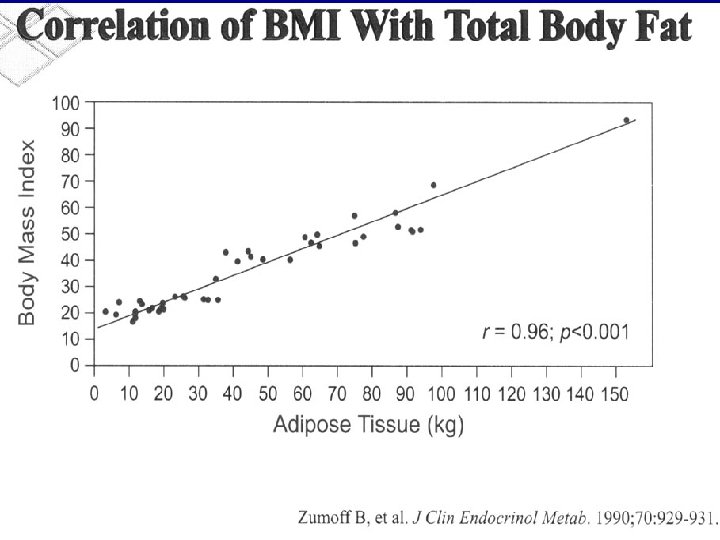
Obesity An excess of body fat body mass

 >30 kg/m 2")
Obesity • An excess of body fat; body mass index (BMI) >30 kg/m 2 • Affects ~30% adults in U. S. ; $70 Billion annual health cost • Co-morbidities (CAD, HTN, DM II) affect increasing mortality risk in proportion to BMI
![Body Mass Index -kg/m 2 [Wt(lb) x 703/Ht (inches)2 ] • • • Underweight](http://slidetodoc.com/presentation_image_h2/572f1f7e0156a5dc87c98840a3a800c4/image-3.jpg "Body Mass Index -kg/m 2 [Wt(lb) x 703/Ht (inches)2 ] • • • Underweight")
Body Mass Index -kg/m 2 [Wt(lb) x 703/Ht (inches)2 ] • • • Underweight Normal Overweight Obese Severe (morbidly) obese <18. 5 -24. 9 25 -29. 9 >30 >40

Obesity rates, 1991 vs 2000 Obesity defined as BMI>30. Data were obtained by calculating BMI from phone questionnaire on height and weight on 185000 participants >age 18. CDC study , JAMA 2001; 286, 1195 -1200

A typical fast food meal • Big Mac: 570 kcal • Large Fries: 540 kcal • 32 0 z (large) soda: 400 kcal TOTAL 1510 kcal A 70 kg moderately active man requires 2100 kcal/day (3 meals).
, HTN (40% of")
Obesity co-morbidities • Metabolic syndrome: DM II (15% of all obese), HTN (40% of obese), & hyperlipidemia related to visceral adiposity and insulin resisitance • Sleep apnea • Cardiopulmonary failure • Osteoarthritis • Gallstones • GERD • NASH • Breast cancer

Increases in obesity and diabetes 1991 -2000

Medical management of obesity • Energy equation: wt stability when calories in = calories out • Can therefore reduce by decreasing intake and/or increasing expenditure of calories
 +")
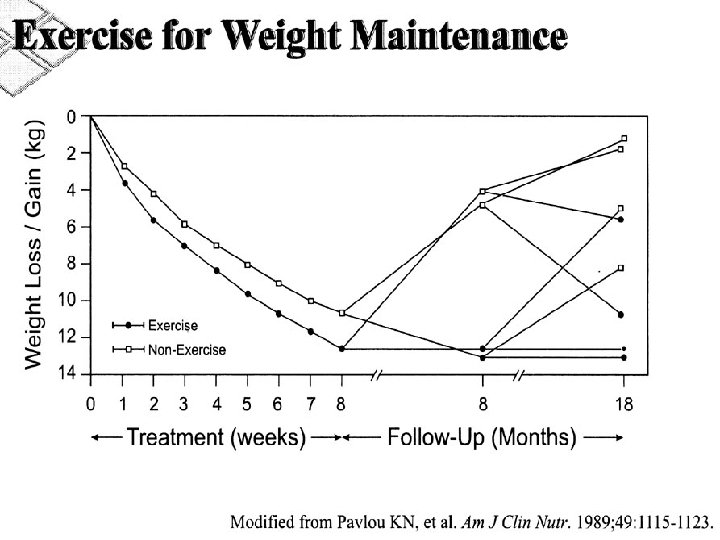
Medical management of obesity • Diet (according to ideal body weight for height) + exercise (30 min/d moderate 5 d/wk) + behavioral modification = 510% wt loss in 6 months, most rebound. • Very low calorie dieting (<900 kcal/d: works for many, but 99% rebound • Pharmacological adjuncts: limited success
 • Incidence in U. S. population: 2. 1%")
The super-obese (BMI 50 + ) • Incidence in U. S. population: 2. 1% (4. 4 million) • Increased risk of osteoarthritis, cardiopulmonary failure, sleep apnea, all consequences of metabolic syndrome (DM, NASH, HTN, hyperlipid) • Medical treatment essentially hopeless, though met syndrome improves with 5 -10% weight loss


Rationale for surgery for morbid obesity • >2 x mortality with BMI>40 kg/m 2 due to cardiopulmonary failure, sleep apnea, diabetes • Poor results of all medical therapies to date • Relative safety and efficacy of gastric bypass compared to older jejuno-ileal bypass procedure

Criteria for obesity surgery • BMI > 40, or >35 with significant comorbidities • Documented failure of medical management (diet + exercise; pharm) • Psychological ability to undergo surgery • Absence of other chronic disease

What are the surgical options? • Restrictive: Adjustable gastric banding & Vertical band gastroplasty • Malabsorptive: Roux-en-Y gastric bypass & Biliopancreatic diversion

• Adjustable gastric band • Vertical band gastroplasty

• RGB • BPD

BPD-DS

Estimated Number of Bariatric Operations Performed in the United States, 1992 -2003 Steinbrook, R. N Engl J Med 2004; 350: 1075 -1079

Laparoscopic Versus Open Gastric Bypass: A Randomized Study of Outcomes, Quality of Life, and Costs Nguyen, Ninh T. MD*; Goldman, Charles MD*; Rosenquist, C. John MD†; Arango, Andres BS*; Cole, Carol J. BS*; Lee, Steven J. MS* and; Wolfe, Bruce M. MD, FACS
 or")
• 155 patients w/ BMI 40 -60 randomly assigned to lap (79) or open (76) Nguyen et al. Laparoscopic Versus Open Gastric Bypass: A Randomized Study of Outcomes, Quality of Life, and Costs. Ann Surg. 234, 2004. 279 -91.

OUTCOMES Nguyen et al. Laparoscopic Versus Open Gastric Bypass: A Randomized Study of Outcomes, Quality of Life, and Costs. Ann Surg. 234, 2004. 279 -91.

OUTCOMES Nguyen et al. Laparoscopic Versus Open Gastric Bypass: A Randomized Study of Outcomes, Quality of Life, and Costs. Ann Surg. 234, 2004. 279 -91.

OUTCOMES Nguyen et al. Laparoscopic Versus Open Gastric Bypass: A Randomized Study of Outcomes, Quality of Life, and Costs. Ann Surg. 234, 2004. 279 -91.

OUTCOMES Nguyen et al. Laparoscopic Versus Open Gastric Bypass: A Randomized Study of Outcomes, Quality of Life, and Costs. Ann Surg. 234, 2004. 279 -91.

OUTCOMES Nguyen et al. Laparoscopic Versus Open Gastric Bypass: A Randomized Study of Outcomes, Quality of Life, and Costs. Ann Surg. 234, 2004. 279 -91.

CONCLUSIONS • Laparoscopic GBP is safe alternative to open GBP – Lap pt ‘s benefited from dec EBL, shorter LOS & more rapid improvement in QOL than open GBP
- Slides: 28