Nursing Process Jane R Bordner RN BSN Nursing

Nursing Process Jane R Bordner, RN, BSN Nursing Instructor HACC N 100 Spring 2014

Nursing

The Changing Face of Nursing

What Do Nurses Do? Nursing process gives us a direct and precise way to answer l Nursing process = a problem solving approach used to meet client needs l

Nursing Process l Is an organized, systematic method of giving individualized nursing care that focuses on identifying and treating unique responses of individuals or groups to an actual or potential alteration in health.

Nursing Process continued… l Based on the fundamental belief that every person is endowed with personal worth and dignity, and has a right to high quality care regardless of socioeconomic status, cultural background, or religious belief.

Purpose of Nursing Process ID nursing-related client health care needs l Establish a plan of care to meet needs l Implement nursing interventions/actions l Provide basis for ongoing evaluation l

Nursing Process and Critical Thinking Critical thinking is very important in nursing decision making l Critical thinking is necessary to make complex decisions involved in patient care l Critical thinking answers the question: who benefits and whose outcomes are being met by my nursing actions? l

Nursing Process and Critical Thinking l Critical thinking : analyze assumptions, challenge status quo, recognize limitations, and take actions to improve it.

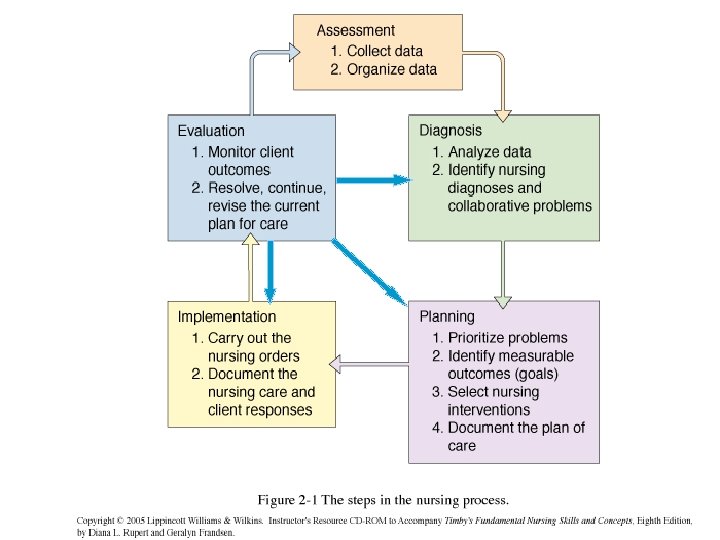
Steps in the Nursing Process Step 1 Step 2 Step 3 Step 4 Step 5 Assessment Nursing Diagnosis Planning Care Implementation Evaluation

Use of Nursing Process l Family member illness l Assessment l Diagnosis l Planning l Implementation l Evaluation

Role of the LPN l Assessment Assist in data collection l Nursing Diagnosis Assist in choosing ND l Planning Assist in formulating and choosing interventions l Implementation l Evaluation Carry out plan within scope of practice Assist in evaluation and revision of plan of care

Step 1: Assessment l l Thorough and holistic Based on: l l clinical and laboratory data medical history patient’s account of symptoms. Requires: l l data collection data validation data sorting data documentation

Types of Data l Subjective Data/Signs l l l Client’s perceptions What the client tells you. l Example: “I am in pain. ” “I feel nauseous. ” Objective Data/Symptoms l l Observations or measurements Things the nurse sees, hears, and feels. l Example: Vital signs, bowel sounds, temperature of skin

Subjective vs. Objective Data 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. ___ My leg pain is a throbbing pain ___ 2 seconds capillary refill ___ Lung sounds clear bilaterally ___ I have no allergies ___ I fell last night ___ Apical pulse 68 and regular ___ Patient moaning ___ Moderate yellow sputum ___ I am extremely tired ___ Skin warm and dry to touch

Shift Assessment Organized l Systematic l Brief l Accurate l Order depends upon presenting S&S l

Types of Assessments l Shift Assessment l Focused Assessment l Comprehensive Health Assessment
 l")
Focused Assessment Detailed assessment of particular system l Brief (2 to 5 minutes) l “Quick check” l ID changes in areas most likely to change l Based on problems ID’d in shift assessment or new problems that arise l Find changes early and avoid complications l

Example l Patient admitted with pneumonia. Though the nurse asks questions and assesses all systems, he/she will focus much more attention on the respiratory system listening to breath sounds, asking about shortness of air, cough, etc…

Example Next shift, same patient, l New nurse enters his room and he reports abdominal pain. The nurse will briefly assess all systems, but in addition to focusing on the respiratory system, he/she will also do a detailed assessment of the GI system. l

WHATSUP guide to Symptom Assessment l l l l W H A T S U P Where is it? How does it feel? Describe it? Aggravating and alleviating factors? Timing: When did it start? How long does it last? Severity on scale of 1 to 10 Useful other data. Other symptoms? Patient’s perception of problem

Using WHATSUP Mrs. Cooper, age 47, had a hysterectomy 2 weeks ago. She is admitted with a right calf deep vein thrombosis that she thinks resulted from having surgery. She rated her pain, which began 2 days ago and is constant, at 8. She has increased calf tenderness with leg movement. Leg elevation and Tylenol #3 increases her comfort. Her calf is hot to touch and red. Her legs measure: R calf 9 inches; L calf 8 inches; R thigh 14 inches; L thigh 14 inches.

Comprehensive Health Assessment of all body systems and detailed health history l Provides baseline of client’s health status and functional abilities at that time l Helps nurse determine plan of action to address client’s nursing needs l Abnormal assessment findings signal nurse to gather additional data in that area l

Parts of Comprehensive Health Assessment l Interview l Physical Exam l Complete l shift assessment Auxiliary Data

Components of Nursing Interview Biographical Data l Chief Complaint l History of Present Illness l Past Medical History l Environmental History l Psychosocial and Cultural History l Review of Systems (ROS) l

Important Interview Techniques Introduce yourself l Unhurried manner l Good eye contact (if culturally appropriate) l Silence/Listening skills/Clarifying l Observation skills (Get objective data during interview) l Age and developmental considerations l Continually work on developing therapeutic relationship l

What is Caring? Responding l Sensing emotions l Acceptance l Making a connection l “Caring for the Whole Person” l

Critical Thinking: Data Collection Your neighbor, Mr. Lewis, age 76, knocks on your door. He says “Look at my left foot. It is very swollen. I wore new shoes yesterday that felt tight. Now I can hardly get any shoes on this foot. There is a tender area on the top of my foot. I think something is wrong. Can you help me? ”

Sources of Data l Client l Family members or significant others l Other members of health care team l Current and previous hospital records l Diagnostic studies/Laboratory reports

Documentation of Data ALL objective and subjective data must be documented l Only what was observed by or stated to you l Subjective data using direct quotes l NOT DOCUMENTED, NOT DONE l
")
Common Diagnostic Tests l Blood CBC Electrolytes ABG’s Blood Glucose l Urine Urinalysis (UA) Urine Culture and sensitivity

Common Diagnostic Tests l Radiological Exams Chest X-ray Upper GI Lower GI CT & MRI scans l Stool Ova and Parasites Clostridium difficile (C. diff) Occult blood

Common Diagnostic Tests l Sputum Culture and Sensitivity Acid Fast Bacilli Cytology l Other EKG or ECG Stress Test TB Test

Medications Patient History Laboratory Studies Assessment Data

Step 2: Nursing Diagnosis Standardized label that identifies client’s problem l Makes it understandable to all nurses l Language of nurses l Address actual or potential health problems l

Step 2: Nursing Diagnosis ID’d by nurse after analyzing assessment data and comparing it with what is considered to be normal l Abnormal findings are organized into data clusters l Nursing diagnoses are developed from data cluster l

Nursing, Medical, Collaborative Diagnoses Nursing diagnoses: problems which can be treated independently by nurses l Medical diagnoses: those that require care that only a physician or nurse practitioner can render l Collaborative diagnoses: problems that can be helped by both medical and nursing interventions l

Medical VS. Nursing Diagnoses l Medical l ID’s pathological basis for illness l Focuses on physical condition only l Addresses actual problems l Nursing l ID’s response to illness l Focuses on physical, psychosocial, and spiritual needs l Addresses actual and potential problems

Medical VS. Nursing Diagnoses l Medical l Not validated with client l Uses standardized treatments and goals l May not be resolvable l Nursing l Validated with client l Uses individualized goals and interventions l Usually resolvable
")
Medical VS. Nursing Diagnosis Client admitted with medical diagnosis of congestive heart failure (CHF) l Look up medical diagnosis in front of your Nursing Diagnosis Handbook. l Many potential nursing diagnosis based on one medical problem l Assessment data will reveal which may best FIT YOUR client l
 l Part")
Writing Nursing Diagnoses l Part 1 Nursing Diagnosis Label related to (R/T) l Part 2 Etiology (cause) as evidenced by (AEB) l Part 3 Signs and Symptoms

Example Client has abdominal surgery this am. Assessment data reveals that the client is experiencing pain. It is rated by the patient as 4 on a scale of 0 to 5. The patient is also exhibiting facial grimacing and is moaning. l The nursing diagnosis related to this assessment data is ACUTE PAIN. l

Writing Nursing Diagnosis l Part 1 Acute pain related to… l Part 2 actual tissue damage from abdominal surgery as evidences by… l Part 3 Patient stating “My pain is 4 of 5. ” Moaning/ facial grimacing

Part 1 of Statement NANDA list of approved nursing diagnosis labels l Problems that nurses routinely address in practice l List in back of your Nursing Diagnosis Handbook l “I am so nauseated from my chemo treatments that I cannot eat anything. ” l

Part 2 of Statement Etiology or cause l Statement follows nursing problem and words “related to” = R/T l Comes from your nursing knowledge and assessment data l Etiology is individualized for each client l NO MEDICAL DIAGNOSIS l “I am so nauseated from my chemo treatments that I cannot eat anything. ” l

Part 3 of Statement Defining characteristics l Follows words “as evidenced by” = AEB l List signs and symptoms obtained from assessment l S&S that supports your statement l Use all relevant information l l Objective l Subjective l “I am so nauseated from my chemo treatments that I cannot eat anything. ”

Nursing Diagnosis Nausea R/T treatment/medications AEB pt stating “I am so nauseated from my chemo treatment that I cannot eat anything”.

Nursing Diagnosis: Actual vs. High Risk Problems l Actual l Existing problem l Client has S&S of problem l Requires 3 part nursing diagnosis statement l High Risk l High probability of occurring in future l There are no S&S l Requires 2 part nursing diagnosis statement

High Risk Diagnosis l Assessment Data l Patient has been on bedrest for 1 week l Patient is incontinent of urine l Patient unable to move or turn self in bed l Skin is clean and intact

High Risk Diagnosis Risk of impaired skin integrity: Risk factors: incontinence and physical immobility. *Note: This is a risk problem because no skin breakdown has occurred yet. You are going to use your nursing skill to prevent skin breakdown.

Nursing Diagnosis

Nursing Diagnosis Practice l Assessment Data l Patient states she is feeling “nervous and anxious”. l Her hand are shaking. l Staff observes her crying. l Progress notes state that her physician told her earlier that her lung biopsy was positive for cancer.

Nursing Diagnosis Anxiety R/T change in health status AEB pt stating that she feels “anxious and fearful” and episodes of crying and shakiness.

Nursing Diagnosis Practice l Assessment Data l 92 year old female. l Patient has weakness in all extremities. l Fatigues rapidly with activity. l Unable to perform ADL’s without becoming fatigued. l Frequently makes statements such as “I feel so tired and weak”.

Nursing Diagnosis Activity intolerance R/T generalized weakness AEB inability to perform ADL’s without fatigue and stating “I feel so tired and weak”.

Nursing Diagnosis Practice l Assessment Data l 82 year old male l Past medical history of a stroke with left-sided weakness and bilateral cataracts l Walks with a walker l Shuffling gait

Nursing Diagnosis Risk for falls R/T impaired vision/impaired mobility Impaired physical mobility R/T neuromuscular impairment AEB left-sided weakness and using walker to ambulate

Nursing Process Worksheet READ and HIGHLITE abnormal data l IDENTIFY objective vs. subjective data l What does abnormal data tell us? l What are some nursing diagnoses? l

Nursing Diagnoses What problems do you see here? l Are they actual problems or high risk problems? l How would you write them? l Look at NANDA list. What works for this patient? l

Nursing Diagnosis Worksheet l ACTIVITY PROBLEMS 1. Activity intolerance related to ______ AEB _______________. 2. Sleep deprivation related to ______ AEB _______________.

Nursing Diagnosis Worksheet 3. Fatigue related to __________ AEB _______________.

Nursing Diagnosis Worksheet • PAIN 1. • Chronic pain related to _________ AEB _______________. NUTRITION 1. Imbalanced nutrition: less than body requirements related to ________ AEB ________________.

Nursing Diagnosis Worksheet • SAFETY 1. • Impaired skin integrity related to _________ ABE ________________. RISK PROBLEMS 1. Risk for injury related to _______________.

Nursing Diagnosis Worksheet • OTHERS? 1. Impaired physical mobility related to _____________ AEB _______________.

Nursing Process Summary The nursing process is a problem solving approach. Experienced nurses engage in this type of thinking as a matter of routine. l You need to learn how to think this way in order to be a successful nurse. l

Nursing Process Summary

Types of Assessments l Shift Assessment l Focused Assessment l Comprehensive Health Assessment

Shift Assessment Involves a brief systemic review of client’s condition at beginning of a shift l Nurse compares assessment findings with those from previous shift l Takes 10 to 15 minutes l

Preparation ID client l Privacy l Keep client comfortable l Body mechanics l Lighting l Quiet l Equipment l

Shift Assessment l Equipment Needed l Stethoscope l BP cuff l Thermometer l Watch with a second hand l Pen light l Measuring Tape (maybe)

Cultural Sensitivity Cultural differences influence a patient’s behavior l Recognition of cultural diversity helps to respect the patient l Consider a patient’s l l Health beliefs l Use of alternative therapies l Nutritional habits l Family relationships l Use of personal space

Physical Assessment Includes Inspection l Palpation l Percussion l Auscultation l

Inspection l The use of vision and hearing to distinguish normal from abnormal findings l Use adequate lighting l Position and expose body parts l Inspect for size, shape, color, symmetry, position, and abnormalities l Side to side comparison l Pay attention to detail

Palpation Involves using the hands l Examine accessible body parts l Palpate skin l l Temperature, moisture, texture, turgor, tenderness, and thickness l Palpate abdomen l Tenderness, distention, or masses

Percussion Tapping the body with fingertips to produce a vibration l Character of sound l l Determines location, size, and density of structures l Depends on the density of tissues l Abnormal sounds can be mass, air, or fluid

Auscultation Listening to sounds produced by the body l Assess sounds heard in the heart, lungs, and gastrointestinal systems l Requires the use of a stethoscope l Characteristics include l l Frequency l Loudness l Quality l Duration

General Survey Begins when you first meet a patient l Begins with review of primary health pattern l The survey provides information regarding l l Characteristic of illness l Hygiene l Skin condition l Body image l Emotional state l Developmental status

General Appearance and Behavior Gender and Race Age Signs of Distress Body Type Posture Gait Body Movements Hygiene and Grooming Dress Body Odor Affect and Mood Speech Patient Abuse Subculture Abuse

Shift Assessment Includes Vital signs l Integumentary l Neurological l Musculoskeletal l Circulatory l Respiratory l Gastrointestinal l Genitourinary l Psychosocial l

Skin Assessment l Nursing history l l Color l Moisture l Temperature l Texture l Turgor l Vascularity l Edema l Lesions

Nails Inspection and palpation l Condition of nails reflects l l General health l Nutritional status l Occupations l Level of self-care

Hair and Scalp Use inspection l Assess l l Distribution l Thickness l Texture l Lubrication

Neurological l Mental Status l Orientation l Speech

Neurological System Conduct a nursing history l Assess l l Language l Intellectual function l Cranial nerve function l Sensory nerve function l Motor function

Head and Neck Inspection and palpation l Assess l l Headache, dizziness, seizures, poor vision, loss of consciousness l Head size, shape contour of head and skull l Facial symmetry

Nose and Sinuses Inspection and palpation l Assess for exposure to l l Dust l Pollutants l Allergies l Nasal obstruction l Trauma l Discharge, postnasal drip l Headaches

Mouth and Pharynx Assesses overall health l Determine oral hygiene needs l Develop therapies for dehydration l Assess oral trauma l Assess for airway trauma l

Oral Cavity

Neck muscles l Lymph nodes l Carotid arteries l Jugular veins l Thyroid gland l Trachea l

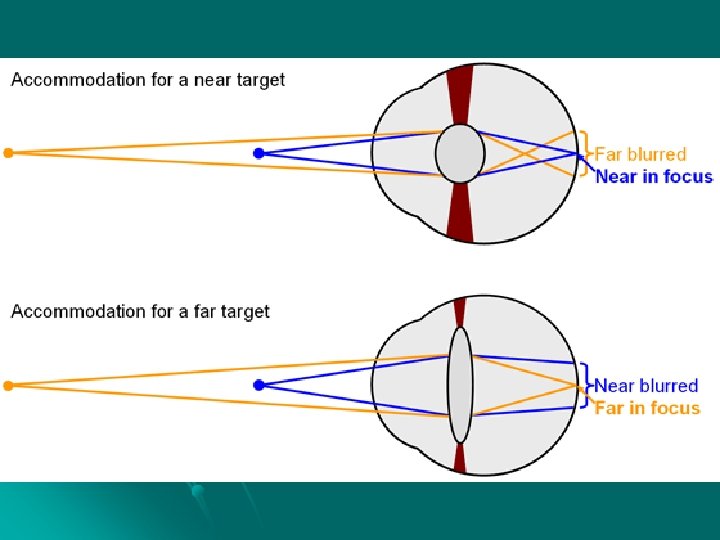
Eyes Vision

Ears Hearing

Circulatory l. Core Body Temperature l. Skin l. Color l. Temperature

Turgor Capillary Refill

Edema

Skin Integrity/Alterations

BP APICAL PULSE

Peripheral Pulses Radial Pulses 80 A/80 R


IV’s Peripheral

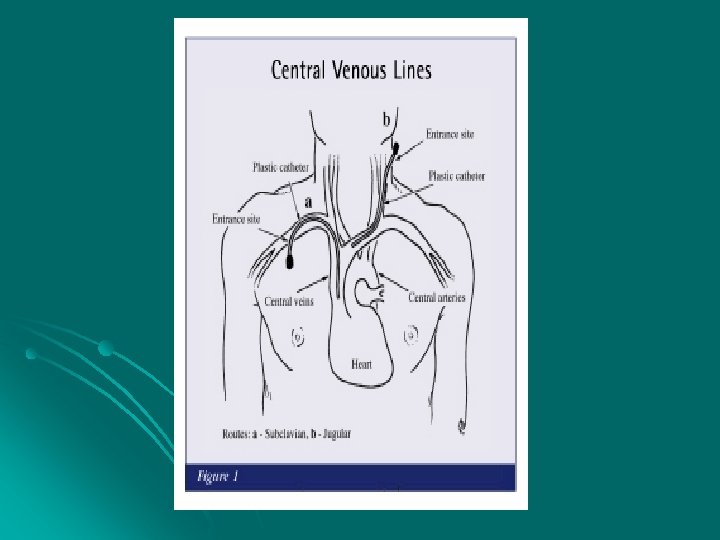
PICC

Mediport

Breasts Examine both female and male breasts l Take a health history l Use inspection and palpation l

Respiratory l Respirations l Cough

O 2 nasal cannula face mask

Lung Sounds RUL RML RLL LUL LLL

LUNG SOUNDS

Gastrointestinal Nutrition l. Diet l% eaten l. N&V l. Ht. & Wt.

Abdomen LOOK, LISTEN, & FEEL

Right Upper Quadrant RUQ RLQ Right Lower Quadrant Left Upper Quadrant LUQ LLQ Left Lower Quadrant

Bowels l What is “normal”? l Ask about l Frequency l Color l Consistency l Amount

Genitourinary l Urine l Intake and Output l Perineal Area

Foley Catheter Draining urine
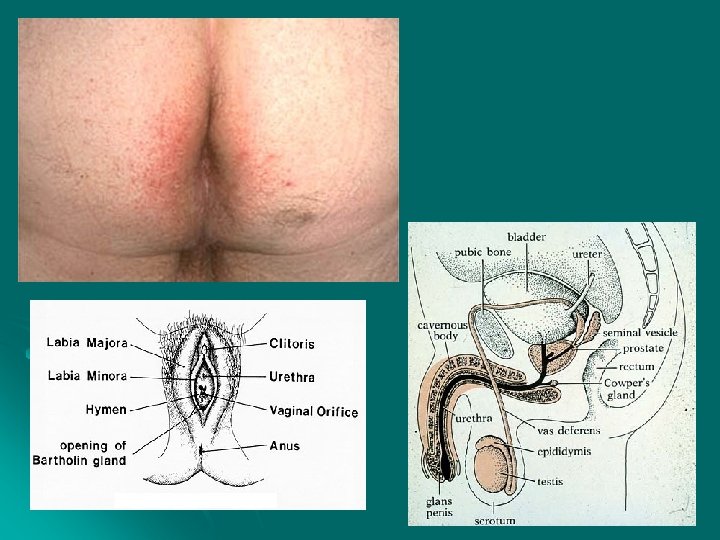

Female Genitalia Examination of the genitalia includes external and internal sex organs l Must provide privacy l Need to understand cultural sensitivity l Conduct a nursing history l Use inspection and palpation l

Male Genitalia Assess the integrity of external genitalia, inguinal ring, and canal l Conduct a nursing history l Use inspection and palpation l

Musculoskeletal l Gait l Posture l Extremities l. Contractures/Amputations l. Enlargement l. Alignment/Symmetry l. Heat, tenderness, edema

ROM

Muscle Strength

Abnormal Sensations

Musculoskeletal l. BUE l. BLE l. RUE l. LLE l. LUE l. RLE

Psychosocial l Emotional l Support System l Cultural l Spiritual/Religion l Social Interaction

Additional Data l Pain l Self-care Deficits

Wounds/Incisions 1. 2. 3. 4. 5. 6. 7. 8. 9. Kocher/Subcosta l Midline Mc. Burney Battle Lanz Paramedian Transverse Rutherford Morrison Pfannenstiel

Tubes/Drains
- Slides: 127