Nutrition By MBBSPPT COM Nutritions are constituents in

Nutrition By MBBSPPT. COM

• Nutritions are constituents in the food which should be supplied in adequate amt. for optimal growth. Classifications: üMacronutrients - need in large amt. by the body. • Carbohydrates • Proteins • Fats üMicronutients – need in small amt. • Vitamins & minerals

On basis of function • Energy yielding foods- carb. & fats • Bodybuilding foods- proteins • Protective foods- vit. & minerals Recommended daily allowance (RDA)- nutrient intake considered adequate to meet the known nutrient needs of practically all healthy children in a particular age.

Holliday- Segar formula for calculating the daily requirement of calories Wt. in kg Daily req. of calories ( kcal/kg) < 10 10 - 20 1000 + 50 > 20 1500 + 20 ICMR recommendations Age Calories (kcal/kg/d) Protein (g/kg/d) 0 -3 mo 120 2. 2 4 -6 mo 115 1. 8 6 -9 mo 110 1. 8 9 -12 mo 105 1. 5 1 yr 100 1. 5 2 -3 yrs 120 1. 4 4 -6 yrs 80 -90 1. 3 7 -9 yrs 70 - 80 1. 2 10 -12 yrs 60 -70 1. 2

Carbohydrates – 55% of total calorie • Monosaccharides- glucose, fructose, galactose • Disaccharides- lactose, maltose, sucrose • Polysaccharides- starch, dextrins, glycogen, pectin Glycaemic index – effect of carb. on the blood glucose levels. • High GI- raise blood glucose rapidly • Low GI – raise blood glucose slowly hence less fluctuation on insulin Dietary fibres- non starch polysaccharides. , donot have any calories value, help in digestion. Eg- cellulose, lignins, pectins etc

Proteins – 20 aminoacids • 12 non essential a. a • 8 essential a. a Biological value (BV)- fraction of retained nitrogen compared to the absorbed nitrogen. • BV= retained nitrogen/ absorbed nitrogen X 100 Protein efficiency ratio ( PER)- define a the gain in wt. per unit wt. of prot. consumed over a pd. of time.

BV of various protein Source of prot. BV Egg 96 -100 Cow milk 90 Rice 77 Fish 75 Meat 74 Wheat 66 Bengal gram 74 PER Source of prot. PER Egg 3. 8 Fish 3. 5 Meat 3. 2 Cow milk 2. 8 Rice 1. 7 Wheat 1. 3 Bengal gram 1. 1
 –amt. of absorbed nitrogen compared to nitrogen present in the food")
Digestibility Coefficient (DC) –amt. of absorbed nitrogen compared to nitrogen present in the food • DC= absorbed nitrogen/ food nitrogen X 100 Net prot. Utilization (NPU) – amt. of retained nitrogen to the nitrogen present in the food item. It the product of BV & DC • NPU= retained nitrogen/ food nitrogen X 100 • NPU= BV X DC

NPU Source of Prot. NPU Egg 96 Cow milk 85 Rice 77 Meat 76 Fish 74 Bengal gram 61 Wheat 61

• Fatty acids- saturated , monounsaturated, polyunsaturated. Source – • Animal source-ghee, butter, egg yolk, cheese etc • Plant – mustared oil, nuts, vegetable oils • EFA- is a polyunsaturated fatty acid need in the diet. Eg- omega-6 ( linoleic acid), omega— 3 ( linolenic acid). • EFA – 3% of total energy requirement of the child.
 Oil Total EFA Linoleic Linolenic Safflower")
EFA in various edible oils ( g/100 g) Oil Total EFA Linoleic Linolenic Safflower 74. 5 74 0. 5 Soya bean 57 52 5 Sunflower 52 52 trace Ground nut 28. 3 28 0. 3 Coconut 2. 2 nil Ghee 2. 1 1. 6 0. 5
 • Fat- 30%- 35%")
Balanced diet • Carb. - 55%- 60% (1 g=4 kcal) • Fat- 30%- 35% (1 g=9 kcal) • Protein- 10%-15% (1 g=4 kcal) • Ratio of prot. derived from cereals to pulse should be 4: 1 • Minimum level of leafy & other vegetables should not be less than 150 g/day • Cereal – defecient of lysine, threonine , tryptophan. • Pulses rich in lysine & defecient in methionine

Calorie & protein content of common food Food category Food stuff Amount Calorie ( kcal) Protein (g) Cereals Rice 100 g 325 7. 5 Wheat 100 g 341 12. 1 Maize 100 g 340 11 Barley 100 g 335 9 -11 cornflour 100 g 360 8. 6 Bread (white) 1 slice 50 -70 2 Dhal 100 g 372 P 21, C 60 Soya bean 100 g 432 43. 2 Bengal gram 100 g 360 17 Green gram 100 g 340 24 Red gram 100 g 335 22. 5 Black dhal 100 g 347 P 24, C 55 Breast milk 100 ml 65 1. 1 Cow milk 100 ml 70 3. 5 butter 100 g 730 0 Veg oil 100 g 900 0 Pulses Milk & milk products Fats & oil
 Protein (g) Nut Coconut 100 g")
Food category Food stuff Amount Calorie ( kcal) Protein (g) Nut Coconut 100 g 444 4. 5 Almond 100 g 655 20 Ground nut 100 g 560 27 Egg 1 66 -80 6 Mutton 100 g 194 18. 5 Chicken 100 g 300 18 Liver (goat) 100 g 107 20 Beef 100 g 400 8 pork 100 g 114 18. 7 Fish 100 g 100 -300 20 -60 1 tsf 16. 0 C-4. 2, F-0, P-0 100 g 346 22 Meat & poultry Sugar Rajma C-60, F-1. 3

Malnutrition Indicators • Wt/age • Ht. /age • Wt. / ht Calculation & interpretation- Wt. for age= wt. of the child/ wt. of normal child of same age X 100 Indicator Acute malnutrition Chr. malnutrition W/A (underweight) low H/A( stunting) N low W/H ( wasting) low N

Protein Energy Malnutrition Iceberg
 Normal >80 Grade I PEM")
Classification IAP Classification: Nutrition status Wt. for age (%) Normal >80 Grade I PEM 71 -80 Grade II PEM 61 -70 Grade III PEM 51 -60 Grade IV PEM <50 Welcome Trust Classification Wt. for age Odema present Odema absent 60 %- 80% kwashiorkor undernutrition < 60% Marasmic kwashiorkor marasmus
")
Gomez Classification Nutritional status Wt. for age Normal >90 I degree PEM ( mild) 76 -90 II degree PEM ( moderate) 60 -75 III degree ( severe) <60 WHO Classification parameter Moderate undernutrition Severe undernutrition Symmetrical odema Absent Present Wt. for ht. Z score or SD score between -2 & -3 Z score or SD score between < -3 Ht. for age Z score or SD score between -2 & -3 Z score or SD score between < -3
 Classification Ht. for age (%) Normal >95 First")
Waterlow classification ( Ht. for age) Classification Ht. for age (%) Normal >95 First degree stunting 90 -95 Second degree stunting 85 -89 Third degree stunting <85 Waterlow classification ( Wt. for Ht. ) Classification Ht. for age (%) Normal >90 Mild wasting 80 -90 Moderate wasting 70 -79 Severe wasting <70
 • Bangle test, Shakir’s tape üSkinfold")
Age independent criteria üMidarm circumference (1 -5 yr) • Bangle test, Shakir’s tape üSkinfold thickness (1 -6 yr)- biceps, triceps, infrascapular, suprailiac Harpenden caliper >10 mm- normal <6 mm- abnormal üKanawati index= MAC( cm)/ head circumference (cm) üRao & Singh’s index= wt. (kg)/ (ht. in cm)² X 100 üDugdale’s index= wt. in kg/ (ht. in cm)₁∙₆ X 100 üPonderal index= wt in g X 100/ ht. in cm₃ üBMI= wt. in kg/ (ht. in m )²

Kwashiorkor

Clinical Manifestations: q Diagnostic Signs ü Edema ü Muscle wasting ü Psychomotor changes q Common Signs ü Hair changes ü Diffuse depigmentation of skin ü Moonface ü Anemia q q q ü ü Occasional Signs: ü Flaky-paint rash ü Noma ü Hepatomegaly Laboratory: Decreased serum albumin EEG abnomalities Iron & folic acid deficiencies Liver biopsy fatty or fibrosis may occur

Noma Flaky-paint rash

Marasmus

Clinical Manifestations: 1. Wasting 2. Muscle wasting 3. Growth retardation 4. Mental changes 5. No edema 6. Variable-subnormal temp, slow PR, good appetite, often w/diarrhea, etc. Laboratory Data: 1. Serum albumin N 2. Urinary urea/ crea N 3. Serum essential a. a. index N 4. Anemia uncommon 5. K+ deficiency present 6. Serum cholesterol low 7. Diminished enzyme activity 8. Bone growth delayed 9. Liver biopsy N or atrophic

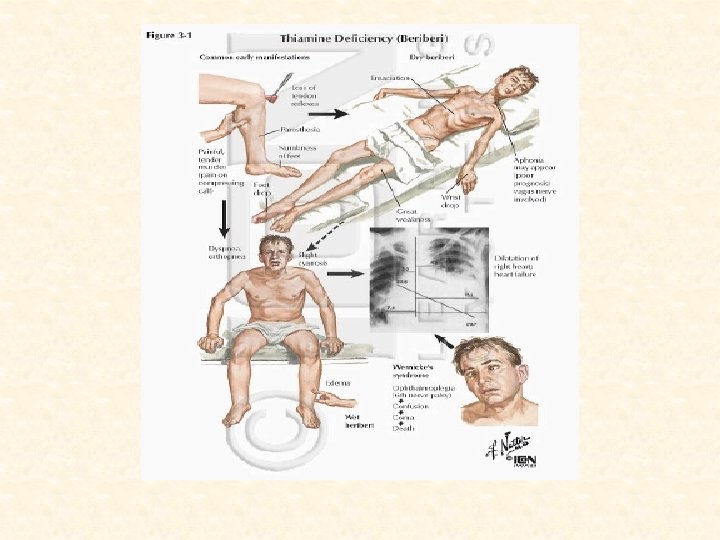
Thiamine, Riboflavin, Niacin, Pyridoxine are cofactors to enzymes in energy metabolism, hence, deficiencies show up in quickly growing tissues such as epithelium. Typical symptoms for the group include: üDermatitis üGlossitis üCheilitis üDiarrhea Nerve cells use lots of energy, so symptoms also show up in the nervous tissue: ü Peripheral neuropathy ü Depression ü Mental confusion ü Lack of motor coordination ü Malaise
 Deficiency Beriberi Three forms: 1. Wet beri: generalized edema, acute")
Thiamine (Vitamin B 1) Deficiency Beriberi Three forms: 1. Wet beri: generalized edema, acute cardiac symptoms and prompt response to thiamine administration 2. Dry beri: edema not present, condition similar to peripheral neuritis w/ neurological disorders present 3. Infantile beri divided into: a. Acute cardiac - ages 2 -4 months; sudden onset of cardiac such as cyanosis, dyspnea, systolic murmur & pulmonary edema w/ rales b. Aphonic - ages 5 -7 months; insidious onset of hoarseness, dysphonia or aphonia c. Pseudomeningeal - ages 8 -10 months; signs of meningeal irritation apathy, drowsiness & even unconsciousness. Treatment: 1. Children: 10 mg p. o. daily for several weeks 2. Adults 50 mg
 Deficiency Functions: 1. Acts as coenzyme of flavoprotein important in")
Riboflavin (Vitamin B 2) Deficiency Functions: 1. Acts as coenzyme of flavoprotein important in a. a. , f. a. & CHO metabolism & cellular respiration 2. Needed also by retinal eye pigments for light adaptation Clinical Manifestations: 1. Characteristic lesions of the lips, the most common of which are angular stomatitis and cheilosis 2. Localized seborrheic dermatitis of the face may result such as nasolabial seborrhea or dyssebacia and angular palpebritis 3. Scrotal or vulvar dermatosis may also occur 4. Ocular s/sx are photophobia, blurred vision, itching of the eyes, lacrimation & corneal vascularization Treatment: 1. Riboflavin 2 -5 mg p. o. daily w/ increased B complex 2. Parenteral administration if relief not obtained

Riboflavin Deficiency
 Deficiency Pellagra Etiology: 1. Diets low in niacin &/or tryptophan")
Niacin (Vitamin B 3) Deficiency Pellagra Etiology: 1. Diets low in niacin &/or tryptophan 2. Amino acid imbalance or as a result of malabsorption 3. Excessive corn consumption Clinical Manifestations: 1. Start w/ anorexia, weakness, irritability, numbness & dizziness 2. Classical triad of dermatitis, diarrhea & dementia 3. Dermatitis may develop insidiously to sunlight or heat a. First appears as symmetrical erythema b. Followed by drying, scaling & pigmentation w/ vesicles & bullae at times c. Predilection for back of hands, wrists, forearms (pellagrous glove), neck (Casal’s necklace) & lower legs (pellagrous boot) 4. GIT s/sx are diarrhea, stomatitis or glossitis; feces pale, foul milky, soapy or at times steatorrheic 5. Mental changes include depression, irritability, disorientation, insomnia & delirium

Treatment Niacin 50 -300 mg daily which may be taken for a long time Skin lesions may be covered w/ soothing lotions
 Deficiency Functions: 1. Vitamin B 6 is involved in the")
Pyridoxine (Vitamin B 6) Deficiency Functions: 1. Vitamin B 6 is involved in the synthesis and catabolism of amino acids, synthesis of neurotransmitters, porphyrins and niacin 2. Plays important role in clinical conditions such as anemia, hyperemesis gravidarum, cardiac decompensation, radiation effects, skin grafting, INH therapy & seborrheic dermatitis Etiology: 1. Losses from refining, processing, cooking & storing 2. Malabsorptive diseases such as celiac disease may contribute 3. Direct antagonism might occur between INH & pyridoxal phosphate at the apoenzyme level

Clinical Manifestations: 1. Three different types a. Neuropathic, due to insufficient neurotransmitter synthesis, such as irritability, depression & somnolence b. Pellagrous, due to low endogenous niacin synthesis, such as seborrheic dermatitis, intertrigo, angular stomatitis & glossitis c. Anemic, due to low porphyrin synthesis, such as microcytic anemia & lymphopenia 2. In genetic diseases involving pyridoxal phosphate enzymes also xanthurenic aciduria, cystathioninuria & homocystinuria Treatment: 1. Pyridoxine 100 mg IM injection for seizures due to deficiency 2. Children w/ pyridoxine dependency should be given 2 -10 mg IM injection or 10 -100 mg oral vitamin B 6
 Deficiency Functions: 1. Needed for RBC & DNA formation,")
Folic Acid (Vitamin B 9) Deficiency Functions: 1. Needed for RBC & DNA formation, cell multiplication esp. GI cells 2. Newly discovered functions: a. Prevents neural tube defects b. Prevents heart disease (reduces homocysteine levels) c. Prevents colon cancer Etiology: üPeak incidence 4 -7 months üDeficient dietary intake: goat’s milk deficient & powdered milk poor source ü Deficient absorption as in celiac disease, achlorhydria, anticonvulsant drugs, zinc deficiency & bacterial overgrowth ü Impaired metabolism w/ ascorbic acid deficiency, hypothyroidism, drugs like trimethoprim & alcoholism ü Increased requirement during rapid growth & infection ü Increased excretion/loss may occur subsequent to vitamin B 12 deficiency & chronic alcoholism ü Increased destruction possible in cigarette smoking

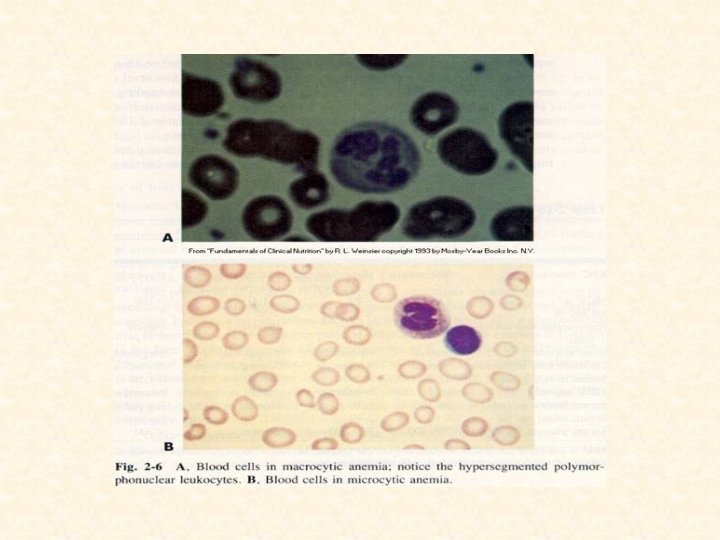
Clinical Manifestations: 1. Megaloblastic anemia w/ irritability, failure to gain wt & chronic diarrhea 2. Thrombocytopenic hemorrhages advanced cases 3. Scurvy may be present Laboratory Findings: 1. Anemia macrocytic 2. Serum folic acid <3 ng/ml, normal level=5 -20 ng/ml 3. RBC folate levels indicator of chronic deficiency, normal level=150 -600 ng/ml 4. Serum iron & vitamin B 12 normal or elevated 6. Formiminoglutamic acid in urine esp after oral histidine 7. Serum LDH markedly high 8. Bone marrow hypercellular RDA: 20 -50 mcg/24 hrs Treatment: 1. Parenteral folic acid 2 -5 mg/24 hrs, response in 72 hrs, therapy for 3 -4 wks 2. Transfusions only when anemia severe 3. Satisfactory responses even w/ low doses of 50 mcg/24 hrs, have no effect on primary vitamin B 12 deficiency 4. If pernicious anemia present, prolonged use of folic acid should be avoided
 Deficiency Absorption: Vitamin B 12 + glycoprotein (intrinsic factor) from")
Cobalamine (Vitamin B 12) Deficiency Absorption: Vitamin B 12 + glycoprotein (intrinsic factor) from parietal cells of gastric fundus terminal ileum absorption + intrinsic factor + Ca++ blood Function: Needed in reactions affecting production of methyl groups Etiology: ü Congenital Pernicious Anemia: Lack of secretion of intrinsic factor by stomach manifest at 9 months-10 years as uterine stores become exhausted ü Inadequate intake or dietary deficiency rare 1. Strict vegetarian diet 2. Not commonly seen in kwashiorkor or marasmus 3. Breast-fed infants whose mothers had deficient diets or pernicious anemia ü Consumption or inhibition of the B 12 -intrinsic factor complex ü Vitamin B 12 malabsorption from disease of ileal receptor sites or other intestinal causes

Clinical Manifestations: 1. Megaloblastic anemia that becomes severe 2. Neurological includes ataxia, paresthesias, hyporeflexia, Babinski responses, clonus & coma 3. Tongue smooth, red & painful Laboratory Findings: 1. Anemia macrocytic 2. Serum vitamin B 12 <100 pg/ml but serum iron & folic acid normal or elevated 3. Serum LDH activity markedly increased 4. Urinary excess of methylmalonic acid, a reliable & sensitive index RDA: Infants 0. 5 mcg/day Older children & adults 3 mcg/day Treatment: 1. Prompt hematological response w/ parenteral vitamin B 12 1 -5 mcg/24 hrs 2. If there is neurological involvement 1 mg IM daily for at least 2 wks 3. Pernicious Anemia: Monthly vitamin B 12 1 mg IM necessary throughout patient’s life
 Deficiency Scurvy Functions: 1. Collagen is the major connective tissue")
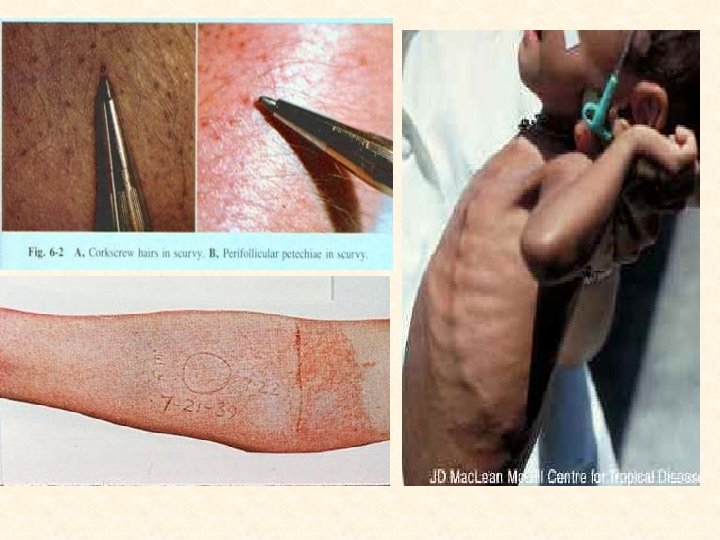
Ascorbic Acid (Vitamin C) Deficiency Scurvy Functions: 1. Collagen is the major connective tissue in the body & hydroxyproline, found only in collagen, is formed from proline requiring ascorbic acid 2. If there is defective collagen formation, endochondral bone formation stops , intercellular substance is no longer formed 3. Vitamin C is involved in hydroxylation reactions in the synthesis of steroids and epinephrine 4. Ascorbic acid also aids iron absorption by reducing it to ferrous state in the stomach, spares vitamin A, vitamin E and some B vitamins by protecting them from oxidation, and enhances the utilization of folic acid by aiding the conversion of folate to tetrahydrofolate Etiology: ü More common 6 -24 months ü May develop in breastfed infant if mother’s diet deficient ü Improper cooking practices produce significant nutrient losses & faulty dietary habits

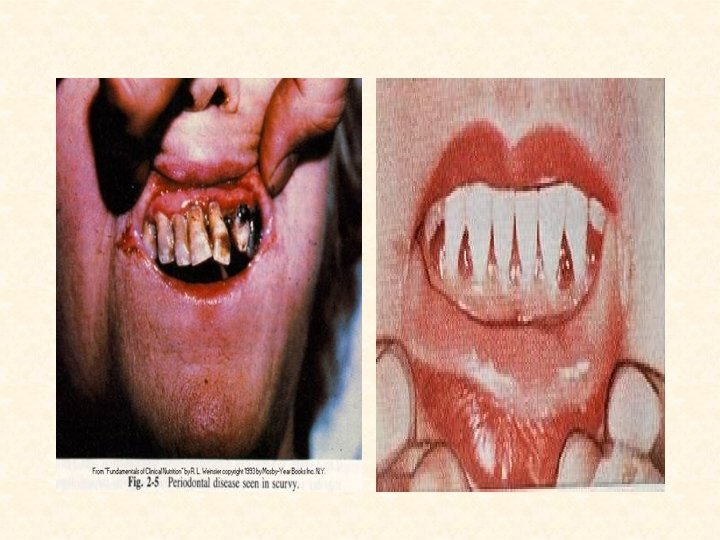
Clinical Manifestations: 1. 2. 3. 4. 5. 6. 7. 8. Early stages are vague symptoms of irritability, digestive disturbances & anorexia Mild vitamin C deficiency signs include ecchymoses, corkscrew hairs and the formation of petechiae due to increased capillary fragility resulting from weakened collagen fibrils Severe deficiency results in decreased wound healing, osteoporosis, hemorrhaging, bleeding into the skin and friable bleeding gums with loosened teeth A presenting feature is an infant w/ painful, immobile legs (pseudoparalysis), edematous in “frog position” & occasionally w/ mass There is depression of sternum “rosary of scorbutic beads at the costochondral junction due to subluxation of the sternal plate Orbital or subdural hemorrhages, melena & hematuria may be found Low grade fever & anemia usually present Impairment of growth & development

Diagnosis: 1. 2. 3. 4. History of vitamin C-deficient diet Clinical picture Therapeutic test X-ray findings in the long bones: a. Most prominent & early change is simple knee atrophy b. Shaft trabeculae cannot be distinguished giving “ground glass appearance” c. Cortex reduced to “pencil-point thinness” d. Zone of well-calcified cartilage, white line of Fraenkel, seen as irregular & thickened white line w/c e. Zone of rarefaction, a linear break in bone proximal & parallel to white line under at metaphysis f. Calcifying subperiosteal hemorrhages cause bone to assume a dumbbell or club shape

Differential Diagnosis: 1. Bleeding, swollen gums: Chronic gingivitis & pyorrhea w/ pus & respond to good dental hygiene 2. Pseudoparalysis: Syphilis negative x-ray; Poliomyelitis absent tenderness of extremities 3. Tenderness of limbs: RF age >2 yrs; Suppurative arthritis & osteomyelitis positive blood cultures 4. Bleeding manifestations: Blood dyscracias positive blood exams 5. “Rosary of scorbutic beads”: Rickets

Prognosis: 1. Recovery rapid w/ adequate treatment & permanent deformity rare 2. Pain ceases in a few days but swelling caused by subperiosteal hemorrhages may last several months Prevention : 1. A minimum daily intake of 30 mg is recommended by WHO for all age levels. 2. Every infant should receive supplement starting 2 nd week of life. 3. Lactating mothers should have at least 50 mg vitamin C daily. 4. Guava & papaya richer in vitamin C than citrus fruits, also in most green leafy vegetables, tomatoes & fresh tubers but absent in cereals, most animal products & canned milk. Treatment: Ascorbic acid 200 -500 mg daily or 100 -150 ml of fruit juice.

Be master of your habits, Or they will master you………
- Slides: 47