Obesity Epidemic Mohammed I Tarrabain M D St

Obesity Epidemic Mohammed I. Tarrabain, M. D St. Vincent Medical Group IAFP Spring CME & Research Day May 7, 2015

The Obesity Epidemic • In the United States, it is estimated that 93 million Americans are affected by obesity. • In 2001, the states with the top five percentages for obesity were Mississippi, West Virginia, Michigan, Kentucky and Indiana- Overweight and Obesity (2010) 2/3 rd (65. 9%) overweight, with a BMI of 25 or greater. 1/3 rd (29. 6%) obese, with a BMI of 30 or greater. CDC. Behavioral Risk Factor Surveillance System: Prevalence and Trend Data–Overweight and Obesity, U. S. Obesity Trends, Trends by State 2010. Available online at http: //www. cdc. gov/ brfss/

The Obesity Pandemic

…In the United States • More than one‐third of adults and one‐sixth of children and adolescents are obese. • This is more than double the prevalence in 1994.

The Future • Childhood obesity, in the past 30 years, has more than doubled in children and quadrupled in adolescents • Obese Children who are 70 percent more likely to continue being obese into adulthood.

BMI for children • Even worse, being affected by childhood obesity at a young age are predisposed to obesity and severe obesity in adulthood. “Early Adiposity rebound”

Obesity impact in Elderly

Obesity & Mortality

Obesity & Cancer

Obesity Disease ICD 278. 00

Obesity Disease • In 2000, a National Institutes of Health panel was one of the first to describe obesity as a chronic disease. • More recently, the AMA adopted a policy in June 2013 recognizing obesity as a disease, “with the hope that doing so will help change how the medical community tackles this complex issue. ”

• Obesity is a multifactorial disease that results from a combination of both physiological, genetic, and environmental inputs.
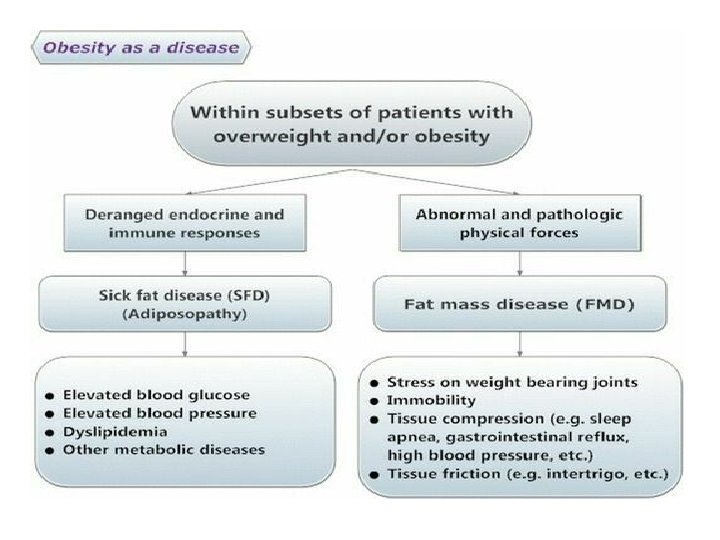

“sick fat” • Adipose tissue has no less pathogenic potential than other body organs, with adiposopathy being analogous to cardiomyopathy, neuropathy… • Adiposopathy or “sick fat” is defined as adipocyte/adipose tissue dysfunction caused by positive caloric balance and sedentary lifestyle in genetically and environmentally susceptible individuals. • This results in adverse endocrine and immune responses that both directly and indirectly contribute to metabolic disease and increased CVD risk.
 may be more metabolically active than subcutaneous")
Fat “storage” • Visceral adipose tissue (VAT) may be more metabolically active than subcutaneous adipose tissue (SAT). • These depots (VAT) inherently differ in processes involving lipolysis/lipogenesis, expression of adipocyte receptors, and differ in the secretion of adipokines/cytokines, enzymes, hormones, immune molecules…

• From a clinician standpoint, recognizing the pathogenic potential of adipose tissue may give a clearer rationale toward recommending weight reduction to overweight/obese patients.

E = mc 2 • Some obese patients believe that their metabolic fate is unavoidable, irrespective of intervention, and come to develop the defeatist belief that they will always gain fat mass, even if they reduce consumption of calories/energy.

Let’s be reasonable,

The brain! • The brain is the central location of behavior and hunger, and the hypothalamus is a target for weight management pharmacotherapies.

Lessons…
 lorcaserin (Belviq)")
New anti‐Obesity drugs Hit the market in the past 3 years: 1) lorcaserin (Belviq) 2) phentermine/topiramate (Qsymia) 3) naltrexone/bupropion (Contrave) 4) liraglutide (Saxenda)

New Guidelines • Headed by the Endocrine Society with support from the Obesity Society and the European Society of Endocrinology. • The new guidelines expand on ones for managing overweight and obesity in adults that were released in 2013 by the Obesity Society, the American Heart Association, and the American College of Cardiology.

Classic Guidelines • USPSTF: “physicians should offer or refer their patients with obesity for high‐intensity multicomponent behavioral interventions” • For patients who do not meet their target weight, intensification of therapy is needed. Options include: additional behavioral therapy; modifying dietary protocols; referral dietitian; the addition of pharmacotherapy that promotes weight loss; referral for bariatric surgery.

Natural History of Wt Loss Programs • With the best of lifestyle interventions, the average weight loss, was 5%‐ 10% in 6 months. • Not all patients are successful in achieving even 5% WL due to compensatory mechanisms in appetite and metabolic rate. • Furthermore, the usual pattern after 6 months is a period of weight stabilization (plateau); or weight regain gradually in many patients. the Look AHEAD study

Goals of Treatment • Indeed, in clinical studies of approved medications, substantially more patients are able to achieve 5% to 10%, or even 15% weight loss compared with placebo. • In practice, the weight loss goal for a patient is approximately 5% to 15%. • If achieved and maintained, these modest and moderate weight loss targets are well known to improve health indices.

Impact of weight loss • Bariatric surgical procedures produce weight loss by restricting the size of a meal (all procedures) and by their effects on gut hormones that affect appetite, such as gastric bypass and gastric sleeve. These procedures have been shown to not only produce weight loss, but to have a positive impact on diabetes, hypertension, dyslipidemia and even mortality.


Current “Combination Rationale” • Because combination pharmacotherapy for obesity deploys medications with differing mechanisms of action, it offers the prospect of overcoming the counter‐regulatory mechanisms that become manifest in the weight‐reduced state. • Combination therapy also allows prescription of lower doses of each medication to minimize adverse effects

Rationale for using medications • Prescription medications serve as an adjunct to lifestyle changes in order to produce the negative energy balance that is required for weight loss. • Medication does not work on its own—however, it does suppress the appetite to help the patient ingest fewer calories. • With less hunger, more satiety, and the ability to resist food cues induced by medications that act on central appetite centers, patients will be better able to adhere to their diet.

“Obesity Based Medicine” • While a wide variety of medications have been utilized to promote weight loss, only those shown to be effective and approved by the FDA for chronic obesity management should be utilized.

Obesity “Chronic Condition” • long‐term use of medication for weight loss is most effective when continued indefinitely. • The patient should be monitored periodically. • Address patient concerns, and provide ongoing support…. (most important)

… and lifestyle • Medications are best suited for patients who are motivated to lose weight and adherent to lifestyle intervention since the combination is more effective than lifestyle intervention or pharmacotherapy alone.
 ≥ 30 • or ≥ 27 who have other risk")
PHARMACOTHERAPY CRITERIA • (BMI) ≥ 30 • or ≥ 27 who have other risk factors or diseases, (comorbidities) such as hypertension, dyslipidemia, cardiovascular disease, diabetes, fatty liver disease, and obstructive sleep apnea. . .

Two Drugs for Weight Loss • In 2012, the FDA approved one new drug and a new combination of 2 old drugs as adjuncts to lifestyle changes for chronic weight management.
.")
Qsymia q Qsymia is a fixed‐dose combination Phentermine and Topiramate(ER).
: a randomised, placebo‐controlled, phase 3 trial. • Interpretation: Ø The combination")
Qsymia • (CONQUER): a randomised, placebo‐controlled, phase 3 trial. • Interpretation: Ø The combination of phentermine and topiramate, with office‐based lifestyle interventions, might be a valuable treatment for obesity that can be provided by family doctors. JAMA. 2013; 310(6): 637‐ 638.

Qsymia • The most commonly observed adverse events: dry mouth constipation paresthesia dysgeusia
 7. 5 mg/46 mg")
Qsymia Dose: dose escalation required • Target: Phentermine/Topiramate(ER) 7. 5 mg/46 mg
 is a selective serotonin (5 HT) 2 C receptor agonist.")
Belviq q Belviq (Lorcaserin) is a selective serotonin (5 HT) 2 C receptor agonist.

Belviq • The BLOOM, BLOSSOM, and BLOOM‐DM trials involved 7, 648 overweight or obese patients. • In the BLOOM‐DM trial, which included only patients with diabetes, lorcaserin 10 mg once or twice daily led to significant improvement in the glycated hemoglobin (Hb. A 1 c) compared with placebo (‐ 1. 0% vs ‐ 0. 9% vs ‐ 0. 4%, respectively; P <. 001 for both doses of lorcaserin vs placebo). Obesity. 2012 Jul; 20(7): 1426‐ 36.

Belviq • Lorcaserin has been shown to have a favorable tolerability profile. Most common: headache, nausea, dizziness, back pain and fatigue.

Belviq • 10 mg twice daily, the dose approved by the FDA
 • Across the 3 trials, new heart valvulopathy occurred in 2. 37%")
Belviq (safety) • Across the 3 trials, new heart valvulopathy occurred in 2. 37% of lorcaserin patients and 2. 04% of placebo patients (risk ratio, 1. 16; 95% confidence interval, ‐ 0. 46 to 1. 13). • Remember: cardiac 5 HT‐ 2 B receptors (Fenfluramine in Phen‐Fen) produces valvular heart disease not 5 HT‐ 2 C (Belviq) • One concern is the use of lorcaserin with other serotonergic drugs since there is a possible risk of serotonin syndrome. For example SSRIs…

Contrave Approved by FDA in September 2014 for obesity. q. Bupropion SR/Naltrexone SR

Food!

Contrave • The combination of naltrexone SR and bupropion SR simultaneously stimulates hypothalamic anorexigenic (satiety) neurons and blocks orexogenic (hunger) ones. • Plus, this combination also has the potential to modulate the mesolimbic reward system and regulate dopamine midbrain areas to reduce food intake.

Contrave • Primarily because of adverse events, the completion rate was low in phase III trials with rates ranging from 54‐ 58%

Contrave Adverse events included: • Nausea, headache, constipation, dizziness, vomiting, dry mouth, tremor, abdominal pain, bronchitis, and tinnitus.
 • FDA approved December 23 rd, 2014 •")
Saxenda q Liraglutide 3 mg (Saxenda®) • FDA approved December 23 rd, 2014 • Also, “First New Anti-Obesity Drug in Canada in Two Decades”
 agonists • mimic GLP‐ 1,")
GLP‐ 1 • Glucagon‐like peptide receptor (GLP‐ 1 R) agonists • mimic GLP‐ 1, an incretin gut hormone secreted when a meal is ingested. • GLP‐ 1 lowers glucose by increasing insulin output and decreasing glucagon secretion, both in a glucose‐dependent manner (no hypogylcemia) • GLP‐ 1 Rs are expressed in the periphery and in several areas in the brain that are implicated in the regulation of appetite.

Saxenda • Liraglutide demonstrated significant dose‐ dependent weight loss in studies of patients with type 2 diabetes mellitus (T 2 DM) and has led to its investigation and recent submission to the FDA for approval for the treatment of obesity.

Saxenda • A phase III study randomized patients with obesity but without DM. • Over the 56 weeks of treatment, patients treated with liraglutide lost significantly more weight, and significantly more liraglutide‐ treated patients lost and maintained ≥ 5% or ≥ 10% of randomization weight

“the more the better” • dose, Liraglutide 1. 2, 1. 8, 2. 4, 3. 0 mg

Saxenda • The most frequent drug‐related adverse events were mild to moderate, transient nausea and vomiting. • “desirable nausea”

Childhood Obesity
 with lifestyle intervention, such as a low‐fat diet calorie‐reduced")
Orlistat • Orlistat (Xenical, Alli) with lifestyle intervention, such as a low‐fat diet calorie‐reduced diet, resulted in weight loss long term. • Orlistat is also associated with reductions in low‐density lipoprotein cholesterol (LDL‐C) • The safety profile of orlistat is good. It is the only obesity medication approved for use in adolescents • Available both by prescription (120 mg 3 times daily) and OTC (60 mg) • However, gastrointestinal adverse events (oily spotting, flatulence, and fecal urgency) limit patient acceptance, although these symptoms are generally mild and transient (again, diet compliance. . ) • Kidney stones may occur in patients at risk for renal insufficiency and in rare cases serious liver injury have been reported with orlistat. • Remember to supplement with vitamins.

Opening the Door…

Context Barriers to Discussing Weight by Health Care Providers: ◦ Concern over offending patient ◦ Belief that patients are not motivated to make changes and that counseling will be ineffective ◦ Time ◦ Payment ◦ Lack of knowledge and skills ◦ Lack of practical tools

Primary care literature “I’m afraid raising the issue of weight will offend my patient. ” “What difference could my counseling efforts make anyway? My patients won’t follow my recommendations and won’t lose weight? ” “I don’t have the time. ” “I don’t get paid for obesity counseling. ” “I’m not sure how to do this. ” “I don’t’ have practical tools with which to do this. ”

Scenario “No health care provider has ever discussed weight with patient before and he/she is in your office…”

Raising the Issue of Weight Language. • Preferred term is “weight” “Achieving and/or maintaining a healthy weight” o Least desirable term is “fat” or “fatness” o The term “obesity” could be avoided. Permission. An example: “Evelyn, now that we’ve addressed your main reason for the visit, I’d like to discuss the issue of weight. Would that be ok with you? ”
 2) 3) 4) 5) Ask (or Assess) Advise Agree Assist")
5 As Paradigm 1) 2) 3) 4) 5) Ask (or Assess) Advise Agree Assist Arrange

ASK ü How ready are you to lose weight? v“Would you be interested in working together on helping you make changes in your lifestyle over a period of time which would help you achieve a healthier weight? ” ü What do you believe you could do to get to a healthier weight?

Assessing Readiness to Change How ready are you to lose weight? • I have not really thought about it (pre-contemplation) • I mean to lose weight but I don’t actually get around to it. (contemplation) • From time to time, I go on a diet/exercise, but then I stop after a few days (preparation) • I have been working on losing weight for the past 6 months (action) • I have kept my weight off for over 6 months (maintenance) Readiness to change (Huang J et al, 2004)

ASK “Would you be interested in working together on helping you make changes in your lifestyle over a period of time which would help you achieve a healthier weight? ”

Asking/Assessing Motivation… “What do you believe you could do to get to a healthier weight? ” The moment of truth… “what are the main reasons you would like to lose weight, and why now? ”

ADVISE An “opportunity” to advise about impact of behaviors on weight and health.

Calories? ? Bottom Line • It’s the calories and all calories count • Goal is a 500 ‐ 750 k/cal/day energy deficit o Prescribe 1200‐ 1500 k/cal/day range (low calorie diet)

Exercise “Exercise and diet go together. Weight management is most successful when careful attention is given to both physical activity and proper nutrition. ” American College of Sports Medicine, 2013 • Physical Activity: The Look AHEAD Study – unsupervised – 175 minutes moderate intensity/week – 5 days/week – walking!!!

AGREE “Negotiating” framework: SMART goals S – specific M – measurable A – achievable R – rewarding T – in what time period

Assist & Arrange Assistance ◦ Obesity tx… ◦ Recommending supportive apps/programs… ◦ Warn about what doesn’t work: commercial wt loss…

Arrange • Follow‐up appropriately. • Reinforcement. • Support‐ most important!

Thank you
- Slides: 73