Nutritional consequences after bariatric surgery Dr Reem Murad

Nutritional consequences after bariatric surgery Dr : Reem Murad

A growing consensus favors bariatric surgery � “Bariatric surgery should be considered for adults with BMI ≥ 35 kg/m 2 and type 2 diabetes, especially if the diabetes is difficult to control with lifestyle and pharmacologic therapy. ” � – American Diabetes Association (2009) � “When indicated, surgical intervention leads to significant improvements in decreasing excess weight and co-morbidities that can be maintained over time. ” – American Heart Association (2011) � “Bariatric surgery is an appropriate treatment for people with type 2 diabetes and obesity not achieving recommended treatment targets with medical therapies” � – International Diabetes Federation (2011) � “The beneficial effect of surgery on reversal of existing DM and prevention of its development has been confirmed in a number of studies” � – American Association of Clinical Endocrinologists (2011) Sources: American Diabetes Association. Standards of medical care in diabetes – 2009. Diabetes Care 2009; 32(S 1): S 13 -S 61, Poirier P, Cornier M-A, Mazzone T et al. Bariatric surgery and cardiovascular risk factors: A scientific statement from the American Heart Association. Circulation 2011; 123: 00 -00. International Diabetes Federation. Bariatric surgical and procedural interventions in the treatment of obese patients with type 2 diabetes. 2011. Handelsman Y, Mechanick JI, Blone L et al. American Association of Clinical Endocrinologists medical guidelines for clinical practice for developing a diabetes mellitus comprehensive plan. Endocr Prac 2011; 17(Suppl 2). page 2

Bariatric Procedures Roux-en-Y Gastric Bypass LAP-BAND

Improvements of Co-morbidities � Type 2 diabetes mellitus � Hypertension � Hyperlipidemia � Degenerative joint disease � Sleep apnea � GERD � 5% to 10% weight reduction is associated with significant decrease in risk � Weight loss from surgery reduces or eliminates medications � Improves severity or resolves co-morbid disease

Macronutrient Concerns �Protein �Carbohydrates �Fat

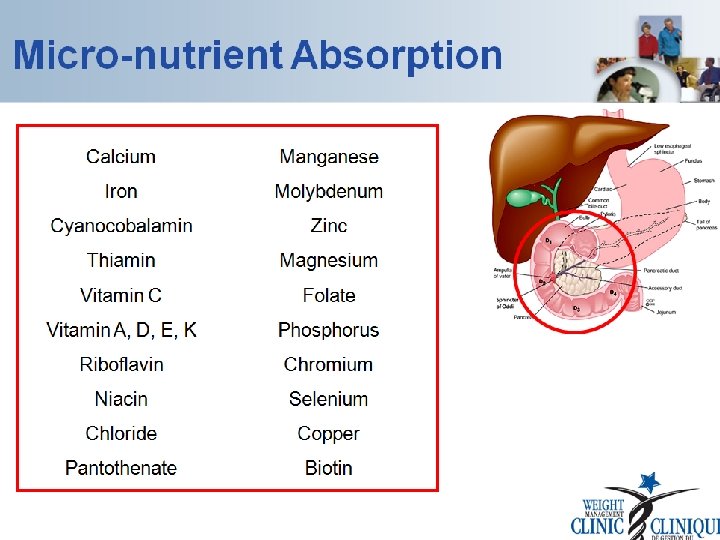
Micronutrient Concerns �Iron �Calcium and Vitamin D �Vitamin B 12 �Folic acid �Thiamin �Zinc

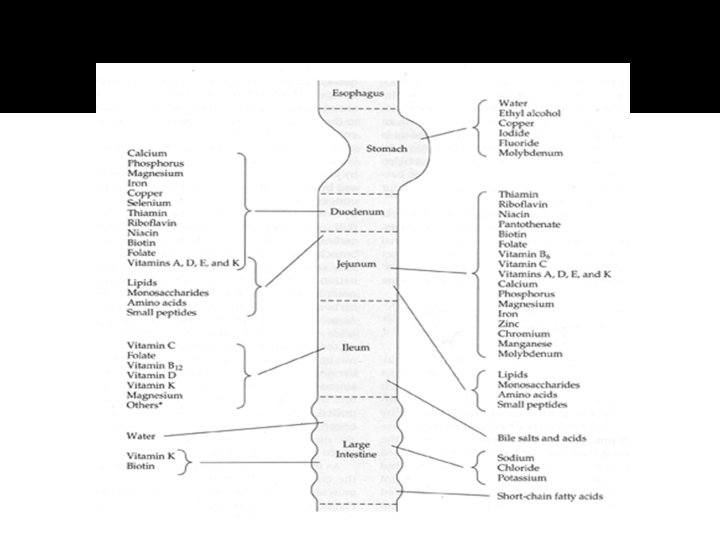
Sites of Nutrient Absorption �Stomach Water, ethyl alcohol, copper, iodide, fluoride, molybdemum, intrinsic factor �Duodenum Calcium, iron, phosphorus, magnesium, copper, selenium, thiamin, riboflavin, niacin, biotin, folate, vitamins A, D, E, K

Sites of Nutrient Absorption �Jejunum Thiamin, riboflavin, niacin, pantothenate, biotin, folate, vit B 6, vit C, vit A, D, E, K, dipeptides, tripeptides, calcium, phosphorus, magnesium, iron, zinc, chromium, manganese, molybdenum, amino acids �Ileum Vit C, folate, vit B 12, vit D, vit K, magnesium, bile salts/acids

Common Nutrient Deficiencies � Gastric Bypass: Most common: Iron, Vitamin B-12, Folic acid, Fat soluble Vitamins A, D, & E Thiamin (seen in patients with frequent vomiting) Calcium Protein malnutrition � Gastric Banding: Except for folate, nutrition deficiencies are less commonly seen post gastric banding � Sleeve Gastrectomy Possible B-12

Iron deficiency and anemia Common following RYGB As high as 49% of patients Multifactorial cause � � � � Low gastric acid levels prohibit iron cleavage from food Absorption inhibited because no nutrient exposure to duodenum or proximal jejunum Decrease in iron-rich food consumption due to intolerance Treat with oral supplementation of ferrous sulfate or ferrous gluconate

Ulcers, NSAIDs, �Patients with persistent iron loss should be evaluated for blood loss through the gastrointestinal tract. �Ulcers at the margin of the. �All NSAIDs, including aspirin have the potential to cause ulcers

Thiamin/Vitamin B 1 �Absorption of thiamin occurs primarily in the proximal small intestine �Thiamin deficiency after RYGB surgery can occur in up to 49% of patients �Thiamin deficiency mainly affects the central nervous system, potentially leading to beri and Wernicke encephalopathy which can develop into Wernicke-Korsakoff syndrome (WKS). �The classic triad of symptoms of WE involves ocular abnormalities, gait ataxia, and mental status changes

Niacin/Vitamin B 3 �Niacin/Vitamin B 3 Niacin deficiency after bariatric surgery is rare

Folate/Vitamin B 9 �Folate absorption occurs in the proximal portion of the small intestine, Complete absorption requires B 12 �Absorption dependent on HCl and upper 1/3 stomach �postoperative deficiency up to 40% patients �It is recommended that patients consume 200% of the daily value (800 mcg) of folic acid daily

Vitamin B 12 deficiency �Up to 70% of patients �Lack of hydrochloric acid and pepsin in stomach �Manifestation of vitamin B 12 deficiency is more likely to develop years after surgery due to the body’s B 12 reserve capacity. �Oral supplementation usually adequate, otherwise, IM injections used
")
�Recommended treatment for maintenance levels is 1000 mcg/d. �Several treatment options exist(daily, weekly, monthly) and method of intake (oral, intramuscular, nasal)

Malabsorptive bariatric surgery �Roen-en-Y gastric bypass: protein and fat malabsorption. . � Fat malabsorption manifests its presence by fat-soluble vitamins A, D, and K

�Vitamin D absorption occurs primarily in the distal small intestine. �a suggested dose is 50, 000 international units of ergocalciferol taken orally, once weekly, for 8– 12 weeks �recommended supplementing 3000 international units of vitamin D 3 daily

�Calcium absorption occurs mainly in the duodenum and proximal jejunum and is dependent on vitamin D levels �To support optimal bone health throughout weight loss, calcium supplementation should be given at 1200– 1500 mg/d along with regular consumption of calcium-rich foods.

Vitamin D and Calcium Deficiency � Vitamin D deficiency is common among obese people � Calcium absorption decreased because duodenum is bypassed � Intolerance to dairy, foods high in calcium � Vitamin D is required for Ca++ absorption � Prolonged deficiencies lead to Bone resorption, osteomalacia, osteoporosis

� Vitamin A : risk for vitamin A deficiency those with BPD and DS due to the limited available absorptive area and changes with fat absorption after surgery � recommended that 50, 000– 100, 000 international units of vitamin A be given intramuscularly for 3 days followed by 50, 000 international units per day intramuscularly for 2 weeks � Treatment for vitamin A deficiency without corneal changes is 10, 000– 25, 000 international units per day orally until clinical improvement is seen.

Specific signs and symptoms of common vitamin and mineral deficiencies �Calcium: bone pain �Iron: fatigue �Zinc: brittle nails �Vitamin A: inability to see in the dark �Vitamin E: poor wound healing �Vitamin K: easy bruising �Vitamin B 1 (Thiamin): numbness and tingling in the hands and feet �Vitamin B 12 (Methylcobalamin): fatigue

�” Due to fat malabsorption, severe vitamin D deficiency will develop along with an already reduced ability to absorb calcium �fractured bones �a bone density study “severe bone loss”

Hair loss �or telogen effluvium, is seen frequently 3– 6 months after surgery. �Lasting as long as 6– 12 months � it can be terribly distressing to the patient. �Although there is no known treatment, it usually reverses without intervention
 : Goal Female, 30– 160 mcg/d. L")
Laboratory Monitoring Schedule �Thiamin (vitamin. B 1) : Goal Female, 30– 160 mcg/d. L Male, 30– 300 mcg/d. L �Treatment: Confirm patient taking 2 MVIs daily (1 MVI LAGB) each containing 100% RDA thiamin. � � Parenteral supplementation 100 mg/d for 7. 14 d, then 50 mg/d until levels are normal or symptoms resolve � 500 mg/d IV thiamine should be given for severe deficiency, followed by 250 mg/d for 3. 6 d or until symptoms resolve
 : 200– 1000 pg/m. L �Confirm patient taking 2")
�Cobalamin (vitamin B 12 ) : 200– 1000 pg/m. L �Confirm patient taking 2 MVIs (1 MVI LAGB). � Confirm patient (except LAGB) is taking vitamin B 12 : up to 1000 mcg/d orally or 500 mcg/wk intranasally, or 1000 mcg/mo IM. �� œ If <200 pg/m. L -IM injections or supplement with 350. 1000 mcg/d orally. �

�Vitamin D, 25 -hydroxyvitamin D : >30 ng/m. L (insufficiency = 25– 30 ng/d. L) If <20 mg/m. L, • start ergocalciferol or cholecalciferol 50, 000 units/wk orally � ~ 8 wk. • maintenance dose of vitamin D 3, 3000 international units daily if level is persistently low • Supplementation for vitamin maintenance is recommended a 1000. 2000 i u per day

�Calcium and intact PTH Serum : �Ca: 9– 10. 5 mg/d. L Ionized Ca: 4. 5– 5. 6 mg/d. L i. PTH <65 pg/m. L � Confirm patient taking calcium citrate 1200. 1500 mg/d.

�Folic acid RBC folate: 280– 791 ng/ m. L Serum folate: 11– 57 mmol/L, 5. 3– 99 ng/m. L � Confirm patient taking 2 MVIs (1 MVI LAGB) daily with 400 mcg of folic acid. œ Supplement with 1000 mcg/d orally if serum levels are low, up to 5 mg/d possibly needed with severe malabsorption. (RBC folate is a more sensitive marker than serum folate, which reflects dietary intake). � Encourage consumption of folate-rich foods.

� Iron Serum : iron: 37– 170 mcg/ d. L � Confirm patient taking 2 MVIs each containing at least 18 mg of iron. � Menstruating women and those at risk of anemia may require additional supplementation. � � If oral iron therapy has failed to improve laboratory values, then refer to hematology for IV iron replacement. � After iron infusions, patients should be encouraged to continue with goal iron intake of 50. 100 mg/d to prolong period between infusions

�Vitamin K : PT: 10– 13 Seconds � Confirm patient taking 2 MVIs daily. � 1 mg/d vitamin K supplementation recommended when INR values are >1. 4. �

�Vitamin A Plasma retinol: 20– 80 mcg/d. L �Without corneal changes: 10, 000. 25, 000 international units of vitamin A per day orally until clinical improvement. �With corneal changes: 50, 000. 100, 000 international units of vitamin A IM for 3 d followed by 50, 000 international units per day IM for 2 wk.

�Zinc 0. 66– 1. 1 mcg/ m. L �Confirm patient taking 2 MVIs containing zinc.

�Copper : 0. 75– 1. 45 mcg/ m. L � Confirm patient taking 2 MVIs that provide at least 2 mg/d copper. � Patients should be referred to dietitian. �Ensure 1 mg copper for every 8. 15 mg of oral zinc intake.

Vitamin and Mineral Supplementation �Patients require lifelong vitamin and mineral supplementation �regimens following bariatric surgery. � Routine biochemical monitoring for nutrition status
 with vitamin D (1200 -1500 mg")
Recommended Daily Supplements �Multivitamin with iron �Calcium (citrate) with vitamin D (1200 -1500 mg calcium with 800 -1000 IU vitamin D) �Oral vitamin B 12 (500 -1000 mcg) �Iron (65 mg/day in elemental form) Vitamin C (to increase absorption of Iron) �Thiamin (10 mg/day)

Questions
- Slides: 39