NURSING CARE OF A NEONATE Presented by Mrs

NURSING CARE OF A NEONATE Presented by Mrs. Benazeera Lecturer Dept. Child Health Nursing

NURSING CARE OF A NEONATE Presented by Mrs. Benazeera Dept. Child Health Nursing

Learning objective • Define newborn period • Discuss the physical and physiological characteristics of newborn

DEFINITION The normal newborn can be defined as a infant born at term, between 38 to 42 weeks, cries immediately after birth, establishes independent rhythmic respiration, quickly adapts with the extra- uterine environment, having average weight and no congenital anomalies.

General appearance • physically active, conscious, • Good muscle tone • Pink in color
 – Blood Pressure: • Age 12")
Age associated Vitals • Term Newborn (3 kg) – Blood Pressure: • Age 12 hours: 50 -70 / 25 -45 • Age 96 hours: 60 -90 / 20 -60 • Age 7 days: 74 +/- 22 mm. Hg (Systolic BP) • Age 42 days: 96 +/- 20 mm. Hg (Systolic BP) – Pulse: 80 -200 – Respiratory Rate: 40 -60

Physical characteristics of normal neonates: Weight • The average weight of a normal full term new born is 2. 5 - 3. 5 kg. • It may vary from country to country and indifferent socio-economic status. • 2. 8 kg for Indian babies

ASSESSMENT OF WEIGHT

CHEST CIRCUMFERENCE • The chest circumference is about 3 cm less than head circumference. • i. e, 30 -33 cms. • The head and chest circumference will be equal at one year.

ASSESSMENT OF HEIGHT

LENGTH • At birth the average crown to heel length of the term infant is 50 cm (20 inches) with the range of 48 -53 cm. • For boys 50 cm • For girls 49 cm

HEAD CIRCUMFERENCE • The head circumference is usually varies from 33 -37 cm. • with the average of 35 cm.

ASSESSMENT OF HEAD CIRCUMFERENCE

ASSESSMENT OF CHEST CIRCUMFERENCE

CHARACTERISTICS OF THE NEWBORN HEAD • The newborn head represents one-fourth of his total body length. • Its circumference is equal to that of his abdomen. • The average size is 13" to 14" (33 -35 cm). • The head is shaped or molded as it is forced through the birth canal in vertex presentations.

• The head is covered with fine silky hair is proportionately large than the body. • The head is one fourth the total length. • The cranium is large and the face relatively small when compared with adult cranium.

Regions and landmarks of the fetal skull • The skull comprises the vault, • Face • base

BONES IN THE SKULL • • Two frontal bones Two parietal bones One occipital bone Two temporal bones.
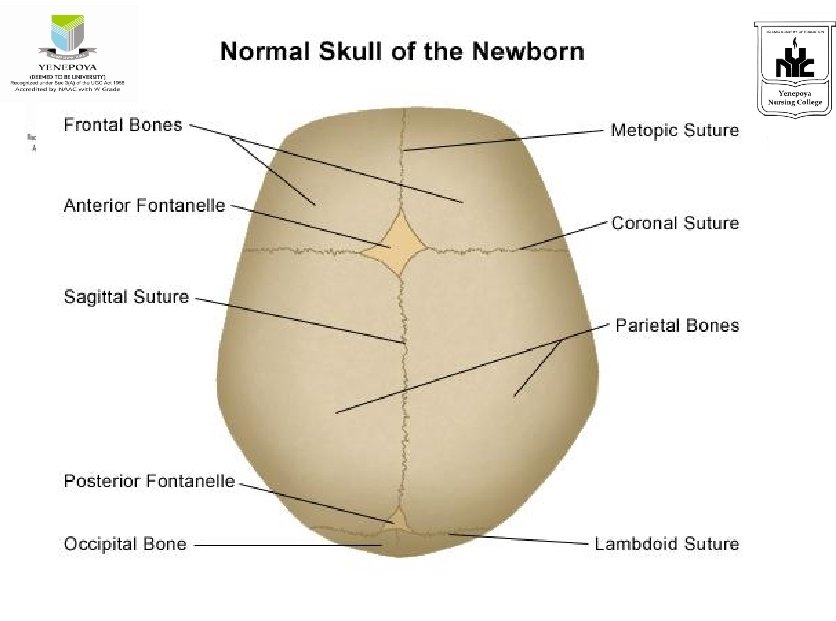

Fontanels • The infant's skull is separated one from another along the suture lines. • Where more than two bones come together, the space is called a fontanel. • This is the unossified space or soft spot between the cranial bones of the skull in an infant. • The infant's pulse is sometimes visible there.

• The anterior fontanel is located at the intersection of the sutures of the two parietal bones and the frontal bones. It is diamond-shaped and strongly pulsatile. It normally closes at 9 to 18 months of age. • The posterior fontanel is located at the junction of the sutures of the 2 parietal bones and 1 occipital bone. It is small, triangular shaped, and less pulsatile. It normally closes at 1 1/2 to 3 months of age. • The anterior fontanel is the larger of the two.

Anterior Fontanels Posterior Fontanels

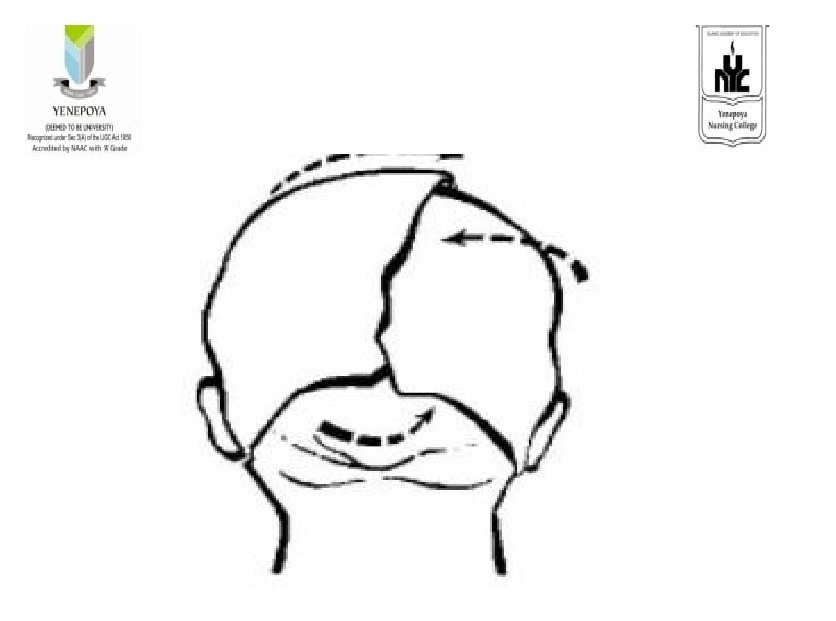
Molding • During delivery, for the large head to pass through the small birth canal, the skull bones may actually overlap in a process referred to as molding. • Such molding reduces the diameter of the skull temporarily. • This elongated look usually disappears a few hours after birth as the bones assume their normal relationships.

Cephalhematoma. This is a collection of blood between periosteum and flat skull bone.

Cephalhematoma

Cephalhematoma. • It is caused by pressure of the fetal head against the maternal pelvis during a prolonged or difficult labor. • The collection of blood does not cross the suture line. • It does not increase when baby cries.

Cephalhematoma • Bleeding is limited to the surface of the particular bone. • Most cephalhematomas are absorbed within several weeks. • No treatment is required in the absence of unexplained neurologic abnormalities.

Caput Succedaneum • This is an abnormal collection of fluid under the scalp on top of the skull • That may or may not cross the suture lines, depending on the size. • Pressure on the presenting part of the fetal head against the cervix during labor may cause edema of the scalp. • This diffuse swelling is temporary and will be absorbed within 2 or 3 days.

Newborn Scalp Hematomata

EYES • The eyes are blue or grey at birth change in to the permanent color in 3 to 6 months. • The iris may be grayish-brown or brown. • The eye movements are not coordinated and both eyes momentarily turn inward or outward. • The eyelids may be edematous for about 2 days after birth. Until the excess fluid eliminated by the kidneys.

• Pupils. The pupils do react to light • can focus on objects about eight inches away. • The infant's blinking is a natural protection reflex. • Lacrimal apparatus. The lacrimal apparatus is small and nonfunctioning at birth • tears are not usually produced with crying until one to three months of age.
 or infection of the tissue lining")
Ophthalmia neonatorum • Neonatal conjunctivitis is swelling (inflammation) or infection of the tissue lining the eyelids in a newborn.

CAUSES • A blocked tear duct • Infection by bacteria or viruses, • irritation from antibiotic eye drops containing silver nitrate.

SYMPTOMS • Infected newborn infants develop drainage from the eyes within 1 day to 2 weeks after birth. • The eyelids become puffy, red, and tender. • There may be watery, bloody, or thick pus-like drainage from the infant's eyes.

Treatment • Eye irrigation • For a blocked tear duct, gentle warm massage between the eye and nasal area may help. • This is usually tried before starting antibiotics. • If it has not cleared up by the time the baby is a year old, surgery may be needed.

• Antibiotics are often needed for eye infections caused by bacteria. • Eye drops and ointments may also be used. • Salt water eye drops may be used to remove sticky yellow drainage. • Special antiviral eye drops or ointments are used for herpes infections of the eye.

Subconjunctival hemorrhage • Subconjunctival hemorrhage is a frequent finding in normal newborns. • It results from the breakage of small vessels during the pressure of delivery. • The red area may be large or small • It does not affect vision, and spontaneously resolves in several days.

Subconjunctival hemorrhage

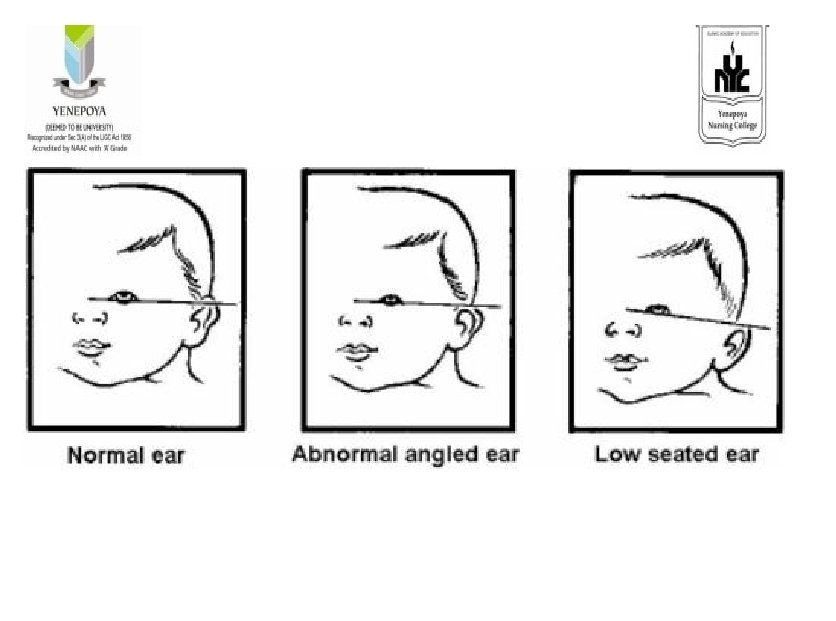
EARS • • The ears tend to be folded and creased. • A line drawn through the inner and outer canthi of the eye should come to the top notch of the ear where it joins the scalp. • The pinna is very soft • The infant usually responds to sound at birth.

• EAR TAG -A single, small ear tag is an occasional finding on physical examination. • It is often inherited as a familial trait. • EAR PITS (preauricular pits). They are located at the superior attachment of the pinna to the face and may be unilateral or bilateral.

EAR TAG

EAR PITS

STAHL'S EAR • This deformity of the pinna is characterized by a flat helix at the superior pole.

STAHL'S EAR

LOP EAR • This pinna deformity, where the superior edge of the helix is folded down, is known as lop ear.

LOP EAR

CUP EAR • Also known as "prominent ear", • cup ear refers to an auricle shape that stands away from the head at the superior, posterior, and inferior aspects.

CUP EAR

Nose • The narrow nostrils of the newborn may be slightly obstructed because accumulation of mucus. • It must be removed soon after birth to clear the airway.

DISLOCATED NASAL SEPTUM • A positional deformity of the nose, • But here the actual diagnosis is dislocated nasal septum • A dangerous look-alike which can result in permanent deformity if not corrected. • The vertical axis of the nose deviates to the infant's left.

DISLOCATED NASAL SEPTUM

MOUTH • The infant's lips should be pink and the tongue smooth and symmetrical. • The tongue should not extend or protrude between the lips. • The connective tissue attached to the underside of the tongue should not restrict the mobility of the tip of the tongue. • The gums may have tooth ridges along them, and rarely a tooth or two may have erupted before birth. • The roof of the mouth should be closed, and the uvula should be present.

EPSTEIN PEARL • The small white papule seen in the midline of the palate of this infant is an Epstein pearl.

EPSTEIN PEARL

Cleft lip and cleft palate • Cleft lip and cleft palate are birth defects • that affect the upper lip and roof of the mouth. • They happen when the tissue that forms the roof of the mouth and upper lip don't join before birth. • This can affect the way the child's face looks. It can also lead to problems with eating, talking and ear infections.

CLEFT LIP

CLEFT LIP

Treatment • Usually is surgery to close the lip and palate. • surgery in several stages. • Usually the first surgery is during the baby's first year. With treatment, most children with cleft lip or palate do well.

BOHN'S NODULES • Mouth nodules • are large, they are sometimes mistaken for teeth.

BOHN'S NODULES

ANKYLOGLOSSIA • Tongue-tie occurs in approximately 4% of newborns. • Many babies with this condition can breastfeed without difficulty, • but in some cases, a tight frenulum makes latching on difficult. In those cases, frenotomy may be indicated.

ANKYLOGLOSSIA

NATAL TEETH

NATAL TOOTH • This infant's tooth is erupted and is clearly visible.

NATAL TOOTH

MICROGNATHIA • Micrognathia, or "small jaw", • Underlying genetic conditions • There are quite a few chromosomal conditions associated with this finding.

MICROGNATHIA

SKIN • The infant has delicate skin at birth • That appears dark red. • This redness can be seen through heavily pigmented skin and becomes even more flushed when the baby cries.

VERNIX CASEOSA • This is a soft, white, cheesy, yellowish cream on the infant's skin at birth. • It is caused by the secretions of the sebaceous glands of the skin. • It offers protection from the watery environment of the uterus, is absorbed in the skin after birth, and serves as a natural moisturizer. • If there is a large amount of vernix caseosa present, it should be meticulously removed as it is thought to be a good culture medium for bacteria.

VERNIX CASEOSA

LANUGO • This is a long, soft growth of fine hair on the infant's shoulders, back, and forehead. • It disappears early in postnatal life.

LANUGO

MONGOLIAN SPOTS • These are blue-black colorations on the infant's lower back, buttocks, and anterior trunk. • They are often seen in infants of Black, Indian, Mongolian. • They disappear in early childhood.

MONGOLIAN SPOTS

PHYSIOLOGIC JAUNDICE • This is a yellow discoloration that may be seen in the infant's skin or in the scera of the eye. • Jaundice is caused by excessive amounts of free bilirubin in the blood and tissue. • Evident between the 3 rd and 7 th days. • Icterus neonatorum

PETECHIAE • These are small, blue-red dots on the infant's body caused by breakage of tiny capillaries. • They may be seen on the face as a result of pressure exerted on the head during birth.

PETECHIAE

MILIA • These are tiny sebaceous retention cysts. • They appear as small white or yellow dots and are common on the nose, forehead, and cheeks of the infant. • They are of pin head size. • Milia is due to blocked sweat and oil glands that have not begin to function properly. • They disappear spontaneously within a few weeks.

MILIA

BIRTHMARKS • These are small, reddened areas sometimes present on the infant's eyelids, mid-forehead, and nape of the neck. • They may be the result of local dilatation of skin capillaries and abnormal thinness of the skin. • They are sometimes called stork bites or telangiectasia. These marks usually fade and disappear altogether.

CUTIS MARMORATA

ERYTHEMA TOXICUM • This is the "rash" most commonly observed in newborn. • Lesions generally start on day 1 or 2 and increase in number over the next several days. • spontaneous resolution in about a week.

ERYTHEMA TOXICUM

PORT WINE STAIN • They are typically more intense and purple-red in color patches. • May affect a large surface area. • The discoloration is not, of itself, a problem, but it may be a clue to an underlying condition.

PORT WINE STAIN

Acrocyanosis • Symmetric cyanosis of the extremities.

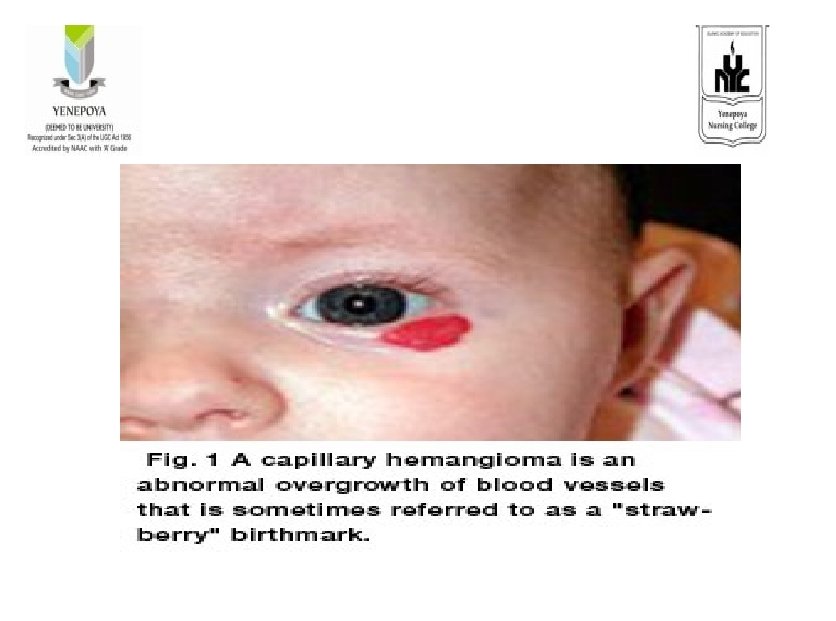
HEMANGIOMA OR STRAWBERRY MARK • A Hemangioma or strawberry mark is a type of birthmark that is characterized by a dark or bright red raised, in rough surface. • They do not develop for several days. • They may regress spontaneously or may even increase in size.

NECK • The neck appears short in composition. • Creases are present.

CHEST • The chest is bell shaped and at birth is approximately the same circumference as the abdomen. • And about 1 inch less than head. • For this reason it appears small. • The clavicle will be smooth while palpation • If it is bulged indication of fracture during birth.

• The thorax of the newborn is almost circular. • The anterior and lateral diameters are almost equal. • The child does not use the chest for respiration only diaphragm and abdominal muscles are using.

ABDOMEN • Appears rounded and slightly protruded. • Peristaltic waves can seen over the abdomen. • Bowel sounds may be heard soon after birth.

Esophagus • The cardiac sphincter and pyloric sphincter is not as well developed.

Stomach • The capacity of the infant's stomach is about one to two ounces (30 to 60 ml) at birth, but increases rapidly. • Milk passes through the infant's stomach almost immediately. • The infant is capable of digesting simple carbohydrates and proteins, but has a limited ability to digests fats.

UMBLICAL CORD


UMBILICAL CORD • The connection between the fetus and the placenta • It is a bluish white gelatinous structure at birth. • It normally contains 2 umbilical arteries and 1 umbilical vein encased in wharton`s jelly. • The presence of these structure should be determined when the cord is cut.

• Day by day gradual color changes will occur in the umbilical cord and it sloughs off by 6 -10 days after birth. • Granulating area that heals in another week.

INTESTINES • Irregularity in peristaltic motility slows stomach emptying. • Peristaltic increases in the lower ileum, which results in one to six stools a day.

Anogenital area • The buttocks are plump and firm. • In the anal region there should be no redness and fissures. • The size of the genitalia penis scrotum varies. • The scrotum seen edematous and dark in color. • The testes descended in to the scrotum

• Female genitalia may be slightly swollen. • The labia minora and clitoris appear large.

Urine • • The bladder contains urine at birth. And may empty immediately after birth. Some cases it may delayed up to second day. It is diluted because of the immature kidneys.

MECONIUM • The first stools after birth and for three to four days afterwards are called meconium. • It is sticky odor less material. • Meconium is stringy, tenacious, and black and has a tarry texture. With the ingestion of colostrum or formula, a gradual transition occurs. • It must be passed from 8 to 24 hours after birth.

Skeletal structures • Bones are very soft. • Skelton is flexible and joints are elastic. • The back is normally straight and flat.

Extremities • The arms and legs are relatively short. • If the feet both do not align normally with manipulation a talipes deformity may be suspected (club foot).
")
• • Common anomalies are Club foot Syndactyly (union of the finger toes) Polydactyly (supernumerary digits)

Muscular development • Muscles are smooth. • Prone for injuries • Muscle movements are uncoordinated.

Physiological characteristics

Circulatory • The heart rate : 120 -160 beats • Blood pressure ranges from: 60 -80 mmof Hg systolic and diastolic 25 -40 mm of hg. • Transitional Circulation = acrocyanosis • Peripheral circulation = sluggish • High: RBC 4. 8 -7. 1; Hg: 14 -24; • WBC 18, 000 @ birth; 23 -24, 000 @ 1 day • Coagulation: Vit. K dependent clotting factors are decreased. • Platelet counts (150, 000 -350, 000)

Respiratory • 30 -60 b/m • Before birth O 2 needs met by placenta • After delivery -need mature lungs that are vascularized, have surfactant and sacules - usually adequate by 32 -35 weeks.

Gastrointestinal System • Immature at birth, reaches maturity at 2 -3 years of age • place food at back of tongue • sucking becomes coordinated @32 wks • little saliva until 3 months of age • bowel sounds after 1 hour of birth
 • NB have difficulty digesting complex starches and fat • Abdomen becomes")
Gastrointestinal (continued) • NB have difficulty digesting complex starches and fat • Abdomen becomes easily distended after eating • Initial fecal material = meconium • No normal flora at birth in GI system to synthesize Vit. K

Immune System • Limited specific and Non-specific immunity at birth • passive immunity(from mom- Ig. G) for the first 3 months of life ~ this will be reduced if baby is born premature • breastfeeding = ^ passive immunity (Ig. A)

Temperature Regulation • 36. 5 c to 37. 5 • brown fat is the primary source of heat production. Brown fat is broken down into glycerol & fatty acids producing heat. • Brown fat is found @ the nape of the neck, axillae, around the kidneys and in the mediastinum. • Slightly warmer to touch than normal skin.

Cold Stress • An increase in the metabolic rate associated with non-shivering thermogenesis --> increased O 2 demands and caloric consumption • It’s important to provide a neutral thermal environment to prevent metabolic acidosis and prevent depleted brown fat.

Kidneys and Urination • 92% of all healthy infants void in the first 24 hrs of birth • initial urine: cloudy, scant amounts, uric acid crystals-> reddish stain on diaper • Kidneys not fully functional until child is 2 years of age.

Hepatic Function • Liver produces substances essential for clotting of blood. • Stores needed iron for the first few months. Preterm & small infants have lower iron stores than full term and heavier infants. (full term infants stores last 4 -6 mo) • NB at risk for Physiologic Jaundice after 24 hours of age, due to increased breakdown of RBC’s and immature liver functioning.

Increased Bilirubin Levels • Jaundice in the 1 st day is NOT normal • Bilirubin level greater than 12 at any time needs further attention • Maternal causes of increased bilirubin levels in the NB: epidural use, oxytocin induced labor, infection, hepatitis

Kernicterus • Complication of neonatal hyperbilirubinemia -> encephalopathy • basal ganglia and other areas of the brain and spinal card are infiltrated w/ bilirubin (produced by the breakdown of hemoglobin -> levels of 20 - 25 or more). • Poor prognosis if untreated.

Neurologic • All neurons are present, but many are immature: • uncoordinated movements • poor muscle control • startle easily • tremors in extremities

Weight Loss • It is normal for the newborn infant to loose 510% of weight in the first 4 to 5 days of life.
, Maternal and Child Health Nursing, 6 th edition, Lippincott")
References • Adele Pillitteri (2010), Maternal and Child Health Nursing, 6 th edition, Lippincott Williams and Wilkins Publications. • Lowdermilk Perry (2007), Maternity and Womens Health Care, 9 th edition, Mosby Elsevier Publications. • Wong Perry, Hockenberry and Lowdermilk Wilson (2006), Maternal Child Nursing Care, 3 rd edition, Mosby Elsevier Publications. • Emily Wone Mckinney, Sharon Smith Murray, Jean Weiler Ashwill (2009), Maternal Child Nursing, 3 rd edition, Saunders Elsevier Publications. • Susan A. Orshan (2008), Maternity, Newborn and Womens Health Nursing, 1 st edition, Lippincott Williams and Wilkins.
- Slides: 126