Nuts Bolts Things to Consider when Preparing IRB

Nuts & Bolts: Things to Consider when Preparing IRB Submissions Amanda Coltes-Rojas, MPH, CIP Human Subject Research Office Associate Director, Regulatory Affairs & Educational Initiatives Pediatric Clinical Research Forum April 2 nd, 2008

Overview • • • Regulatory Oversight Types of Review Assessing Risk in Pediatric Research Consent/Assent Wards of the State HSRO Process
 • The mission of the Office for Human Research")
Regulations Overview (DHHS & FDA) • The mission of the Office for Human Research Protections (OHRP) is to monitor and promote compliance with regulations set forth from the Department of Health and Human Services (DHHS) that relate to the ethical standards of research involving human subjects (45 CFR 46). – Subpart D • Any research involving a drug, a biologic, or a medical device is subject to Food & Drug Administration (FDA) regulation (21 CFR 50, 56, 312, 812) – Adopted Subpart D, 4/01
 • Children are persons who have not attained the legal age")
Definitions (Subpart D) • Children are persons who have not attained the legal age for consent to treatments or procedures involved in the research, under the applicable law of the jurisdiction in which the research will be conducted. • Assent means a child's affirmative agreement to participate in research. Mere failure to object should not, absent affirmative agreement, be construed as assent. • Disorder or condition relates to a specific characteristic which describes a group of children, a physical, social, psychological, or neurodevelopmental condition affecting children, or the risk of certain children developing a disease in the future based on diagnostic testing or physical examination.

Types of Review • Exempt No more than minimal risk vs. • Expedited More than minimal risk • Full Board

Exempt Review: Things to Keep in Mind • These studies involve the least amount of risk to participants. • Categories 1 -6 as listed in the DHHS regulations are for new protocol submissions • Primarily involves: – education research – surveys, interviews, etc. – analysis of existing data • Reflects the concern about protecting the subjects privacy and avoiding any risks associated with breach of confidentiality. – Data is anonymous and disclosure of the responses would not place subjects at risk of criminal or civil liability or be damaging to the subjects' financial standing, employability, or reputation

Expedited Review: Things to Keep in Mind • No greater than minimal risk • May not be used where identification of the subjects and/or their responses would reasonably place them at risk – criminal or civil liability; be damaging to the subjects’ financial standing, employability, insurability, reputation; be stigmatizing, – reasonable and appropriate protections must be implemented so that risks related to invasion of privacy and breach of confidentiality are no greater minimal • Categories 1 -7 for new/continuing review; Categories 8 -9 for continuing review of research initially approved by the convened IRB
 & FDA 21 CFR")
What is Minimal Risk? • DHHS 45 CFR 46. 102(i) & FDA 21 CFR 56: – The probability and magnitude of harm or discomfort anticipated in the research are not greater in • OHRP guidance: and of themselves than those – Minimal risk is relative to ordinarily encountered in daily the daily life of a normal, life or during routine physical healthy person. The risk or psychological exams or threshold cannot tests increase because the person is sick and faces greater risk due to illness.

What is Minimal Risk? • OHRP guidance: – Minimal risk is relative to the daily life of a normal, healthy person. The risk threshold cannot increase because the person is sick and faces greater risk due to illness. • National Human Research Protection Advisory Committee (NHRPAC) guidance: – Minimal risk is risk level associated with the daily activities of a normal, healthy, average child.
 • Level")
Interpretation of Risk: 45 CFR 46. 404 (FDA 21 CFR 50. 51) • Level of risk is no greater than minimal regardless of whether the research offers the prospect of direct benefit to the child – socially allowable risks which parents generally permit their children to be exposed to in non-research settings – should take into account the differing risks experienced by children of different ages – if certain groups of children are routinely exposed to greater risks because of circumstances in which they live, their level of increased risk should not be interpreted as minimal just because it is part of their common experience
 • Research")
Interpretation of Risk: 45 CFR 46. 405 (FDA 21 CFR 50. 52) • Research involving greater than minimal risk – presenting the prospect of direct benefit to individual subjects – risk is justified by anticipated benefits to subjects – relation of anticipated benefit to the risk is at least as favorable to the subjects as that presented by alternative approaches
 • Research")
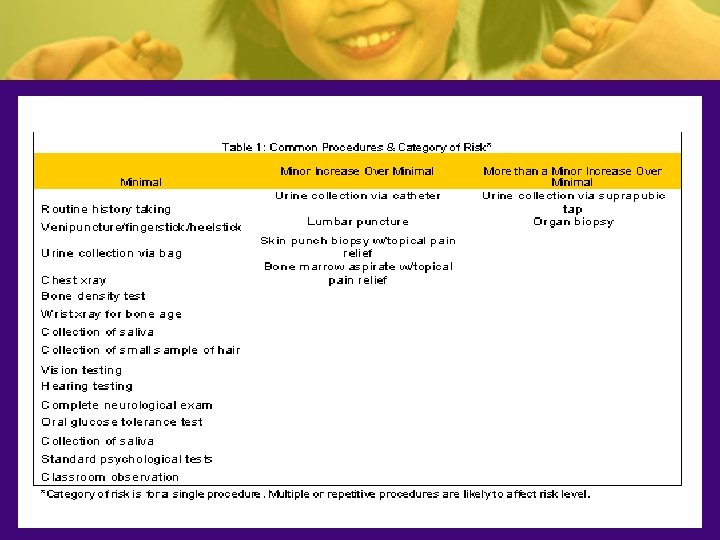
Interpretation of Risk: 45 CFR 46. 406 (FDA 21 CFR 50. 53) • Research involving greater than minimal risk – Minor Increase Over Minimal Risk – No prospect of direct benefit to an individual child, but likely to yield generalizable knowledge about the child’s disorder or condition • Risks should be commensurate with the risks of interventions or procedures experienced or expected to be experienced in the lives of children with a specific disorder or condition. • Research should have substantial promise to contribute to the understanding or amelioration of the subject’s disorder, or condition.

Minor Increase Over Minimal w/o Prospect of Direct Benefit: Research Examples Infancy Prematurity Adolescence Living in a compromised physical environment Genetic predisposition to future illness Poverty Institutionalization

Risk Amelioration • Important to consider the context of the research. • Consider social and cultural factors of subject population to evaluate increase or decrease of risk as it pertains to specific group. • In one setting certain risks considered minor increase over minimal while the same risk in another setting would be more than a minor increase over minimal risk.

Minimizing Risks • Procedures should only be performed by professionals skilled with children; • Protocols should include guidelines setting limits on the number of attempts at a procedure (i. e. , venipuncture) or the length of time for completion of a questionnaire; • Appropriate methods should be used to orient the child to the study and decrease anxiety and discomfort; • Plans should be developed to protect subjects from breaches in privacy and confidentiality.

HSRO Policy: Consent • Under age 18, consent must be obtained from the child’s biological or adoptive parents, or court-appointed legal guardian

HSRO Policy: Assent • Applies to children 7 through 17 years of age. • Failure to object is not assent • IRB determines whether and how assent is to be documented • Assent is required except: – when child is not capable: age, maturity, or psychological state; – when research presents direct benefit; important to the child’s well-being and available only in context of research
: a child who is")
Wards of the State • FDA 21 CFR 50. 3(q): a child who is placed in the legal custody of the State or other agency, institution, or entity, consistent with applicable Federal, State or local law. • Florida Statute 755. 102(2) : a person for whom a guardian has been appointed.

Wards: Things to Keep in Mind • Wards can be included if the research is related to their status as a ward; OR • Conducted in schools, camps, hospitals, institutions, or similar settings in which majority of children involved are not wards. • Specific authority from the court must first be obtained

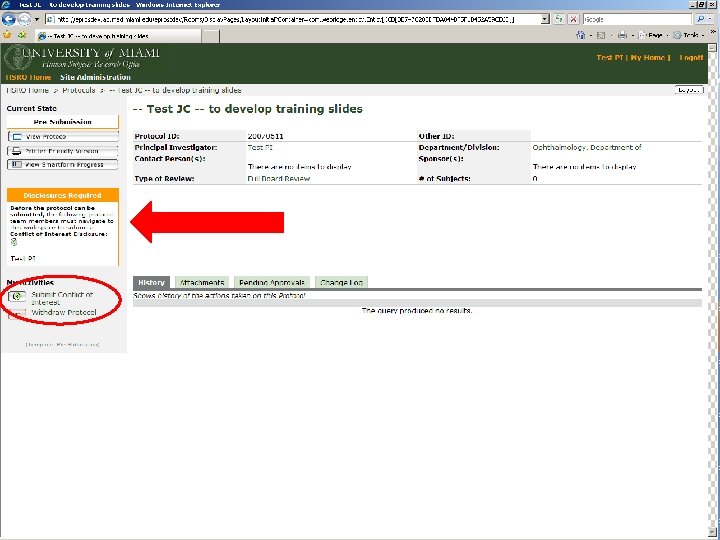
HSRO Process: Things to Keep in Mind • All departments electronically enabled as of March 15, 2008 • Office has two areas of “pre-review”: exempt/expedited and full board. • Protocol information must first be captured on e. Prost (electronic protocol submission and tracking system). § All users must request an e. Prost account: https: //eprost. med. miami. edu • Once it is entered on e. Prost, the submission may require varying levels of departmental review and/or ancillary committee review. • JHS/CRRC process is parallel to HSRO/IRB process and required of any study utilizing JHS resources.

HSRO Office Flow Average time for completion of review process/IRB determination = 4 -6 weeks Study cannot begin until PI has received approval notification from the IRB. Determination Letter IRB Regulatory Specialist (Exempt & Expedited Review) Submission arrives At HSRO IRB Chair/Designee IRB Regulatory Analyst (Full Board Review) Full Board
 Study team unsure of when HIPAA Waiver or HIPAA")
Common Delays: New Submissions 1) Study team unsure of when HIPAA Waiver or HIPAA authorization form is required; 2) Conflict of Interest Disclosures have not been submitted for all study team members; 3) Study requires use of ancillary committee;
 JHS/CRRC application & forms must be submitted for approval")
Common Delays: New Submissions 4) JHS/CRRC application & forms must be submitted for approval from CRRC for use approval of JHS resources; 5) IND/IDE information is incomplete; 6) Study is in ancillary committee review 7) Study supporting documentation was omitted (e. g. , ICFs, questionnaires, data collection sheet).
 Standard of Care vs. Care for Research Purposes: PI")
Common Delays: New Submissions 8) Standard of Care vs. Care for Research Purposes: PI should be as detailed as possible in question 4. 6. - risks involved with medical standard of care procedures vs. risks due to research procedures 9) e. Prost forms do not contain sufficient information
 Study team unsure if event constitutes an unanticipated problem involving")
Common Delays: UPIRTSOs 10) Study team unsure if event constitutes an unanticipated problem involving risk to self or others – Do not hesitate to contact HSRO to discuss if event requires reporting.
 Meaning Pre-submission Submission information entry in smartform is")
Submission States & Meanings State (“Status”) Meaning Pre-submission Submission information entry in smartform is in progress; PI has NOT clicked on “submit” Originating Department Review PI has clicked on “submit”; originating department is reviewing study. Depending on department, it could be a three-step process: administrative review, scientific review, chair’s review. Ancillary Committee Review Correlates to information entered by study team on section 2 b. and question 3. 7 (JHS-related activities). Pre-Board Review Submission has arrived at HSRO inbox Regulatory Review Ownership of the submission has been assigned to either a regulatory specialist

Submission States & Meanings State Meaning Awaiting Meeting Assignment (applies to FULL BOARD submissions only) Submission is waiting assignment to a meeting agenda. IRB Meeting Assigned (applies to FULL BOARD submissions only) Submission has been assigned to a meeting. Meeting Complete/Post-Board (applies to FULL BOARD submissions only) Determination complete; study documents going through final preparation (e. g. , watermarking of all supporting documentation). Approval (or Deferred to Chair; Deferred to Full Board; Disapproved) Determination has been made by the IRB and notification sent to the PI.

References • • HSRO Policies & Procedures: https: //eprost. med. miami. edu/ Bankert, E. A. , Amdur, R. J. Institutional Review Board Management and Function. Boston: Jones and Bartlett Publishers; (2006). • http: //ctep. cancer. gov/forms/nhrpac 16. pdf • http: //hhs. gov/ohrp/

- Slides: 31