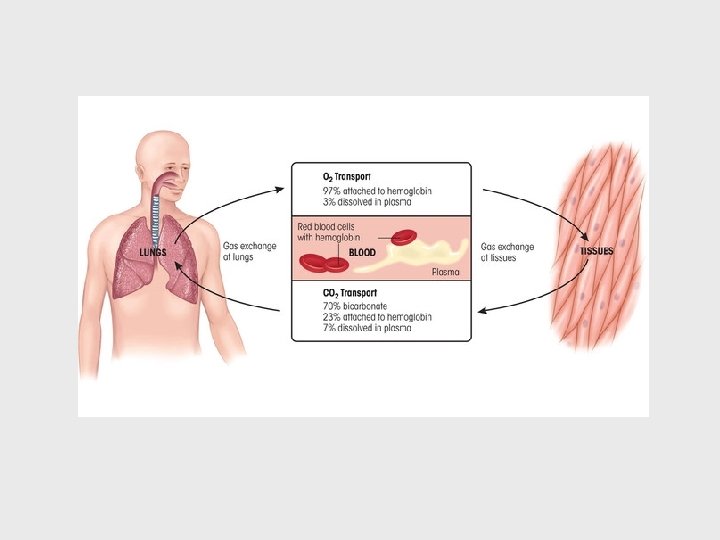
Objective 4 Erythrocytes A Functions Carry O 2

Objective 4 Erythrocytes A. Functions Carry O 2, CO 2 B. Normal Values (At sea level) adult males: 4. 7 – 6. 1 X 106/ l blood adult females 4. 2 – 5. 4 X 106/ l blood that’s about 83 billion/in 3 Why do men have a higher concentration of RBCs than women? ? testosterone enhances RBC production estrogen suppresses RBC production

C. Structure: diameter averages: 7. 5 m biconcave discs organelles: none; are anucleate RBCs have a limited lifespan (120 days) and generate ATP anaerobically

Important Proteins in RBCs: Hemoglobin: Spectrin: Enzymes: carries CO 2 and O 2 maintains the biconcave shape but allows for change in shape (reversible deformity) antioxidant enzymes, glycolytic enzymes (Why? ) and carbonic anhydrase
 The")
Erythrocytes are shaped like biconcave discs (maintained by cytoskeletal elements including spectrin, ankyrin) The flattened biconcave shape provides maximum surface area for the diffusion of gases into and out of the cell

Spectrin Ankyrin What do you predict happens to the shape of RBCs when people have defective or absent spectrin or ankyrin? They assume a more rounded shape and are called spherocytes

Normal Blood Smear Spherocytosis

Splenomegly is one consequence of hereditary spherocytosis. Can you think of any other consequences? Pay attention through the rest of the topic and see if you can spot other potential consequences !

What erythrocyte characteristics enhance the gas transporting ability of an erythrocyte? • small size, lots of surface area (biconcave shape) • presence of hemoglobin • anaerobic metabolism (they do not consume the O 2 that they carry)

Objective 5 Hemoglobin A. Functions 1. Carries up to 4 molecules of O 2 lungs HHb + n. O 2 reduced hemoglobin Hb(O 2)n + H tissues oxyhemoglobin (deoxyhemoglobin) 2. Carries up to 2 molecules of CO 2: tissues HHb + n. CO 2 Hb(CO 2) n lungs carbaminohemoglobin
, a vasodilator 4. Buffers H+ Hb has a much")
3. Carries NO (nitric oxide), a vasodilator 4. Buffers H+ Hb has a much greater affinity (200 X) for carbon monoxide (CO) than O 2. Why is CO so toxic? Hb + CO carboxyhemoglobin (bright purple)

B. Normal Values: Adult males: 13 -18 g/100 ml blood Adult females 12 -16 g/100 ml blood Infants 14 -20 g/100 ml blood C. Location Found only within erythrocytes Why is it advantageous for hemoglobin to reside in RBC’s ? ? 1. Prevents degradation and leakage into tissues and urine 2. Prevents it from contributing to viscosity and osmotic pressure Remember hemoglobin is a protein !
 each globin")
Structure of Hemoglobin Globin: 4 polypeptide chains (2 , 2 non ) each globin chain binds covalently to a heme globin binds to CO 2

Heme porphyrin ring with a central Fe 2+ there are four hemes/hemoglobin each heme binds to one O 2

Hemoglobin Heme Let’s complete the workbook chart by examining this figure.

# globin chains/molecule 4 # Fe 2+/heme 1 # chains/molecule 2 # O 2 carried by one Fe 2+ 1 # of non- chains/molecule 2 # hemes/molecule 4 # of hemes/globin chain 1 maximum # of O 2 carried by one molecule 4

Globin is encoded by genes present on chromosome #16 and chromosome #11

Hemoglobin Variants: Hb. A 1 2 2 comprises about 96% of all adult hemoglobin Hb. A 2 2 2 comprises < 2% of adult hemoglobin Hb. F 2 2 comprises < 2% of adult hemoglobin but is the dominant form in the fetus it is gradually replaced by Hb. A after birth
 Avg. 5 6 7 8 9 10 11 12 Blood")
A 1 C (%) Avg. 5 6 7 8 9 10 11 12 Blood Sugar (mmol/L)Avg. Blood Sugar (mg/d. L) 4. 5 6. 7 8. 3 10. 0 11. 6 13. 3 15. 0 16. 7 80 120 150 180 210 240 270 300 Hemoglobin A 1 c is a glycated hemoglobin (glucose binds to a terminal valine of the chain) Elevated Hb A 1 c levels are associated with uncontrolled diabetes mellitus

Fetal hemoglobin has higher O 2 affinity than adult hemoglobin Physiologically, is this is an advantage for the fetus ? ? ? Why or why not? ?

Sickle cell anemia is an inherited disorder in which abnormal hemoglobin is produced. The disease results from a mutation in the β-globin gene. The abnormal hemoglobin causes red blood cells to assume a sickle shape, like the ones seen in this photomicrograph. Why is the disease not manifested until the 5 th or 6 th month of postnatal life?

Objective 6 Hematopoiesis: Erythropoiesis blood cell formation Fetal Sites: yolk sac, liver, spleen, red bone marrow (after 19 weeks) Adult Sites: red bone marrow of the ribs, sternum, vertebrae, pelvis, scapulae, skull, proximal humerus and proximal femur Embryo model
 Red marrow to circulation Circulation")
A quick overview In red marrow (adult) Red marrow to circulation Circulation

Hemocytoblast: a pluripotent stem cell present in bone marrow that can differentiate into any of the formed elements Stem cells have two abilities: regeneration (mitosis) and differentiation

Erythropoiesis: Hemocytoblast: pluripotent stem cell capable of proliferation and differentiation into any of the formed elements Let’s review. What are the formed elements?

Myeloid Stem Cell: Either a Myeloid Stem Cell or an erythroblast ……. . Capable of proliferation and differentiation into any of the formed elements (except lymphocytes) Has receptors for erythropoietin (EPO)
 receptors; capable of proliferation and differentiation Basophilic erythroblast")
Proerythroblast committed cell; has erythropoietin (EPO) receptors; capable of proliferation and differentiation Basophilic erythroblast basophilic agranular cytoplasm (lots of r. RNA); hemoglobin synthesis Polychromatophilic blue staining basophilic RNA and pink erythroblast hemoglobin mix to form a grey colored cytoplasm

Orthochromatic erythroblast cytoplasm becomes increasingly pink as hemoglobin concentration increases; when hemoglobin concentration is about 34%, the nucleus is extruded (pyknosis) Reticulocyte ribosomes and r. ER clump (becomes a reticulum) reticulocytes enter the bloodstream and mature into erythrocytes within 48 hours the normal range for a reticulocyte count is 1 -2% of erythrocytes

What happens to cell size during erythropoiesis? cell gets smaller What happens to cell color during erythropoiesis? cells develop red color What happens to organelles during erythropoiesis? organelles degraded and nucleus is extruded What happens to cell number during erythropoiesis? increases, due to mitosis of hemocytoblasts and proerythroblasts

What do you think an elevated reticulocyte count might indicate? Predict what might happen to the recticulocyte count during the week after a person has donated blood
 Percent")
C. Nutritional requirements for erythropoiesis: 1. Iron: needed for hemoglobin synthesis Iron (grams) Percent of Total Hemoglobin 2. 7 66 Myoglobin 0. 2 3 0. 008 0. 1 < 0. 0001 --- Intracellular Storage (Ferritin, Hemosiderin) 1. 0 30 Intracellular Labile Iron (Chelatable Iron) 0. 07 (? ) 1 Intercellular Transport (Transferrin) 0. 003 0. 1 Compartment Heme Proteins (cytochromes) Non-heme Proteins

Nutrient Function Vitamin B 12 DNA Synthesis absorption requires the presence of IF (intrinsic factor) produced by parietal cells of the stomach lining
 Folic acid DNA synthesis Vitamin C Antioxidant; keeps iron in its reduced")
Nutrient Function(s) Folic acid DNA synthesis Vitamin C Antioxidant; keeps iron in its reduced state which helps with iron absorption Nicotinic Acid Pantothenic acid Biotin, Thiamine intermediary steps in metabolism Amino Acids Globin Synthesis

Iron absorption, storage and transport

Iron transport and storage Transferrin Ferritin/Hemosiderin Free iron is toxic! And, it is so small that if it circulates by itself it could get filtered by the kidney and lost……. . See if you remember. Transferrin is a ____ protein, and therefore it is most likely produced by the _______.

Intrinsic Factor: 1. Produced by parietal cells of the stomach lining 2. Needed for vitamin B 12 absorption

D. Regulation of Erythropoiesis RBCs are produced at the rate of approximately 2 X 106/second The rate of erythropoiesis is controlled by erythropoietin (EPO), a glycoprotein hormone produced primarily by kidney cells and liver cells EPO acts on erythroprogenitor cells and accelerates erythropoiesis EPO production is stimulated by testosterone and inhibited by estrogen
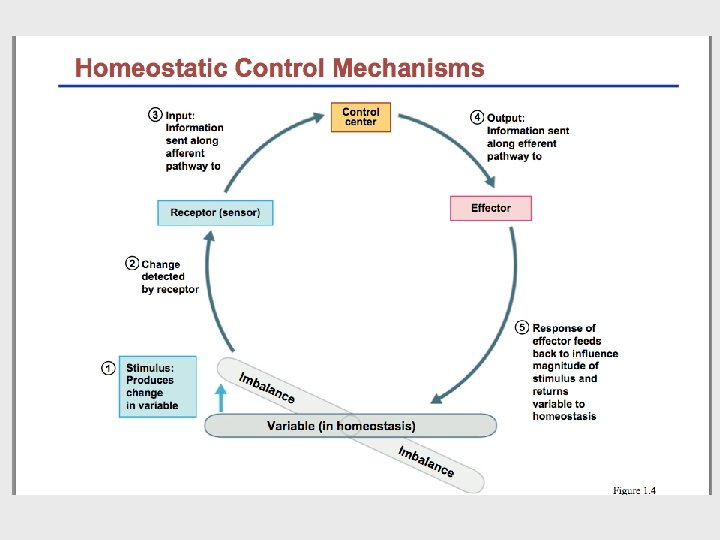

Normal levels: 11 -18 /ml Hypoxia Increased O 2 carrying capacity of the blood EPO binds to proerythroblasts Enhanced erythropoiesis increases the RBC count Stimulus? Causes? hypoxia Efferent Pathway? Kidney and liver secrete EPO erythropoitein Low RBC count, defective Hb, O 2 deficient environment Effector? Positive or Negative feedback? Negative red bone marrow
: 1. anemia")
Erythropoietin is released into the plasma when blood O 2 decreases (hypoxia): 1. anemia (decreased RBC count, decreased or defective Hb) 2. lung disease which decreases O 2 uptake 3. low O 2 environments 4. increased use of O 2 by tissues (intense aerobic activity) Other factors which boost erythropoiesis, either by increasing EPO or by acting directly on proerythroblasts: Testosterone Placental lactogen Vasopressin (ADH) Thyroid hormone Angiotensin Prolactin Norepinephrine

Questions: What happens to the RBC levels in: dialysis patients with kidney disease ? Decrease, why? ovarectomized subjects ? Increase, why? castrated subjects ? Decrease, why? laboratory subjects breathing pure O 2 ? Decrease, why? Besides increased erythropoiesis, what other compensatory behaviors would the body activate during conditions of hypoxia? elevated heart rate, elevated ventilation rate, elevated arterial pressure

Cigarette smoke produces carbon monoxide. If a nonsmoker smokes a pack of cigarettes a day for several weeks, what would happen to the person’s hematocrit? Explain your answer. 1. What effect does CO have on RBC function? 2. What does this mean in regards to O 2 carrying capacity of the blood? 3. What is the bodies response to your answer to question number 2? 4. So what happens to hematocrit?

Objective 7 Erythrocyte Degradation Erythrocyte life span is 100 -120 days. Damaged, or defective erythrocytes are engulfed by macrophages of the liver, spleen and bone marrow Macrophages engulf and destroy erythrocytes hemoglobin heme Iron globin biliverdin Carried by albumen to the liver bilirubin amino acids (recycled or bile urobilinogen stored) stercobilin (feces) urobilin (kidneys)

Macrophage Biliverdin Bilirubin In the liver incorporated into bile Bile is secreted into intestine Becomes urobilinogen Intestine Stercobilin Feces Kidney Urobilinogen Urine

Let’s review • What happens to globin portion of hemoglobin? • What happens to heme? – Iron – protoporphyrin ring

Let’s see if you got this material! Where are red blood cells produced and where are they mainly destroyed? What two gasses are carried by hemoglobin? How many oxygens can one hemoglobin molecule bind? Is oxygen stored in the mitochondria of red blood cells? Which component of hemoglobin breakdown is not recycled? Is it normal to see a polychromatophilic erythroblast in a blood smear?

Objective 8 A. Polycythemia Erythrocyte Disorders excess number of RBCs (> 7 X 106/mm 3) Normal Blood Smear Polycythemia Vera

B. Anemia: 1. Any condition in which the blood has abnormally low O 2 carrying capacity 2. Causes include reduced numbers of RBCs, reduced concentration of hemoglobin or synthesis of abnormal hemoglobin What are some causes? Reduced rate of erythropoiesis Excessive hemolysis Excessive bleeding

Classification of anemias: 1. Those based on RBC morphology: Red blood cell size Red blood cell color microcytic (small cells) hypochromic (pale cells) normocytic (normal size) color) normochromic (normal macrocytic (large size) hyperchromic (dark cells) Hypocytic, hypochromic Anemia (Iron deficiency) Hypercytic, normochromic Anemia (Autoimmune hemolytic)

Anemias Caused By Reduced Erythrocyte Number Hemorrhagic Anemia Hemolytic Anemia Aplastic Anemia Hemolytic anemia

Anemias Caused By Reduced Hemoglobin or Abnormal Hemoglobin Iron deficiency anemia Pernicious anemia Sickle cell anemia Thalassemia Iron Deficiency Anemia Pernicious Anemia Sickle cell Anemia
- Slides: 51