F or >101 degrees F")
Assessment Criteria (cont’d) �Body temperature: ◦ < 97 degrees F or >101 degrees F (< 36 degrees C or >38. 5 degrees C) �Tachycardia: Use reference guide for age appropriate range �Tachypnea: Use reference guide for age appropriate range �Serum glucose: >180 mg/d. L

RED Flags �Skin pale, ashen cyanotic or mottled or has a non blanching rash �Prolonged capillary refill of >5 seconds �Supplemental oxygen, required to maintain Sp. O 2 > 92% �Et. CO 2 <32 mm. Hg �Respiratory: severe respiratory distress, tachycardia, bradycardia, grunting or apnea

Red Flags �Heart Rate: High for age range �Systolic Blood pressure: Hypotensive for age range ◦ <1 month: <60 mm. Hg ◦ 1 month to 10 years: <70 +(2 x age in years) mm. Hg ◦ Older than 10 years: <90 mm Hg �Urine output <1 m. L/kg (dry diapers) �Serum glucose <120 mg/d. L or >180 mg/d. L

Septic Shock �Cold Shock �Pulses central and peripheral weak �Capillary refill> 3 sec �Skin mottled and cool �Mental status altered �Warm Shock �Pulses central and peripheral are bounding �Capillary refill <1 sec �Skin is flushed, ruddy erythroderma �Mental status decreased, irritability, crying or

PALS Guidelines �Recognize altered mental status and perfusion q. Give oxygen q. Support ventilation q. Establish vascular access q. Fluid at 20 cc/kg repeat as needed. Reassess after each bolus q. Blood glucose

What Should EMS DO? �Airway: May require advanced airway �Breathing: Supportive oxygen ( consider BVM to reduce or eliminate the work of breathing) �Circulation: Rapid vascular access via IV or IO. ◦ Fluid administration 20 m. L/kg boluses of normal saline �Hyperglycemia is more common finding but check for hypoglycemia and treat age appropriate

Scenario �You are called for the 4 year old who has been feeling ill for 5 days with fever of 102. 0. �Child was seen in the ER last night and sent home with Tylenol. Diagnosed with a virus �Child is crying stating his stomach hurts. �Has not been eating or drinking today and minimal intake last several days
 �Pediatric Assessment Triangle ◦ Appearance= Lethargic ◦ Work of breathing = Rapid")
Scenario (cont’d) �Pediatric Assessment Triangle ◦ Appearance= Lethargic ◦ Work of breathing = Rapid and Shallow ◦ Circulation to skin =Pale �Sick or not Sick?

Scenario �Vital ◦ ◦ ◦ Signs Heart rate = 150/min RR= 30/min Temp = 102. 4 F Blood pressure= 80/ 46 Pulse oximetry = 92% �Lungs clear �Abdomen slightly rigid, tenderness in right lower quadrant �Not oriented to person, place

Scenario �Dry mucous membranes �Skin cool and dry �Capillary refill >3 seconds �Sick or not sick? �Treatment

Scenario �Once in the ambulance the child is placed on the monitor and oxygen. �IV was unsuccessful �You begin transport and the child becomes more lethargic and repeat vital signs are now: ◦ ◦ ◦ BP 70/P HR: 170 RR 40 Cap refill >5 secs What are your next steps in caring for this child?

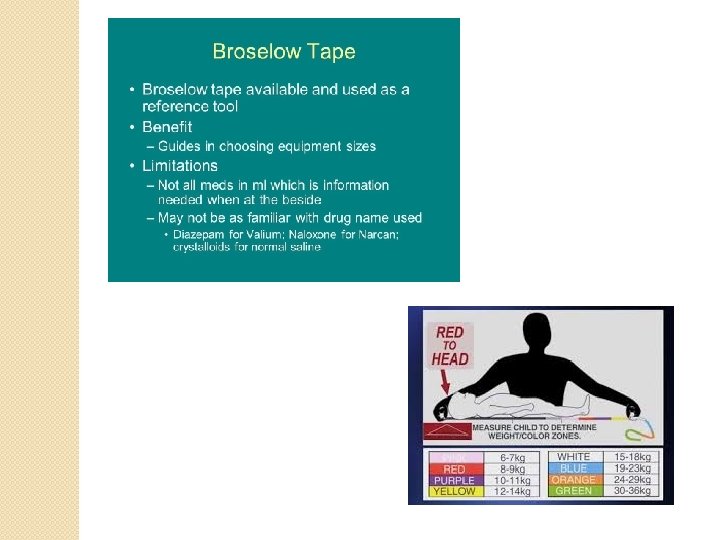
Broselow Tape �Visual system for mediation doses and equipment selection �Based on relationship between weight and length across all ages �To use effectively have child lying down �Hold red end of tape at child’s head �Run tape down length of body until even with his/her heels �Medications are best dosed by actual body weight

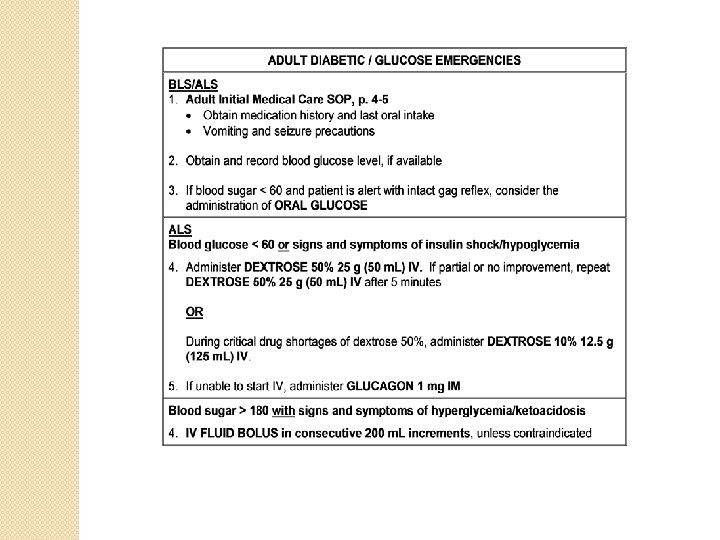
Dextrose 10% �Option due to frequent shortages of Dextrose 50% �Many diabetics have poor vasculature and dextrose 10% is better for the veins, easier to infuse (less osmotic) �The half life of D 50 varies averaging about 30 minutes �D 50 administration can result in rapid and prolonged hyperglycemia

Dextrose 10% �Rapid elevation of serum glucose may exacerbate chronic issues in the diabetic �Hyperglycemia acute and long term has been associated with deleterious side effects in ◦ ◦ Stroke Head injury Post resuscitation outcomes Sepsis

Dextrose 10% �Dextrose ◦ ◦ 10% reduces risks of Vessel injury Tissue damage from extravasation Glucose fluctuations are less significant Minimizes the risk of secondary rebound hypoglycemia

Administration Procedure

Administration Procedure

Administration Procedure

Administration Procedure

Pediatric Dosing Chart

Anyone Can Develop Sepsis

- Slides: 73