NUCLEAR CARDIOLOGYBASICS Dr THIRUMURTHI CHIEFNUCLEAR MEDICINE MADRAS MEDICAL

NUCLEAR CARDIOLOGYBASICS Dr. THIRUMURTHI CHIEF-NUCLEAR MEDICINE MADRAS MEDICAL MISSION

Nuclear Medicine Specialty in which a wide range of clinical conditions are investigated using radioactive tracers administered to the patient n It is completely different process from X -Ray, CT and MRI scan (these look at the anatomy of the body) n To look at the function of the body, Nuclear Medicine uses gamma rays n

Nuclear Medicine Gamma rays are very similar to X-Rays, but the major difference is that the gamma rays are emitted by pharmaceuticals injected into the bloodstream rather than being produced by machines outside the body. n Gamma rays are detected by the gamma camera n
")
Gamma Rays (from Doe Medical Sciences webpage)

Myocardial Perfusion Imaging Radiopharmaceuticals : h 201 Thallium h Technetium based agents PET * Ammonia

Technetium based agents T 1/2 - 6 Hrs Pharmaceuticals : Sesta. MIBI, Tetrofosmin i Sesta. MIBI: Methoxy Iso Butyl Isonitrile i Passive diffusion i Uptake proportional to blood flow & no redistribution i Good quality images, gating, easy availability & Cost effective i 99 m Technetium

Exercise stress testing n n n Treadmill or bicycle ergometer Protocols vary - symptom limited Bruce most popular n n Achieve at least 6 METS for diagnostic accuracy 8 stages Incline and speed increment every 3 minutes Target 85 -100% maximum age predicted HR © Continuing Medical Implementation …. . . bridging the care gap

MPI Stress Procedure i Treadmill i Pharmacological stress IV Dobutamine / Adenosine DOBUTAMINE Max. Dosage: 40 ug / kg / min + Inj. Atropine 0. 6 mg IV ADENOSINE Dose : 140 ug / kg / min - 6 min

Indications i Screening of IHD i Physiological significance of lesions post CAG i Post PTCA & post CABG evaluation i Risk stratification i Myocardial viability detection

Diagnostic Accuracy % Sensitivity % Specificity % Predictive Accuracy Exercise Stress ECG 1 Exercise Stress Echo 1 67 74 69 85 79 83 MPI 1 89 80 89 1. O’Rourke RA, et al. Circulation. 2000; 102: 126 -140. 2. Wackers FJ, et al. Nuclear cardiology. In: Braunwald E, ed. Heart Disease: A Textbook of Cardiovascular Medicine. 5 th ed. Philadelphia, Pa: WB Saunders; 1997.

PET Myocardial Imaging PET Perfusion Imaging PET Metabolic Imaging

Flow tracers Rb-82 n 0 -15 n N-13 n Tc-99 m MIBI n Tl-201 n
 F-18 –BMS 747158 n I-123 BMIPP n")
Metabolic tracer n F-18 – fluorodeoxyglucose(FDG) F-18 –BMS 747158 n I-123 BMIPP n
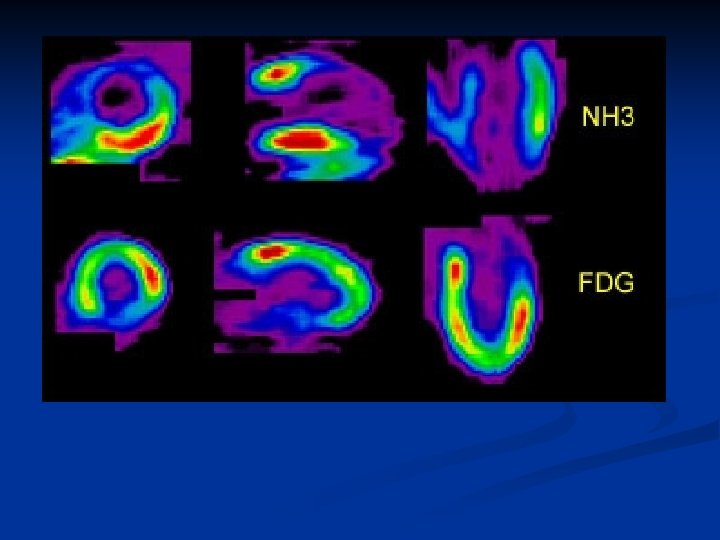

Perfusion Metabolism Dysfunction Reversible Irreversible Condition Stunning Hibernation Scar

MIBI & FDG 30% OF NO PERFUSION SEGMENT SHOWS FDG UPTAKE
 20 16 Influence of Viability Testing on Outcomes With")
Annual Cardiac Death Rate (%) 20 16 Influence of Viability Testing on Outcomes With Revascularization -80% p<0. 0001 16 p=NS 12 7. 7 8 4 0 6. 2 3. 2 Revasc Med Rx Viable (Allman, JACC 2002; 39: 1151 -1158) Revasc Med Rx Non-viable

ACC/AHA Recommendations for the Use of Radionuclide Techniques to Assess Myocardial Viability Indication Test Class Level of Evidence Predicting improvement in regional and global LV function after revascularization Stress /redistribution/reinjection 201 T II B Rest-redistribution imaging I B Perfusion plus PET FDG imaging I B Resting sestamibi imaging I B Late 201 Tl redistribution imaging (after stress) IIb B Class I: Conditions for which there is evidence and/or general agreement that a given procedure or treatment is useful and effective LOE B: Data derived from a single randomized trial, or from nonrandomized studies
")
First-Pass Radionuclide Angiography (RNA)
 n Valvular heart disease n Congenital heart disease n")
Indications Coronary artery disease (CAD) n Valvular heart disease n Congenital heart disease n

Equilibrium Gated Radionuclide Ventriculogram MUGA

Purpose Examine the function of the pumping chambers of the heart n Left ventricle measurements are more accurate than the right because of the heart’s anatomy (gated first-pass study with radionuclides that do not pass the lungs maybe used for the right ventricle) n

BPGS - Blood Pool Gated SPECT Analysis:
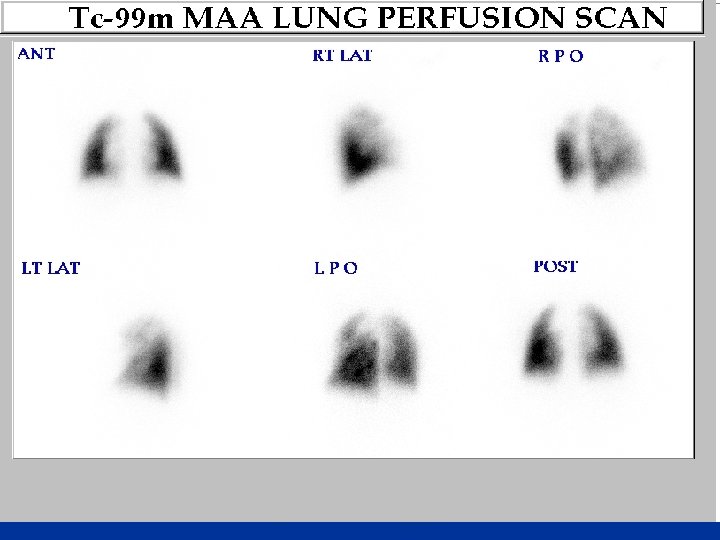

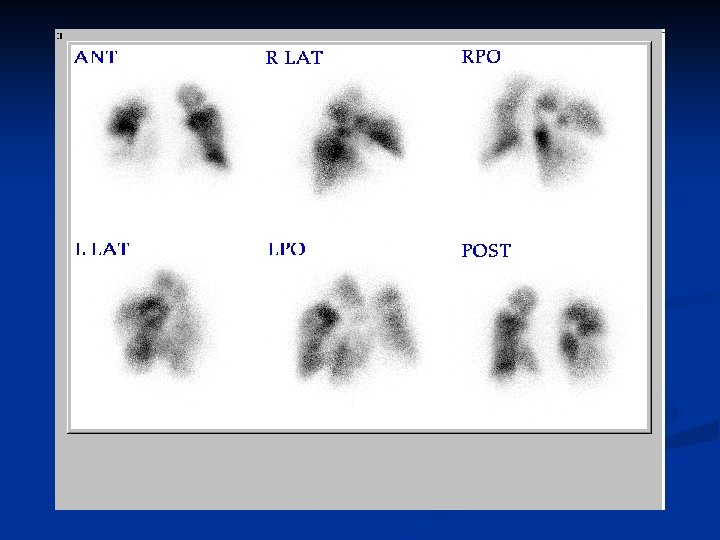
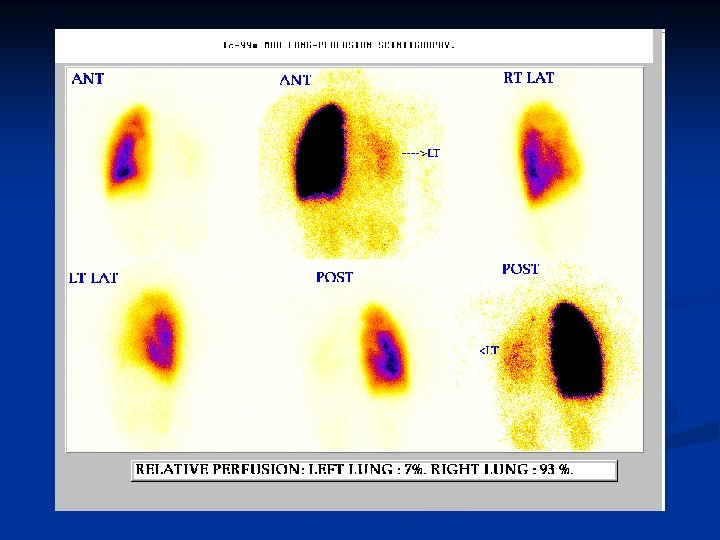

Imaging • CTPA is now the recommended initial lung imaging modality for non-massive PE. [B] • Patients with a good quality negative CTPA do not require further investigation or treatment for PE. [A] • Isotope lung scanning may be considered as the initial imaging investigation providing (a) facilities are available on site, and (b) chest radiograph is normal, and (c) there is no significant symptomatic concurrent cardiopulmonary disease, and (d) standardised reporting criteria are used, and (e) a non-diagnostic result is always followed by further imaging. [B]
- Slides: 34