Nuances of Diabetes Management Arash Nafisi MD Olive

Nuances of Diabetes Management Arash Nafisi, MD Olive View – UCLA Medical Center Fall, 2018

Objectives • Review evidence behind role of diet, weight loss and exercise in the prevention and treatment of diabetes • Pharmacologic options for management of Type 2 Diabetes Mellitus • Nuances of oral hypoglycemics, including newer agents on DHS formulary • Nuances of insulin therapy, indications for insulin pens • Practical tips/tools to help close the gap our treatment of DM • Discussion of prescribing practices • Pitfalls in prescribing DM medications/supplies • What to do with patients with chronically uncontrolled DM • Food insecurity and DM
 and")
Case 1 Ms. Predia Betes is a 38 F with obesity (BMI 32) and Pre-DM (A 1 c 6. 2 six months ago). She is asymptomatic, though asks whether she needs to be tested again for diabetes. What do you advise? A. Test her today – why not? B. Test her in 6 months C. Test her in 2. 5 years D. Test her for Gonorrhea
 and")
Case 1 Ms. Predia Betes is a 38 F with obesity (BMI 32) and Pre-DM (A 1 c 6. 2 six months ago). She is asymptomatic, though asks whether she needs to be tested again for diabetes. What do you advise? A. Test her today – why not? B. Test her in 6 months C. Test her in 2. 5 years D. Test her for Gonorrhea
 and")
Case 1 Ms. Predia Betes is a 38 F with obesity (BMI 32) and Pre-DM (A 1 c 6. 2 six months ago). She is asymptomatic, though asks whether she needs to be tested again for diabetes. What do you advise? A. Test her today – why not? B. Test her in 6 months C. Test her in 2. 5 years D. Test her for Gonorrhea

Diabetes Screening Recommendations Hopkins Module, DM 2018

Case 2 Ms. Diane B. Tease is a 42 F with HTN. She is noted to have an A 1 c of 7. 4 and fasting glucose on BMP of 155. She is non-adherent with her two HTN medications, citing “I’m too young to be on pills. ” What is the next step in management of her newly diagnosed diabetes? • A. Just give up and refer her to Endocrine • B. Start weight based insulin • C. Start an oral hypoglycemic such as Metformin or Glimepiride • D. Discuss the importance of lifestyle changes and work with patient to come up with SMART goals to achieve this.

Case 2 Ms. Diane B. Tease is a 42 F with HTN. She is noted to have an A 1 c of 7. 4 and fasting glucose on BMP of 155. She is non-adherent with her two HTN medications, citing “I’m too young to be on pills. ” What is the next step in management of her newly diagnosed diabetes? • A. Just give up and refer her to Endocrine • B. Start weight based insulin • C. Start an oral hypoglycemic such as Metformin or Glimepiride • D. Discuss the importance of lifestyle changes and work with patient to come up with SMART* goals to achieve this. SMART Goals = Specific, Measurable, Attainable, Relevant, Time-based

Lifestyle Modification and DM

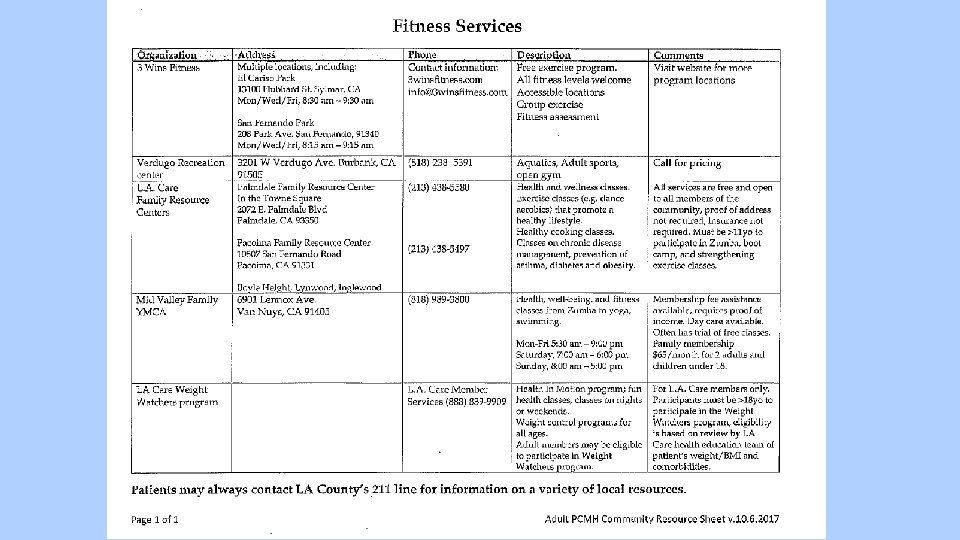
Effective Counseling for Lifestyle Changes • Can lower A 1 c by 1 -2% (more than any oral hypoglycemic) • In my experience, can lower A 1 c much, much more • • Set SMART goals, document this in the chart and re-address at every visit Eliminate liquid calories Focus on foods patient CAN eat rather than foods they can’t eat Portion control Stimulus control Calorie/carb counting, read nutrition labels and keep food log Can also refer to programs that can help with this: • DM Group Education Classes • Nutritionist (e-consult) • Fitness resource sheet (Amb Comm) • 3 Wins Fitness (free exercise program at El Cariso Park), FRC, YMCA, LA Care Weight Watchers

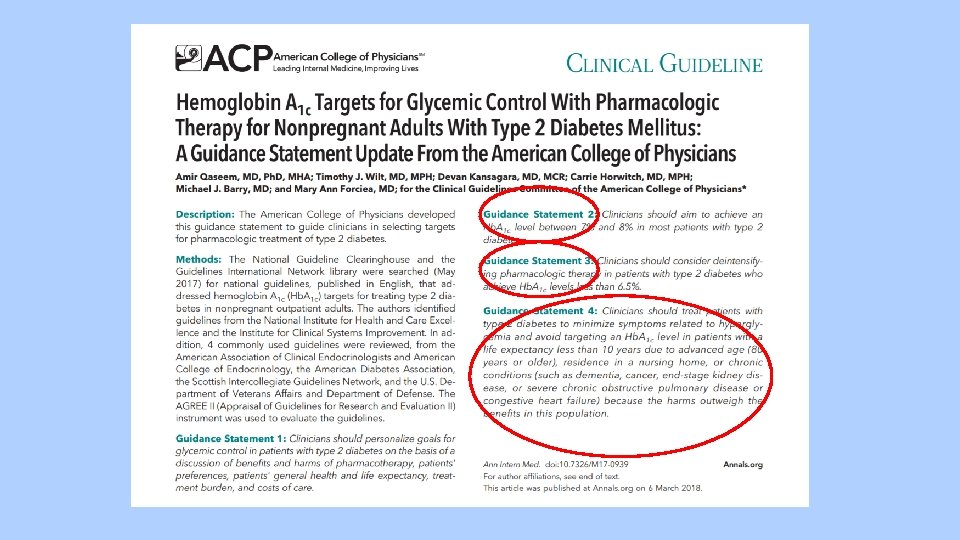
Case 3 Mr. O. B. City is a 71 year old homeless male with longstanding DM, cirrhosis, CKD, CAD who has tried making lifestyle changes, though his most recent A 1 c is 7. 6 on his current regimen. He asks your advice about risks/benefits of adding another agent. • What factors would push you to consider more lenient glycemic control for this patient?
")
Glycemic Targets - Individualization is Key Tight Glycemic Control (Lower A 1 c Goal) Lenient Glycemic Control (Higher A 1 c Goal) Younger patients Older patients Healthier patients with less co-morbidities Sicker patients with co-morbidities (CKD, liver disease, etc) Newly diagnosed diabetes Long-standing diabetes Longer life-expectancy Shorter life-expectancy Fewer CV complications Significant CV complications Highly motivated, adherent, good self-care capability Less motivated, non-adherent, poor self care Steady, readily available resources Limited resources Goal: decrease MICROvascular complications (retinopathy, nephropathy, neuropathy) • Each 1% reduction in A 1 c results in ~37% reduction in risk for microvascular complications. • No evidence that A 1 c < 7 reduces clinical microvascular or macrovascular events
 have")
Tight Glycemic Control and Macrovascular Complications • Three studies (ACCORD, ADVANCE, and VADT) have tried to determine optimal A 1 C targets to reduce macrovascular complications. • The ACCORD study • Compared cardiac outcomes (nonfatal MI, nonfatal CVA, or cardiovascular death) for patient treated to usual care (A 1 C 7. 0 -7. 9%) vs intensive treatment (A 1 C <6. 0%). • After 3. 5 years, the study had to be prematurely terminated because they found a 22% increase in all-cause mortality and 35% increase in cardiovascular death in the intensive treatment group. • Also significantly more weight gain, hypoglycemia and fluid retention • Similar results in patients with type 1 diabetes • Lowering the A 1 C below 7% doubles the risk of death (Hopkins Module - DM) No evidence that glycemic control leads to lower macrovascular complications

Case 4 Mr. Max Dose is a 41 M with HTN, DM, HLD. His A 1 c is 8. 1 on max dose Metformin, Glimepiride and Pioglitazone. He really does not want to start insulin because he is afraid of needles and has a difficult living situation. You decide to: A. Start him on insulin anyway – he’ll get over it. B. Have him come back in 3 months and pray that his A 1 c will be < 7 C. Start Empagliflozin 25 mg 0. 5 tabs qday

Case 4 Mr. Max Dose is a 41 M with HTN, DM, HLD. His A 1 c is 8. 1 on max dose Metformin, Glimepiride and Pioglitazone. He really does not want to start insulin because he is afraid of needles and has a difficult living situation. You decide to: A. Start him on insulin anyway – he’ll get over it. B. Have him come back in 3 months and pray that his A 1 c will be < 7 C. Start Empagliflozin 25 mg 0. 5 tabs qday
 *First line agent Sulfonylureas (Glimepiride, Glipizide) Thiazolidinediones (TZDs) (Pioglitazone)")
Comparing Oral Hypoglycemics Biguanide (Metformin) *First line agent Sulfonylureas (Glimepiride, Glipizide) Thiazolidinediones (TZDs) (Pioglitazone) Sodium-glucose cotransporter (SGLT 2) inhibitors (Empagliflozin) Reduces A 1 c by ~ 1. 5% Reduces A 1 c by 1 -1. 5% Reduces A 1 c by 1% Low risk of hypoglycemia Improves TGs, LDL, HDL Risk of hypoglycemia (particularly glyburide) Less hypoglycemia than Sulfonylureas Low risk of hypoglycemia Improved BP Less weight gain Weight loss Shown to improve CV outcomes (!) GI side effects, B 12 deficiency Lactic acidosis (more likely with renal/hepatic dz) Stimulate B-cells to produce insulin becomes less effective over time Edema, CHF, bone loss Blocks glucose reabsorption in kidney dehydration and genital fungal infections. Contraindicated in CKD Low cost Somewhat expensive Expensive
 • NEJM, 2015")
Empagliflozin • Inhibitor of the Na-glucose co-transporter (glucose, Na not reabsorbed) • NEJM, 2015 – randomized, double-blinded, placebo-controlled, multi-centered trial with 590 sites in 42 countries, Funded by Eli Lily and Boehringer Ingelheim. 7 K patients completed trial, mean duration 2. 5 yrs • Primary outcome (death from CV events, non-fatal MI/stroke) • Empagliflozin 10. 5% vs 12. 1% Control; HR 0. 86, p=0. 04, ARR 1. 6%, RRR 15. 7%, NNT 62 • Also, Empagliflozin had significantly lower risk of: • Death from CV causes (HR 0. 62) • Death from any cause (HR 0. 68, ARR 2. 6%, NNT 38) • Hospitalization for heart failure (HR 0. 65) • Empagliflozin with 5 lbs more weight loss and 3 mm lower SBP than control • Adverse events: higher risk genital infxns (1. 8% vs 6. 4%); no difference in UTIs, significantly less AKI than placebo • To prescribe: endocrine approval (i. e. e-consult) with prior authorization

When to Step Up Management • There is no one answer that will apply to all patients… • Ms. M. E. – A 1 c 16, drinking 1. 5 2 L bottles day of soda when cut this out, and started Metformin, A 1 c down to 7. 4 When to Start… American Diabetes Association Monotherapy Diabetes with A 1 c above goal Dual Therapy A 1 c > 9 Triple Therapy Failure of dual therapy Insulin A 1 c > 10 • Patient preference, home life and social determinants very important Adapted from Hopkins Module, DM 2018
")
Case 5 Mr. Insu Lin is a 56 M with obesity (weight 95 kg) poorly controlled DM with an A 1 c of 9. 7 on 3 max-dose hypoglycemic (Metformin, Glimepiride, Pioglitazone). He is amenable to starting insulin and wants to know his options. You tell him: • A. You don’t need insulin – you need a new name • B. Start Glargine 10 units and Lispro 2 units TIDAC in addition to your home DM regimen • C. Start a long acting insulin, 10 units daily and stop Glimepiride or Pioglitazone
")
Case 5 Mr. Insu Lin is a 56 M with obesity (weight 95 kg) poorly controlled DM with an A 1 c of 9. 7 on 3 max-dose hypoglycemic (Metformin, Glimepiride, Pioglitazone). He is amenable to starting insulin and wants to know his options. You tell him: • A. You don’t need insulin – you need a new name • B. Start Glargine 10 units and Lispro 2 units TIDAC in addition to your home DM regimen • C. Start a long acting insulin, 10 units daily and stop Glimepiride or Pioglitazone*

When To Start Insulin • Evidence is lacking – “art” of medicine • The best medicine in the one the patient actually takes • Patients have to be ready for insulin and understand how to use it • Requires: • Patient education • Understanding of patients’ home life, social history, stressors, support systems • Discussion of risks/benefits/alternative, lots of counseling/education, close follow up • If patient agrees to start insulin, it’s important that nursing provide insulin teaching (how to use insulin, how to check sugars, etc)

How to Start and Up-Titrate Insulin • Start basal insulin (Daily Glargine or Bedtime Insulin/Daytime Orals) • Starting dose of 10 units (or 0. 1 -0. 2 units/kg) • No evidence for difference in NPH vs Glargine • NPH cheaper, often BID, though can be mixed with Regular insulin; more hypoglycemia, though perhaps safer/less hypoglycemia when used in hospital • 70/30 insulin – restrictive b/c of fixed doses. Not generally recommended. • Okay to continue either TZD (Pioglitazone) or SU (Glimepiride/Glipizide) • TZDs increase insulin sensitivity (though also cause weight gain) • SUs can help with glucose control (though become less effective over time) • Need to D/C all oral hypo-glycemics except Metformin when starting short-acting insulin • Continue up-titration of basal insulin until AM pre-prandial FS at goal • Can increase insulin by 10 -20% 1 -2 x/week • No clear evidence about when to switch from Glargine qday to BID • Perhaps when daily dosing exceeds 50 -90 units. Concern for unreliable absorption • Don’t be afraid to change/simplify a complicated regimen (i. e Glargine + Lispro TIDAC Glargine only)

DM Supplies • Insulin • Syringes • Glucometer • Test Strips • Lancets • Alcohol Pads • Glucose Log (highlighting when you’d like patient to check sugars) • If Lantus Basaglar (pen) with pen needles

Case 5 – Continued • You decide to start patient on long acting insulin, 10 units q. HS and ensure he gets RN teaching. He asks: when should I check my sugars? Insulin When to Check Glucose Glargine AM Pre-Prandial NPH nightly AM Pre-Prandial NPH BID AM Pre-Prandial and PM Pre-Prandial Short-acting 2 hours after meals in which inject short-acting insulin • So if patient is placed on Glargine + Lispro TIDAC, patient would be injecting insulin 4 times per day AND should be checking AM pre-prandial FS AND 2 hours after all 3 meals (!)

Insulin Characteristics Hopkins Module, DM 2018

Case 6 Mr. Homeny Vials is a 46 M with DM, on NPH 40 units BID. He calls you and says he is out of insulin, even though you prescribed 3 vials of insulin 3 months ago. How many vials of insulin do you need to prescribe so that he has enough insulin to last him 3 months? A. 4 vials B. 6 vials C. 8 vials D. Vial are you asking me this question?

Case 6 Mr. Homeny Vials is a 46 M with DM, on NPH 40 units BID. He calls you and says he is out of insulin, even though you prescribed 3 vials of insulin 3 months ago. How many vials of insulin do you need to prescribe so that he has enough insulin to last him 3 months? A. 4 vials B. 6 vials C. 8 vials D. Vial are you asking me this question?

Insulin Vials • 1 m. L = 100 units of insulin • 10 m. Ls = 1 vial = 1000 units of insulin • If a patient is on 10 units of insulin per day will use 300 units per month and 900 units every 3 months 1 vial • If on 50 units/day ___ units/month ___ units/3 months __ vials • Shortcut: for every 10 units/day of insulin, need to prescribe 1 vial • If on Glargine 60 units/day __ vials • If on NPH 40 units BID __ vials

Insulin Vials • 1 m. L = 100 units of insulin • 10 m. Ls = 1 vial = 1000 units of insulin • If a patient is on 10 units of insulin per day will use 300 units per month and 900 units every 3 months 1 vial • If on 50 units/day 1500 units/month ___ units/3 months __ vials • Shortcut: for every 10 units/day of insulin, need to prescribe 1 vial • If on Glargine 60 units/day __ vials • If on NPH 40 units BID __ vials

Insulin Vials • 1 m. L = 100 units of insulin • 10 m. Ls = 1 vial = 1000 units of insulin • If a patient is on 10 units of insulin per day will use 300 units per month and 900 units every 3 months 1 vial • If on 50 units/day 1500 units/month 4500 units/3 months _vials • Shortcut: for every 10 units/day of insulin, need to prescribe 1 vial • If on Glargine 60 units/day __ vials • If on NPH 40 units BID __ vials

Insulin Vials • 1 m. L = 100 units of insulin • 10 m. Ls = 1 vial = 1000 units of insulin • If a patient is on 10 units of insulin per day will use 300 units per month and 900 units every 3 months 1 vial • If on 50 units/day 1500 units/month 4500 units/3 months 5 vials • Shortcut: for every 10 units/day of insulin, need to prescribe 1 vial • If on Glargine 60 units/day __ vials • If on NPH 40 units BID __ vials

Insulin Vials • 1 m. L = 100 units of insulin • 10 m. Ls = 1 vial = 1000 units of insulin • If a patient is on 10 units of insulin per day will use 300 units per month and 900 units every 3 months 1 vial • If on 50 units/day 1500 units/month 4500 units/3 months 5 vials • Shortcut: for every 10 units/day of insulin, need to prescribe 1 vial • If on Glargine 60 units/day 6 vials • If on NPH 40 units BID __ vials

Insulin Vials • 1 m. L = 100 units of insulin • 10 m. Ls = 1 vial = 1000 units of insulin • If a patient is on 10 units of insulin per day will use 300 units per month and 900 units every 3 months 1 vial • If on 50 units/day 1500 units/month 4500 units/3 months 5 vials • Shortcut: for every 10 units/day of insulin, need to prescribe 1 vial • If on Glargine 60 units/day 6 vials • If on NPH 40 units BID 8 vials

Case 8 42 F with poorly controlled DM who comes in for follow up. Her last A 1 c recently came back at 11. 2. Looking back, her A 1 c has ranged from 9. 9 -12 over the last 3 years. She is on Glargine 50 units BID and Lispro 10 units TIDAC. She didn’t bring in her FS log or her medications, though says her sugars run between 110 -110 s in the morning before breakfast. You decide to: A. Increase her Glargine from 50 to 55 units BID B. Increase her Lispro from 10 to 15 units TIDAC C. A and B D. None of the above

Case 8 42 F with poorly controlled DM who comes in for follow up. Her last A 1 c recently came back at 11. 2. Looking back, her A 1 c has ranged from 9. 9 -12 over the last 3 years. She is on Glargine 50 units BID and Lispro 10 units TIDAC. She didn’t bring in her FS log or her medications, though says her sugars run between 110 -110 s in the morning before breakfast. You decide to: A. Increase her Glargine from 50 to 55 units BID B. Increase her Lispro from 10 to 15 units TIDAC C. A and B D. None of the above

Converting A 1 c to Mean Glucose • A 1 c of 7 translates to an average glucose of ~ 150 Hb A 1 c Mean Glucose 7 150 8 180 9 210 10 240 11 270 12 300

What to Do for Chronically Uncontrolled DM • Simplify regimen! • Less is more – daily or BID regimens shown to improve adherence • Primary goal is to get fasting sugars to goal – long-acting insulin alone can bring A 1 c down to ~ 8 • It takes more than medicine • • Build rapport - create supportive, non-judgmental environment Ensure patient can see and read Ask about home life, stressors, support systems Enlist support systems, family members – have them come in Address social determinants of health (housing, food, transportation, etc) Screen for mood disorders Ensure patient knows how to check FS and inject insulin properly Utilize available DM resources

DM Resources • RN visits for FS log review and DM teaching • DM Education Classes – series of 2 classes, run by Nutritionist • Group DM Class – run by NP Jackie; group visits for DM education and medication management • Nutrition referral • Weight loss classes • Taking Control Study
 • Best stored inside the fridge")
Insulin Storage • Unopened insulin (vials or pens) • Best stored inside the fridge • Last until expiration date (usually 1 year) • Opened insulin • Vials • Can be stored in fridge OR at controlled room temperature • Should be injected only when at room temperature • Regardless of where stored, open insulin good for 28 days • Pens • Store in controlled room temperature • Pens last 7 -28 days (depending on the pen)

Case 9 Mr. Shore Tacting is a 55 M with DM, A 1 c initially 14, now down to 8. 4 with significant lifestyle changes and Glargine 52 units q. HS. He brings in his FS log, which shows AM pre-prandial FS of 81 -122. He denies hypoglycemic events. You decide together that his A 1 c goal is 7. What is your next step in management? • A. Step away from patient – A 1 c 8. 2 is good enough • B. Increase Glargine to 55 units • C. Start Lispro 5 units TIDAC • D. Discuss with patient whether feasible to check FS 2 hours after largest meal, in anticipation of starting Lispro if glucose > 180

Case 9 Mr. Shore Tacting is a 55 M with DM, A 1 c initially 14, now down to 8. 4 with significant lifestyle changes and Glargine 52 units q. HS. He brings in his FS log, which shows AM pre-prandial FS of 81 -122. He denies hypoglycemic events. You decide together that his A 1 c goal is 7. What is your next step in management? • A. Step away from patient – A 1 c 8. 2 is good enough • B. Increase Glargine to 55 units • C. Start Lispro 5 units TIDAC • D. Discuss with patient whether feasible to check FS 2 hours after largest meal, in anticipation of starting Lispro if glucose > 180

When/How to Start Short-Acting Insulin in DM 2 • Experiences with short-acting insulin • Only start short-acting insulin if: • AM pre-prandial FS at goal • A 1 c not at goal • Patient willing and able to intensify regimen • If patient meets this criteria, ask patient to check FS 2 hours after largest meal • If post-prandial FS consistently above 180, can consider short-acting insulin • Typically, Regular insulin if on NPH and Lispro/Aspart, if on Glargine • Lispro/Aspart: ~ immediate onset, peak in 30 -90 mins (so need to be taken with meals) • Regular: 30 -60 min onset, peak in 2 -3 hours (ideally given 30 mins before a meal) • Continue up-titration until 2 hour post-prandial FS < 180 and once at goal, check A 1 c • If A 1 c still not at goal, ask patient whether willing to check FS 2 hours after second largest meal. • Again, start short acting insulin if FS consistently above 180 and up-titrate until FS < 180. • Repeat…

Case 10 Ms. Hipog Licemya is a 68 F with DM, on U 500 insulin-R 32/28/22 units. Her last A 1 c is 8. 1. She comes in today with her FS log, which shows AM pre-prandial FS of 91 -144 with 3 episodes in the last week of FS between 50 -65. What is your next step in management? • A. Stop U 500 insulin – switch to R U 100 insulin • B. Increase U 500 insulin – A 1 c is above goal • C. Don’t change U 500 – just ask patient to eat more carbs • D. Ask more about hypoglycemic events – this is serious

Case 10 Ms. Hipog Licemya is a 68 F with DM, on U 500 insulin-R 32/28/22 units. Her last A 1 c is 8. 1. She comes in today with her FS log, which shows AM pre-prandial FS of 91 -144 with 3 episodes in the last week of FS between 50 -65. What is your next step in management? • A. Stop U 500 insulin – switch to R U 100 insulin • B. Increase U 500 insulin – A 1 c is above goal • C. Don’t change U 500 – just ask patient to eat more carbs • D. Ask more about hypoglycemic events – this is serious

Hypoglycemia • Lots of data about risks of hypoglycemia • Ask about illness, skipped meals, food insecurity, other social stressors • Decrease insulin by 2 -4 units or 10 -20% if not due to reversible cause (i. e illness)

Seligman, Optimizing Care for Patients with Food Insecurity, 3/2/18

Seligman, Optimizing Care for Patients with Food Insecurity, 3/2/18

Seligman, Optimizing Care for Patients with Food Insecurity, 3/2/18

Seligman, Optimizing Care for Patients with Food Insecurity, 3/2/18

Seligman, Optimizing Care for Patients with Food Insecurity, 3/2/18

Seligman, Optimizing Care for Patients with Food Insecurity, 3/2/18

Seligman, Optimizing Care for Patients with Food Insecurity, 3/2/18

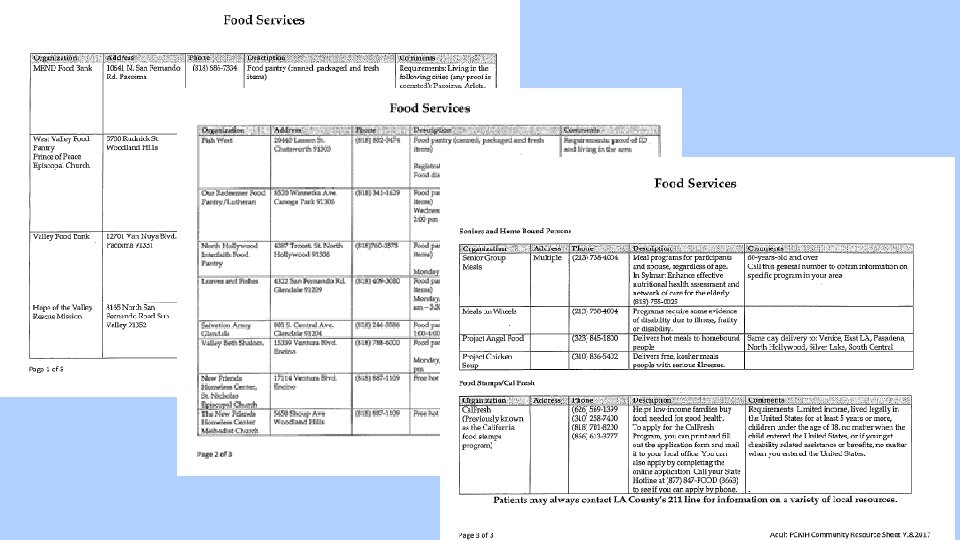
Resources for Food Insecurity • Food Services Resource Sheet • SNAP/Cal. Fresh – food stamps • Underutilized (50% of eligible Californians not enrolled • Elder nutrition programs – Meals on Wheels • Food Pantries • Soup kitchens, etc
 insulin resistance • After 200")
U-500 Insulin • For patients with very high (syndromic) insulin resistance • After 200 units insulin/day, the dose response to further insulin administration is attenuated • If on Glargine 100 units BID, will be injecting 1 m. L of insulin BID… • Variable absorption and injection site discomfort • 5 times more concentrated than U 100 insulin (so injecting less volume) • Only available as Regular form of insulin • Pharmacokinetic profile more closely simulating NPH than regular U-100 • Risk of severe hypoglycemia and weight gain


U-500 • Meta-analysis of studies using U 500 insulin • • • Reviewed 9 studies, 310 patients, all but one retrospective, mean F/U 6 -36 months. Most required > 200 units of U 100 insulin Mean A 1 c reduction with U 500 of 1. 6% 4. 4 kg weight gain Severe hypoglycemia “either not reported to be a problem or was no more frequent than with U 100 R use. ” Slight increase in mild hypoglycemia within first few months • One study with significant increase in hypoglycemia (13 -42%) • Improved quality of life, patient satisfaction, time spent in DM management • Decreased cost • “More extensive studies using continuous glucose monitoring are needed to better understand hypoglycemia risk. Prospective evaluation…is critical to better understand issues of efficacy and safety” • Patient selection, education unclear • Clearly not for everyone • Should only be prescribed by Endocrine or DM expert • Requires significant amount of education to ensure correct prescribing/administration

Questions?

Inpatient DM Management

NICE-SUGAR Trial • NEJM, 2009 • Randomized 6 K patients in ICU to intensive glucose control (goal 80108) vs goal < 180 • Multicenter, non-blinded RCT • Intensive glycemic control group had higher 90 day mortality and more hypoglycemic events than control group • 27. 5% vs 24. 9%, P=0. 02 (90 day mortality) • 6. 8% vs 0. 5% glucose < 40

RABBIT 2 Trial • Journal o • In non-critically ill patients with DM 2, is basal-bolus insulin more effective and safer than sliding scale insulin? • N=130, multicenter, RCT • Patients insulin-naïve with DM for 3+ months, FS 140 -400 on admission • Baseline characteristics: age 56, 65% male, 66% AA, LOS 5 days, average blood glucose on admission 230, A 1 c 8. 9 • Randomized to basal-bolus vs SSI • Target fasting and pre-meal FS < 140

RABBIT 2 Trial • Basal bolus regimen: if FS between 140 -200, total 0. 4 units/kg insulin given • Glargine qday (50% of total dose) with short-acting TID given in 3 equal doses (tot 50% of total dose) • If not eating, short-acting not given • If fasting FS > 140, Glargine increased by 20%; if fasting FS < 70, decreased 20% • SSI given to patient with pre-meal glucose > 140 • SSI regimen: • • If unable to eat, given Regular insulin q 6 hours If able to eat, given Regular insulin before each meal and at bedtime If fasting / pre-meal FS > 140, SSI dosing inceased; if < 70, dose decreased If mean daily FS > 240 on max SSI regimen, switched to basal-bolus 0. 5 units/kg
 vs 165 (SSI) (p<0. 01)")
RABBIT 2 Trial • Mean fasting glucose: 147 (BB) vs 165 (SSI) (p<0. 01) • Mean random glucose: 164 (BB) vs 189 (SSI) (p<0. 01 • Hypoglycemia (< 60): 2 vs 2 • Length of stay the same. Not powered for mortality or difference in clinical outcomes.

ADA-Recommended Diabetic Diet • Carbohydrates • Increase fruits, vegetables, whole grains, legumes, dairy products, fiber • Limit “bad” carbs (high glycemic index) in favor of carbs with low glycemic index • Limit soda/juices, alcohol, fast food • Fats • Ideal fat intake is unknown • Mediterranean diet (with monounsaturated fatty acids) improves glycemic control and may decrease CV risk • Plant based, olive/canola oil, fish/poultry instead of red meat

Classification of Foods Based on Glycemic Index Asif, 2014
- Slides: 67