OBJECTIVES Definition Extent Boundaries Structures passing through the

OBJECTIVES � Definition � Extent � Boundaries � Structures passing through the canal � Protecting mechanism � Applied aspects

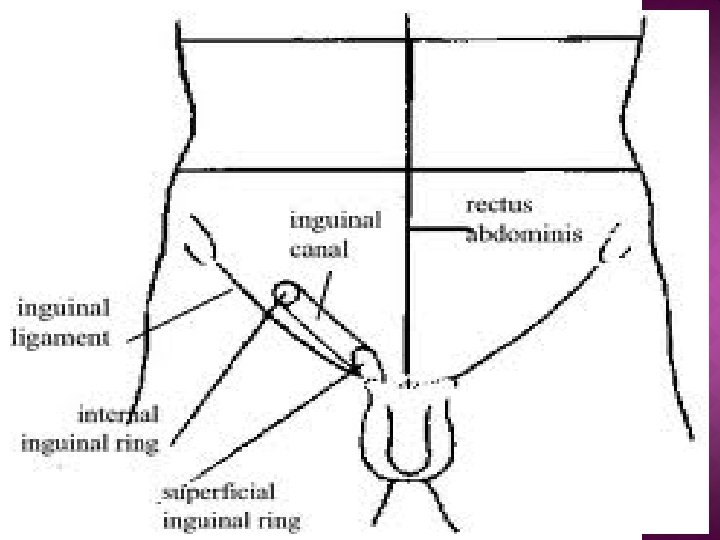
� Oblique passage in the lower part of the anterior abdominal wall, situated just above the inguinal ligament.

LENGTH – About 4 cm EXTENSION – Deep inguinal ring to Superficial inguinal ring Deep inguinal ring Superficial inguinal ring

PECULIARITIES � In females canal is narrow � In newborns the canal is directed almost straight

� Hiatus in the external oblique aponeurosis. � Triangular in shape. � Base is the crest of the pubis. � Sides are the margins of the opening in the aponeurosis(crura). � The lateral crus is stronger

� The medial crus is thin, flat band attached to the front of the pubis and interlacing with the opposite crus. � Intercrural fibres -Some of the fibres of investing fascia of external obliqe, arch above the apex of superficial inguinal ring as intercrural fibres.

� Situated in transversalis fascia, � about 1. 25 cm above the mid inguinal point, lateral to the stem of inferior epigastric artery.

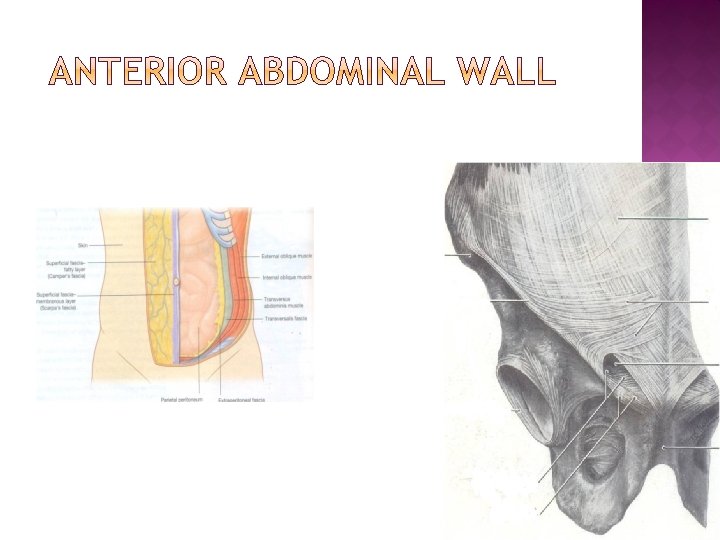
BOUNDARIES OF INGUINAL CANAL. ANTERIOR WALL IN ITS WHOLE EXTENT • Skin • Superficial fascia • External oblique aponeurosis IN LATERRAL ONETHIRD • Fibres of internal oblique

BOUNDARIES OF INGUINAL CANAL POSTERIOR WALL ENTIRELY FORMED BY • Fascia transversalis MEDIAL-HALF • Conjoint tendon MEDIAL ONE -FOURTH • Reflected part of inguinal ligament

roof Arched fibers of the internal oblique and transversus abdominis muscle. Transversus abdominis Internal oblique Floor Grooved upper surface of the inguinal ligament, Medial end: upper surface of the lacunar ligament. Grooved surface
Spermatic cord in males; round ligament of the uterus in females. 2)Ilio-inguinal nerve in")
1)Spermatic cord in males; round ligament of the uterus in females. 2)Ilio-inguinal nerve in both sexes

INGUINAL HESSELBACH. INGUINAL TRIANGLEOFOF HESSELBACH. Peritoneal triangle in the posterior wall of the inguinal canal. BOUNDARIES Lateral – Inferior epigastric artery. Medial – Lateral border of rectus abdominis. Inferior – Inguinal ligament.
 Obliquity of the canal Deep and superficial rings")
DEFENSIVE MECHANISM OF INGUINAL CANAL 1) Obliquity of the canal Deep and superficial rings are at different planes 2) Guarding-mechanism Opposite to the deep ring : anterior wall is strengthened by fleshy fibers of the internal oblique muscle. Opposite to the superficial ring: posterior wall by conjoint tendon and reflected part of inguinal ligament. 3) Slit-valve mechanism Due to approximation of the two crura of the superficial inguinal ring.
 Flap-valve The posterior wall of the canal is pushed forwards and comes in")
4) Flap-valve The posterior wall of the canal is pushed forwards and comes in contact with the anterior wall , obliterating the canal like a flap valve.
 Shutter mechanism Arched fibers of internal oblique and transversus act as demi-sphincters. In")
5) Shutter mechanism Arched fibers of internal oblique and transversus act as demi-sphincters. In increased intra abdominal pressure, it obliterate the canal by bringing the roof in contact with the floor.
 Ball-valve action In increased intra-abdominal pressure, cremaster muscle contracts and pulls the testis")
6) Ball-valve action In increased intra-abdominal pressure, cremaster muscle contracts and pulls the testis towards the superficial ring.

An abnormal protrusion of a viscus or a part of a viscus through a weak point (opening) in the walls of its containing cavity.

ETIOLOGY OF HERNIA Increase in intra abdominal pressure due to: Straining Persistent cough Smoking

INGUINAL HERNIA INDIRECT

INDIREC T DIRECT
 Bubunocele B) Funicular C) Complete")
INDIRECT INGUINAL A) Bubunocele B) Funicular C) Complete

� Herniotomy � Herniorraphy � Hernioplasty Ø Open method Ø Laparoscopic method
- Slides: 26