Nutrition Ramona Sunderwirth MD MPH Global Health Fellowship

Nutrition Ramona Sunderwirth, MD MPH Global Health Fellowship, EM St Lukes/Roosevelt Hospital New York, NY

objectives General principles Specific nutrients Life cycle approach to nutrition Measures of malnutrition Severe malnutrition

Hunger is a term which has three meanings Uneasy or painful sensation caused by want of food; craving appetite, the exhausted condition caused by want of food Want or scarcity of food in a country A strong desire or craving World hunger refers to the second definition The related technical term is malnutrition. 1 Malnutrition is a general term that indicates a lack of some or all nutritional elements necessary for human health Underweight, Stunting, Wasting Obesity

Number of People Hungry in the world 2010 925 M

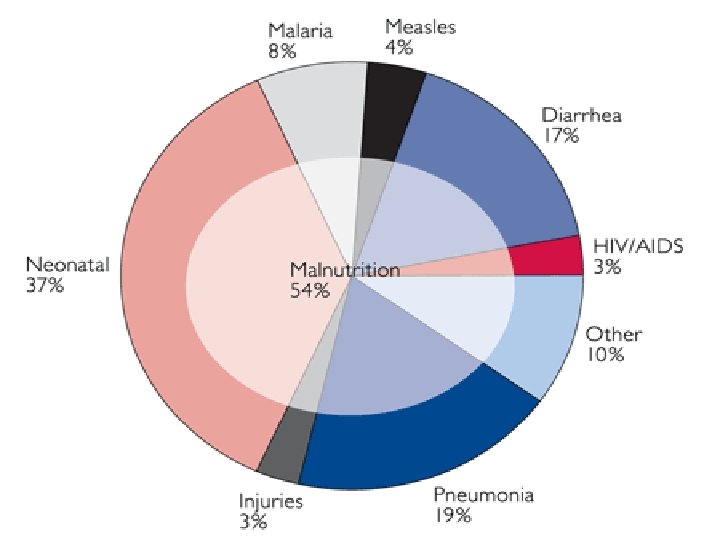
Major Causes of Death in Children Under Five in Developing Countries and the Contribution of Malnutrition

Causes of Hunger Poverty – principle cause Lack of resources, unequal distribution resources (Amartya Sen) Harmful economic systems → poverty & hunger control over resources & income based on military, political & economic power that typically ends up in the hands of a minority, who live well, while those at the bottom barely survive, or don’t Conflict → poverty & hunger Displaced: refugees & IDP Hunger → poverty → hunger poor health, ↓ levels of energy, mental impairment, ↓ ability to work & learn → greater hunger
 Lack")
Causes of Hunger, cont. Dietary practices Breastfeeding Single source diets (corn, rice, cassava) Lack of education/knowledge or access Agricultural productivity lack of farming skills , technology or resources (nitrogen, fertilizers, pesticides , irrigation) Climate change current & future cause of hunger & poverty ↑drought, flooding, changing climatic patterns requiring a shift in crops / farming practices not easily accomplished

Nutritional determinants of health among the most powerful environmental factors influencing health & disease Recommended nutrient intakes RDA now DRV (dietary reference values) Food based dietary guidelines Food pyramid Malnutrition modulates other diseases Infection Major contributor to death Immunity and malnutrition Immunity greatly compromised Barrier defenses breached, cell-mediated immunity depressed Lymph glands/thymus atrophic Ig. A, complement components , phagoycytic activity depressed Effects of less extreme malnutrition/nutrient deficiencies

Infection& Malnutrition: Vicious Cycle

Essential Nutrients Energy Drives consumption of all other nutrients Intake balanced w/ expenditures Deficit must be met by body stores Short term: muscles/liver glycogen/ short term fat stores Medium term: adipose tissue Long term: protein Wasting: sustained energy deficits Adults: Chronic Energy Deficiency CED (BMI < 18. 5) Famines/poverty Incorrect child feeding practices Anorexia of infection & illness
 Amylase, sucrase,")
Essential nutrients Carbohydrates Most energy in most diets (17. 6 k. J/g) Amylase, sucrase, maltase, lactase → glucose Glucose: used by tissues, stored in liver/muscle (glycogen) Insulin vs Cortisol/GH Brain consumes 60% of total circulating glucose Ketones used during starvation (B-hydroxybutyric acid from fats)

Clinically significant disturbances in carbohydrate metabolism Malabsorption Lactase deficiency, gut infections, Kwashiorkor, persistent gastroenteropathy Disturbed Metabolism: hypo. Glycemia Inadequate stores Marasmus, Kwashiorkor Liver damage, hepatitis Sepsis Toxins/drugs Alcohol, insulin Cerebral malaria Disturbed Metabolism: hyper. Glycemia Hormonal DM (insulin resistance) Excess corticosteroids
 (39 k. J/g) Saturated (animal) vs Unsaturated (plants) Long chain")
Essential nutrients Fats (TG) (39 k. J/g) Saturated (animal) vs Unsaturated (plants) Long chain PUFAs (breast milk) & EFAs (found only in food) In Times of Plenty: TG stored in adipose tissue (insulin) In Times of Negative Energy Balance: Noradrenaline & GH stimulate Lipase in adipocytes Fat deposits depleted EFA & TG oxidized in liver to acetoacetic acid (used for energy) EFA used directly by skeletal & heart muscle

Disturbances in Fat metabolism Inadequate stores Dietary Starvation, Marasmus Malabsorption Infections in Gut (giardia, strongyloides) Bile salt deficiency Obstructive Jaundice, Gall bladder disease, Bacterial overgrowth Pancreatic damage Kwashiorkor Pancreatitis Disturbed metabolism Fatty Liver Kwashiorkor Alcoholism
 Provides AA for synthesis: enzymes, plasma proteins, milk,")
Essential nutrients Proteins (17 k. J/g) Provides AA for synthesis: enzymes, plasma proteins, milk, tissue cells Starvation: AA → glucose (gluconeogenesis)>→decrease muscle mass/ damage to vital organs (Marasmus) Essential AA found in diet only Quality of dietary protein measured by animal growth Animal protein: first class protein, similar AA composition to humans Milk: high net protein utilization index (NPU=biological value (quality + digestibility) Plant protein: variable digestibility + quality plant mixtures can supplement each other (high quality proteins) Protein concentration in diets 5 -6% energy 6 -8%: infants, malnourished children, lactating women

Clinically important disturbances in protein metabolism Inadequate stores Inadequate synthesis Starvation Cirrhosis of liver Marasmus, Kwashiorkor Diabetes Malabsorption Pancreatic disease Kwashiorkor Increased catabolism Infections Tumours Increased loss Nephrotic syndrome Severe gut infections Measles, amoebiasis Bacillary dysentery Burns & exudates
 29 7")
Food component Energy Density k. J/g kcal/g Fat 37 9 Ethanol (alcohol) 29 7 Proteins 17 4 Carbohydrates 17 4 Organic acids 13 3 Polyols (sugar alcohols, sweeteners) 10 2. 4 Fiber 8 2

Essential Nutrients Minerals Contained in all tissues/fluids, mainly in bone Functions in co enzymes, hormones, vitamins Balanced diet provides adequate amounts Calcium/Iron: meat/fish/eggs/diary products Iodide, fluoride, selenium: uptake by plants from soil/rocks Potassium/magnesium: cardiac/renal diseases & Kwashiorkor/ chronic diarrhea Micronutrient Initiative (2002): eliminate “hidden hunger” – most damaging worldwide Iron, iodine deficiency , Vit A

Essential Nutrients Vitamins Minute amounts vital for life Not synthesized in body (except Vit D): obtained in diet Regulators of metabolic reactions Fat soluble: Vit A, D, E, K Water soluble: Vit C, B complex Deficiencies : Together in people on poor, monotonous diets Lack of dairy products (riboflavin); Vit A, Vit C (seasonal) Emergencies (famines), prisons Illness w/ suppressed food intake Cultural: women/infants kept indoors

Life cycle approach to nutrition Special needs at special times Phases are linked, and each affect next stage of development: continuous loop Cause & Effect “Fetal & infant origins of diseases” & “Thrifty phenotype” Inter generational cycle of malnutrition

Fetal Growth & nutritional needs of pregnant women Low birth weight Nutritional effects on fetal growth Nutritional needs of pregnancy Dietary supplements in pregnancy Lactation

Fetal growth & nutritional needs of pregnant women Low birth weight predictor of NN & post NN mortality Interventions that raise BW by 100 g have major impact on mortality Fetal growth influenced by many factors Woman’s size predictor of BW (S. Asia vs African SGA rates) Maternal wt gain in pregnancy : 1. 5 kg/mo ↑normal energy intake by 10% (remarkable maternal energy sparing mechanisms) Nutritional needs of pregnancy & dietary supplements Community-wide dietary supplementation of poor rural women can enhance BW (Gambia) HIV + women given micronutrient supplementation : ↓ SGA Interventions to prevent fetal growth retardation targeted at specific pop.

Lactation Nutritional requirements of infant > fetus Energy requirements lactation > pregnancy Highly “robust” process Needs to increase energy intake by 20 -25% If balanced diet, other nutrient needs met Water soluble vitamins, minerals (calcium) Maternal deficiencies reflected as low concentrations in milk Fat soluble vitamins Better buffered Protein, fat, carbohydrate composition very constant Supplementation: in extreme situations

Infant Nutrition Growth Causes of growth failure Severe forms of PEM Classifications: Gomez vs Wellcome Marasmus Kwashiorkor Breast-feeding Optimal duration of exclusive breast feeding Weaning foods

Infant Growth where food supplies insecure, diet low quality, infections frequent Breast-fed infants (3 -4 mos) Ideal food, adequate amount, protection from infection WHO recommends exclusive BF till 6 mos age Growth faltering Begins w/ weaning: low nutrient density, contaminated By 1 yr average WFA -2 Z score in many areas Africa If stunted as well as wasted, look better nourished Strongly associated w/ developmental deficits “Road to Health” charts Wasting: acute malnutrition Stunting: longer term deficit

Malnutrition WHO defines malnutrition as the cellular imbalance between the supply of nutrients & energy & the body’s demand for them to ensure growth, maintenance, & specific functions.

Protein energy malnutrition Pediatrics Wasting : acute malnutrition Rapid weight loss or failure to gain weight normally Stunting: chronic malnutrition Failure of linear growth Underweight: acute & chronic malnutrition occurs as a result of wasting, stunting, or both

Child Nutrition & Malnutrition

• Malnutrition Classifications Chronic Malnutrition → Stunting Eventually affects child’s body proportions → Wasting Gomez Classification: The child's wt compared to that of a nl child of the same age Useful for population screening & public health evaluations % of reference wt for age = [(patient wt) / (wt of nl child of same age)] Waterlow Classification: % wt for ht = [(wt of patient) / (wt of a nl child of the same ht)] % ht for age = [(ht of patient) / (ht of a nl child of the same age)]

Wellcome Classification evaluates the child for edema & with the Gomez Classification system Wt for Age (Gomez) 60 -80% <60% w/ Edema w/ out Edema Kwashiorkor Under nutrition Marasmic. Kwashiorkor Marasmus

Definitions of malnutrition. Classification Definition Grading Gomez Weight below % median WFA Mild (grade 1) Moderate (grade 2) Severe (grade 3) 75%– 90% WFA 60%– 74% WFA <60% WFA Waterlow z-scores (SD) below median WFH Mild Moderate Severe 80%– 90% WFH 70%– 80% WFH <70% WFH WHO (wasting) z-scores (SD) below median WFH Moderate Severe -3%</= z-score < -2 z-score < -3 WHO (stunting) z-scores (SD) below median HFA Moderate Severe -3%</= z-score < -2 z-score < -3 Kanawati MUAC divided by occipitofrontal head circumference Mild Moderate Severe <0. 31 <0. 28 <0. 25 Cole z-scores of BMI for age Grade 1 Grade 2 Grade 3 BMI for age z-score < -1 BMI for age z-score < -2 BMI for age z-score < -3

Classification of Malnutrition in Children Mild Malnutrition Moderate Malnutrition Severe Malnutrition 80 -90% 70 -79% < 70% Percent of Usual Body Weight 90 -95% 80 -89% Albumin (g/d. L) 2. 8 -3. 4 2. 1 -2. 7 < 2. 1 150 - 200 100 - 149 < 100 1200 - 2000 800 - 1199 < 800 Percent Ideal Body Weight Transferrin (mg/d. L) Total Lymphocyte Count (per µL) < 80%
 90 -110 75 -89")
Malnutrition Classifications Gomez- Public Health screenings & Emergencies WFA% (reference) 90 -110 75 -89 60 -74 <60 Classification Normal Grade I – Mild Grade II – Moderate Grade III - Severe Wellcome – Clinical Settings WFA% (NCHS median) 60 -80 < 60 No edema With edema Undernutrition Kwashiorkor Marasmus Marasmic/ Kwashiorkor

Methods of assessing growth failure & pediatric malnutrition Reference growth curves for Wt & Ht Road to Health: %WFA %HFA %WFH ( if age unknown) Expected wt/ht for age WHO curves in Africa Centile curves Same reference curves, 50% is line up center distribution Nl population Z-scores 1 SD from mean of Nl population (average WFH O Z-score) Applied to WFH, HFA, WFA MUAC: constant from 1 -5 yrs ag >140: Normal , 115 -140 mild/moderate, <115 severe Red-severe acute Orange -moderate acute Yellow refer Green- Nl HC, Skinfold thickness (triceps & supra-scapular)

Road to Health Chart

MUAC

Skin fold thickness

Causes of growth failure Infections Primary nutrient shortages-seasonal, famine, cultural, conflict Tropical gastroenteropathy Villous atrophy: degree predicts growth Affects nutrient absorption (lactose) Loss of plasma proteins: protein enteropathy (measles) Increased permeability Over active inflammatory response

Malnutrition in Children 25% world’s pediatric pop undernourished Contributes to > 50% U 5 Mortality in RPC Children very vulnerable to malnutrition High nutritional requirements for growth Reliance on others for food access Two classic phenotypic presentations PEM + micronutrient deficiencies Marasmus: decreased WFH + severe wasting Kwashiorkor: distinguished by edema Marasmic/Kwashiorkor : elements of both

Pathophysiology Tissue starvation influences physiology at every level Native & acquired immunity weakened Antioxidant deficiencies → unchecked free radicals to inflict direct cellular damage Injury to cell wall Na-K pumps → Na retention & K wasting Hypo. Glu: exhaustion of muscle glycogen stores & impaired gluconeogenesis Atrophy & oxidant induced damage of myocardial tissues → cardiac dysfunction + Fluid shifts from leaky membranes + large Na loads during recovery → CHF

Severe forms of Malnutrition Marasmus “adapted state”: prolonged underfeeding forces child to consume own fat/protein stores to maintain function vital organs 1 st yr of life, WFA & HFA diminished Thin, severe muscle wasting, weak Sunken eyes, dry mucous membranes, skin tenting, decreased tears : not to be confused w/ dehydration Bradycardia, hypo TA & hypothermia Thin, dry skin, redundant skin fold. Thin, sparse hair, easily plucked

Severe Forms of Malnutrition Kwashiorkor “Disadapted state”, imbalance in protein supply limits hepatic production albumin & plasma proteins → edema 2 nd year of life. Acute illness Marked muscle atrophy, w/ nl body fat. Anorexia. Apathetic, irritable Pitting edema, anasarca, “Moon Face” Dry, atrophic, peeling skin, confluent areas of hyperkeratosis & hyper pigmentation: Flaky paint dermatosis Dry, dull, hypopigmented hair, orange, falls out/easily plucked Hepatomegaly (fatty liver infiltrates)+ dilated/hypomotile intestinal loops + bacterial overgrowth/gas production, weak abd muscles → distended abdomen

Kwashiorkor & Marasmus

Kwashiorkor & Marasmus

Childhood & adolescence Higher metabolism rate /energy/nutrient requirements than adults Adolescent growth spurt energy, protein, Ca & Iron requirements raise Same diet as Adults Often fed last, after Men, Women & younger children

Treatment of Malnutrition For another Thursday
- Slides: 47