Nutrition in Sick Patients n n n Why










































- Slides: 50
Nutrition in Sick Patients n n n Why it is important? What is the evidence? How to treat and prevent malnutrition Which route to choose What sort of tubes are there? Calculations and refeeding syndrome
‘A slender and restricted diet is always dangerous in chronic and in acute diseases’ Hippocrates 400 B. C.
‘Do not let your patients starve and when you offer them nutrition support, do so by the safest, simplest, most effective route. ’ Dr Mike Stroud Feb 2006 Chair of NICE committee
Why is it important? n n n Mc. Whirter and Pennington 1994: 40% of hospital patients malnourished on admission and nutritional state usually deteriorates in hospital. Costs £ 3. 8 bn/yr Critically ill are often malnourished: admitted after major surgery, following extended illness or hospital stay, high rate of alcohol/drug misuse, poor self care, elderly, co-existing disease etc
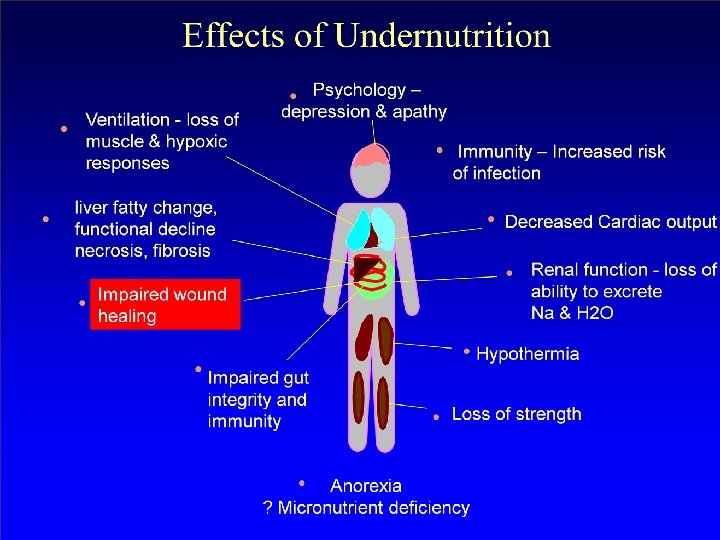
Effects of malnutrition
Nutritional State and Complications HDU
Metabolic response to starvation § § § Aims to minimize impact on vital organs and conserve energy Reduction in tissue metabolism Decreased metabolic rate Decreased temperature Reduction in physical activity Protein loss
Starvation n n n Bobby Sands – lost 7 kg in first 17 days Approx 0. 5 kg/day Died at 65 days (9 weeks) Not expending excess energy, not in ICU patients – often have increased metabolic demands AND starvation Complex metabolic changes
Critical illness: Metabolic demand n n n n n sympathetic nervous system stimulation acute phase response: cytokines severe catabolism organ failure, poor gut function increased oxygen requirements poor wound healing insulin resistance: hyperglycaemia Wasting iatrogenic problems – drugs/HAI
Starvation and ICU n n n Complex metabolic changes Weight loss is high if sick patients are not fed But nutrients are not always adequately absorbed or metabolised Weight loss occurs despite feeding Important to feed patients but with regard to their individual needs and complexities.
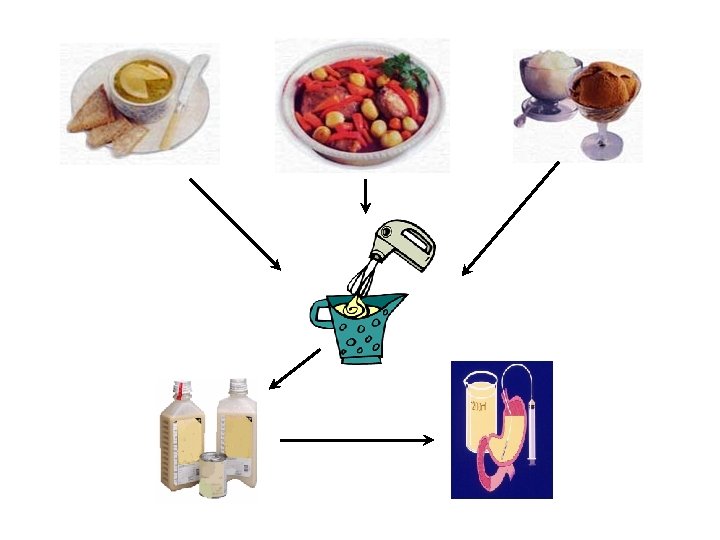
ICU nutrition n Used to be everything mixed up and given via NG tube Risk of infection Now specialised feeds are used in sterile packaging
What is the evidence in HDU? n n n n Early nutrition is important Bowel function may recover within 12 hours Use the gut if you can Bowel sounds are not a good indication of bowel function Ileus is common Giving pre-op sugary drinks can speed bowel function (ERAS) Use EN + TPN to achieve goals
How do we treat/prevent malnutrition? n Whose role is it?
How do we treat/prevent malnutrition? Think about it n Identify it – history – weight loss, intake, vomiting, diarrhoea, IBD, cancer etc: doctors and nurses n Weight- nurses n Optimise intake – oral/enteral/parenteral: doctors/dietitians/nurses Monitor – nurses/dietitians/doctors n
Organisation of Nutrition Support Screen Recognise Treat Oral Enteral Monitor & Review 3. NICE Guidelines for Nutrition Support in Adults 2006 Parenteral
Step 1: Screen MUST Malnutrition Universal Screening Tool MUST from BAPEN n BMI score, n weight loss score, n acute disease effect score together gives low, medium and high risk of malnutrition: if high, patient must be treated early
At risk of malnutrition n n Eaten little or nothing for 5 days and unlikely to do so for at least next 5 days Poor absorptive capacity and/or high nutrient losses and/or increased nutritional needs due to catabolism etc Patient at risk of becoming malnourished 3. NICE Guidelines for Nutrition Support in Adults 2006
Malnourished n n n BMI less than 18. 5 Kg/m 2 Weight loss > 10% within last 3 -6 months BMI < 20 Kg/m 2 and unintentional weight loss > 5% in last 3 -6 months Patient already malnourished 3. NICE Guidelines for Nutrition Support in Adults 2006
Weighing Patients n Important for nutrition screening/dosage Drug dosages Cardiac output monitoring Fluid balance CT scanning n Estimation? n n
Routes: Enteral n n Preserves intestinal mucosal structure and function More physiological Reduced risk of infectious complications £ 6 vs £ 66
Routes Of feeding
Naso-gastric Feeding n n n Risk of aspiration in ICU: HOB 30 degrees Don’t start feed at night Risk of displacement High aspirates and inadequate calories common in ICU PEG/gastrostomy feeding for long-term
Jejunal Feeding n n n Jejunal feed: via a tube placed Trans-nasally by endoscopy, radiologically, at the bedside. Into the jejunum either at laparotomy or laparoscopy May reduce incidence of aspiration Often increases dose of EN given over NG
Why do we use TPN?
Parenteral Nutrition n n GI tract is not functional GI tract cannot be accessed Inadequate GI feeding: Optimise enteral first if possible; if not absorbing start TPN on day 3 -7 depending on nutritional state
TPN n n n n Doctors decide patient needs it Dietitian sees patient Decides best regime Orders bag from pharmacy Made up aseptically to requirements Start low and build up Monitor bloods
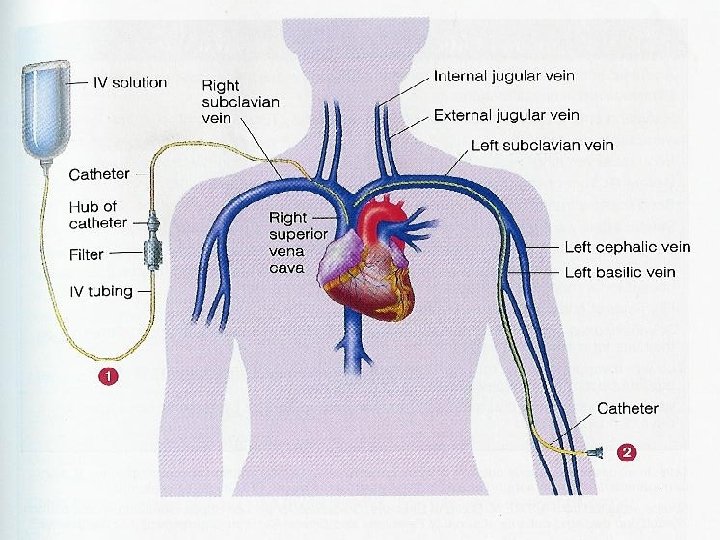
Access for PN n n n Usually central line in ICU – keep a clean port if PN may be needed. 5 lumen Short term PN – can have PIC (need a different formula) or PICC Long-term TPN – tunnelled subclavian catheter (Hickman) or subcutaneous port is usually inserted – OBSERVE STRICT ASEPSIS if handling these lines.
Tubes and Lines
Complications Constipation n Diarrhoea – important points? n Intolerance: ? Sepsis Use pro-kinetics, NJ feeding, drugs n Line sepsis n Ileus – Avoid opioids, optimise fluid balance and electrolytes, ? trickle of feed n n
Overfeeding n n n Lactic acidosis Hyperglycaemia Increased infections Liver impairment (Alk phos, ALT, GGT, acalculous cholecystitis) Persistent pyrexia
How much to give – general recommendations n n n Prescription calculated by dietitian Schofield equation e. g. for 60 -74 year old woman: BMR = (9. 2 x weight in kg) + 687, (tables available)=requirement in Kcal/24 hr Add Activity factor and stress factor e. g. 10% for bedbound + 20 -60% for sepsis – burns i. e for 65 kg woman ventilated woman with sepsis this works out as 1670 Kcal = approx 25 Kcal/kg/24 hr Rough guide to start: 25 Kcal/kg/day total energy. Increase to 30 as patient improves
How much to give – general recommendations n n n 1. 25 g/kg/day protein more just gets excreted 30 ml fluid/kg/24 hours. Add 100 -200 ml/day for each degree of temperature Account for excess losses Adequate electrolytes, micronutrients etc Avoid overfeeding Obesity: feed to BMR no stress factor unless stress is severe e. g. burns/trauma
Refeeding Syndrome n n 1944 conscientious objectors/concentration camps – CCF when fed Starvation 1 st 24 -72 hours – body uses glycogen stores for gluconeogenesis, 72+ hours – FFA oxidation to ketones, sparing protein. Feeding – metabolism shifts back to glucose – ATP and 2 -3 DPG produced. Phosphate drops and K and Mg shift into cells due to anabolism and insulin release. Extra-cellular fluid expansion and thiamine B 1 deficiency occur (co-factor in CH metabolism).
Refeeding Syndrome n n Unlikely to be a clear diagnosis Contributes to fluid imbalances, arrhythmias, muscle weakness, failure to wean, cardiac failure Awareness of the possibility is important: nutritional history and electrolytes Remember in HDU patients too – may not be fed for a long time
Risk of re-feeding syndrome n n One or more of the following: BMI less than 16 kg/m 2 unintentional weight loss greater than 15% within the last 3 -6 months little or no nutritional intake for more than 10 days Very low levels of potassium, phosphate or magnesium prior to feeding NICE Guidelines for Nutrition Support in Adults 2006
Risk of re-feeding syndrome Two or more of the following: n BMI less than 18. 5 kg/m 2 n unintentional weight loss greater than 10% within the last 3 -6 months n little or no nutritional intake for more than 5 days n a history of alcohol abuse or drugs including insulin, chemotherapy, antacids or diuretics
Managing refeeding problems n n n start nutrition support at 10 kcal/kg/day maximum increase levels slowly restore circulatory volume and monitor fluid balance and clinical status provide multivitamin/trace element supplementation: Pabrinex (B 1, B 2, C) o. d. or thiamine B 1 +Vigranon B before feed provide extra Phosphate, K+ and Mg 2+ NICE Guidelines for Nutrition Support in Adults 2006
Complex nutrition: Monitoring n n n n U & Es, phosphate, calcium, magnesium Glucose LFTs Fluid balance Haematology Weight Trace elements if long-term
Conclusion n n n Do not forget about feeding Keep an eye on whether nutritional targets are being met Speak to the surgeons and dietitian Remember refeeding syndrome Do not be reluctant to start PN in a supplemental capacity Avoid hyperglycaemia Nutrition is often neglected