NSAIDs Rheumatoid Arthritis Osteoarthritis A Case Approach Bobo

NSAIDs, Rheumatoid Arthritis, & Osteoarthritis: A Case Approach Bobo Tanner MD Rheumatology & Allergy Monday Feb 19, 2007 VMS IV

AGENDA • • • Differentiate RA & OA Therapeutic Choices Case based examples Treat Early & Monitor for Benefit & Side Effects

Case 1 65 -year-old man: knee pain that began insidiously about a year ago. No other rheumatic symptoms. PMHx: PUD, ischemic heart dz, sulfa allergy • • • What further questions should you ask? What are the pertinent physical findings? Which diagnostic studies are appropriate?

Inflammatory vs. Mechanical RA History & PE • AM stiffness >1 hr. • Symmetrical swelling, tenderness: wrists, MCPs, PIPs Labs • 45 -85% +RF, +CCP Ab ESR, C-RP, Hct X-rays • JSN • erosions OA History & PE • Worse pain w/activity • DIPs, 1 st CMC, wt. bearing jts. Labs • Medication monitoring CBC, BMP, UA X-rays • Osteophytes, asymmetry, sclerosis

Therapeutic Options RA NSAIDs Corticosteroids DMARDs Biologic DMARDs Also: Joint Injections PT/OT Surgery SLE Steroids Anti-malarial Immunosuppressive OA Analgesics NSAIDs Also: Joint injections PT/OT Surgery Nutritional supplements
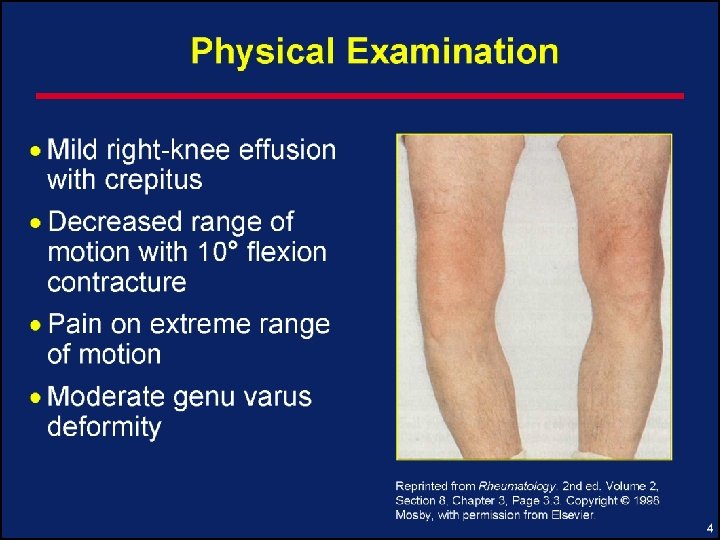

Case 1: Radiographic Features • Asymmetric joint space narrowing • Marginal osteophytes • Subchondral cysts • Bony sclerosis • Malalignment • NAILS THE DIAGNOSIS

OA: Risk Factors • Why did this patient develop osteoarthritis?
 • • Age: 75% of persons over age 70 have")
OA: Risk Factors (cont’d) • • Age: 75% of persons over age 70 have OA Female sex Obesity Hereditary Trauma Neuromuscular dysfunction Metabolic disorders

Case 1: Cause of Knee OA • On further questioning, patient recalls a serious knee injury during high school football • Therefore, posttraumatic OA is most likely diagnosis

Pharmacologic Management of OA • • • NSAIDs Non-opioid analgesics Topical agents Opioid analgesics Intra-articular agents Unconventional therapies

NSAIDs • • • Inhibit prostaglandin synthesis & other Account for ½ the Rx in the elderly If no response to one may respond to another Lower doses may be effective Do not retard disease progression
 • Side effects: GI, renal, cardiac, edema • Severe side effects <5%,")
NSAIDs (cont’d) • Side effects: GI, renal, cardiac, edema • Severe side effects <5%, but large numbers of users • Gastroprotection increases expense • Antiplatelet effects may be hazardous • GI tolerance much better with COX-2 • C-V events overshadow COX-2

Non-opioid Analgesic Therapy • Acetaminophen • • Pain relief comparable to NSAIDs, less toxicity Beware of toxicity from use of multiple acetaminophen-containing products Maximum safe dose = 4 grams/day Lifetime dose & toxicity?

Ibuprofen vs Acetaminophen for Knee OA—Equivalent Benefit * P<. 05 Bradley, et al. N Engl J Med. 1991; 325: 87– 91.

Celecoxcib vs Acetaminophen for Hip & Knee OA—Pincus data PACES trial Patient preferences: • 53% celecoxib (200 mg) vs 24% acetaminophen(4 gm) PACES-a (p<0. 001) • 37% acetaminophen v 28% placebo in PACES-a (p = 0. 340) Ann Rheum Dis. 2004 Aug; 63(8): 931 -9

OA: Nutritional Supplements • Polysulfated glycosaminoglycans— nutriceuticals • Glucosamine +/- chondroitin sulfate: Symptomatic benefit, no known side effects, long-term controlled trials pending

Knee Injection • Knee fully extended • Junction upper third and lower two thirds of the patella • Insert needle under patella and aim superiorly © ACR

OA: Intra-articular Therapy • Intra-articular steroids • • Hyaluronate injections* Pain relief Up to q 3 mo Risks: infection, worsening diabetes, or CHF • Joint lavage • Symptomatic benefit demonstrated * Altman, et al. J Rheumatol. 1998; 25: 2203. • • Synvisc ® , Hylgan® Symptomatic relief Improved function $$$$$$$ Series of injections, fail steroids first? No evidence of longterm benefit Knees, other?

Strengthening Exercise for OA • Decreases pain and increases function • Physical training rather than passive therapy • General program for muscle strengthening Warm-up with ROM stretching • Step 1: Lift the body part against gravity, begin with 6 to 10 repetitions • Step 2: Progressively increase resistance with free weights or elastic bands Rogind, et al. Arch Phys Med Rehabil. 1998; 79: 1421– 1427. • et. Cool-down with 1999; 89: 66– 72. ROM stretching Jette, al. Am J Public Health. •

Surgical Therapy for OA • Arthroscopy • • • May reveal unsuspected focal abnormalities Results in tidal lavage Expensive, complications possible • Osteotomy: May delay need for TKR for 2 to 3 years • Total joint replacement: for severe pain and function significantly limited


Case 2: Rheumatoid Arthritis • 53 -year-old woman with 6 months history of RA sx • Morning stiffness = 30 minutes • Synovitis: 1+ swelling of MCP, PIP, wrist, and MTP joints • Normal joint alignment • Rheumatoid factor positive, anti-CCP + • No erosions seen on x-rays

Rheumatoid Arthritis: Treat Early & Prevent Damage & Dysfunction • Ulnar deviation of R hand • MCP & PIP swelling • synovitis of left wrist • Joint space narrowing & erosions on x-ray • Synovial thickening feels like a firm sponge
 • Assessment • Rheumatoid Arthritis • No sign of damage •")
Case 2 (cont’d) • Assessment • Rheumatoid Arthritis • No sign of damage • Treatment • NSAID, steroid, DMARD • Education + ROM, conditioning, and strengthening exercises Which DMARD would you choose?

Rheumatoid Arthritis: Drug Treatment Options • NSAIDs – Symptomatic relief, improved function – No change in disease progression • Low-dose prednisone (£ 10 mg qd) – If used long term, consider prophylactic treatment for osteoporosis • Intra-articular steroids – Useful for flares Paget. Primer on Rheum Dis. 11 th edition. 1997: 168.
 – Hydroxychloroquine (Plaquenil®) • Modest effect, low")
Rheumatoid Arthritis: • Disease modifying drugs (DMARDs) – Hydroxychloroquine (Plaquenil®) • Modest effect, low toxicity – Sulfasalazine • Moderate effect, monitor like MTX – Methotrexate • Most effective single DMARD • Good benefit-to-risk ratio – Leflunomide (Arava®) • Effect & side effects similar to MTX • Combinations Alarcon. Rheum Dis Clin North Am. 1998; 24: 489– 499. Paget. Primer on Rheum Dis. 11 th edition. 1997: 168.

Rheumatoid Arthritis: Monitoring Treatment With DMARDs • These drugs need frequent monitoring • Blood, liver, lung, kidney, skin are frequent sites of adverse effects • √ CBC, LFTs, creatinine, urine • Lab intervals: 4 to 12 weeks commonly • Most patients need to be seen 3 to 6 times a year
 50 mg SQ weekly – Infliximab (Remicade®) IV")
Biologic DMARDs Anti-TNF – Etanercept (Enbrel®) 50 mg SQ weekly – Infliximab (Remicade®) IV q 8 weeks – Adalimumab (Humira®) 40 mg SQ QOW – Rapid onset, effective in refractory patients with and w/o MTX, halts bone erosions – Screen for Tb, infections, expensive Also – Anakinra (Kineret®), daily SQ, inj. anti-IL-1 – Abatacept (Orencia®), IV monthly , T cell 2 nd sig. – Rituximab ( Rituxan®) IV x 2, TNF failure, B cells Fleischmann. Rheum Dis Clin North Am. 2006; 32(1): 21 -28.

Early Intervention Is Effective in RA • Several studies collectively provide clear evidence that delayed use of DMARD therapy in RA may adversely affect clinical and radiographic outcomes • Treatment should be initiated within months of the diagnosis, not years

Short Delay of Therapy Affected Joint Damage 14 12 10 Delayed Treatment = median 123 days 8 Joint 6 Early Treatment = median 15 days Damage 4 2 0 0 6 12 Time (months) Lard LR, et al. Am J Med. 2001; 111: 446 -451. 18 24

Clinical Parameters Don’t Correlate with Bone Damage 75 Percentage 50 improvement 25 0 – 25 Percentage deterioration – 50 Grip strength Sedimentation rate Ritchie articular index Morning stiffness Pain VAS Hemoglobin Radiological score – 75 VAS = 10 cm visual analogue scale. Mulherin D, et al. Br J Rheumatol. 1996; 35: 1263 -1268.

Case 2 • Which DMARD would you choose? • Monitor : Clinically Labs X-rays

Case 3 • 68 -year-old woman, 3 -years of RA , squeezed into your schedule as a new patient • 4 weeks of increasing fatigue, dizziness, dyspnea, and anorexia • Joint pain and stiffness: mild & unchanged • Meds: flare up 4 mos. ago , switched to naproxen and prednisone
 • Past history: Peptic ulcer 10 years ago, mild hypertension •")
Case 3 (cont’d) • Past history: Peptic ulcer 10 years ago, mild hypertension • Exam: thin, pale apathetic woman with Temp 98. 4ºF, BP 110/65, pulse 110 bpm • Symmetrical 1+ synovitis of the wrist, MCP, PIP, and MTP joints • Heart, lungs, and abdomen: unremarkable
 • The doctor is falling behind in the schedule • What")
Case 3 (cont’d) • The doctor is falling behind in the schedule • What system must you inquire more about today? A. Cardiovascular B. Neuropsychological C. Endocrine D. Gastrointestinal
 • Clues of impending disaster • • High risk for NSAID")
Case 3 (cont’d) • Clues of impending disaster • • High risk for NSAID gastropathy Presentation suggestive of blood loss • • • Pale, dizzy, weak Tachycardia, low blood pressure No evidence of flare in RA to explain recent symptoms of increased fatigue
 • NSAID gastropathy is sneaky and can be fatal Don’t Miss")
Case 3 (cont’d) • NSAID gastropathy is sneaky and can be fatal Don’t Miss It

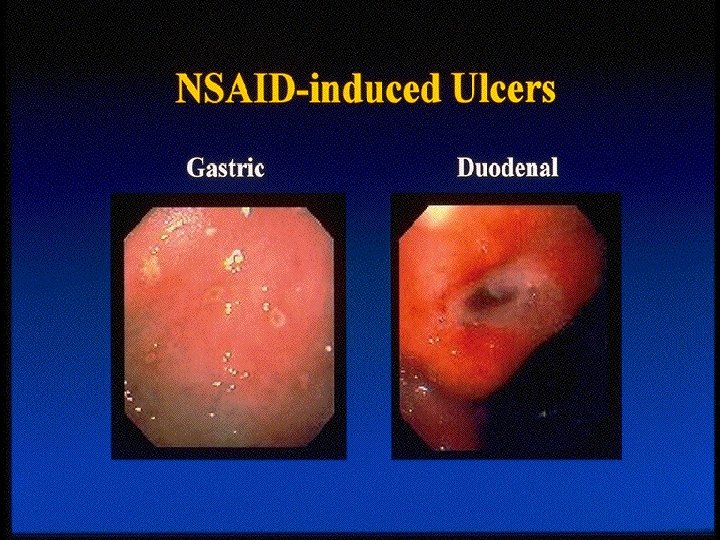
NSAID Gastropathy • Gastric ulcers are more common than duodenal ulcers • No reliable warning signs • 80% of occur without prior symptoms • Ulcers in RA 2. 5 - 5. 5 times more than general population • 107, 000 hospitalized & 16, 000 deaths annually due to NSAID-GI complications Singh. Am J Med. 1998; 105(suppl B): 31 S– 38 S.

NSAID Gastropathy: Key Points Know the risk factors • The best way to treat it is to prevent it • • Avoid it: Use acetaminophen, salsalate, (or ? selective COX-2 inhibitor) Counteract it: PPI or prostaglandin analogue • Antacids and H 2 blockers are not the answer • May mask symptoms but do not prevent serious events

GI Risk Factors : NSAID Ulcers • Older age • Prior history of peptic ulcer or GI symptoms with NSAIDs • Concomitant use of prednisone • NSAID dose • Disability level: The sicker the patient the higher the risk Singh. Am J Med. 1998; 105(suppl B): 31 S– 38 S.

Balancing NSAID Efficacy and Safety • Antiinflammatory activity • Analgesia • • • GI toxicity • Renal toxicity • Platelet effects Is NSAID therapy indicated? Can low dose relieve symptoms? Risk of complications ? Consider NSAID therapy with reduced GI toxicity or combination Rx with GI med

Selective COX-2 Medications • VIOXX® : withdrawn from market 9/30/04 • Celebrex® • Bextra® withdrawn 2005 also associated with cardiovascular dz, hypertension, edema and sulfa & skin rxns

COX-2 Selective NSAIDs • A replacement for non-selective NSAIDs? • • • Pain relief equivalent to older NSAIDs Less GI toxicity (rofecoxcib) No effect on platelet aggregation or bleeding time Cost similar to generic NSAIDs plus proton pump inhibitor or misoprostol Side effects: Cardio-Vascular, BP, edema Medical Letter. 1999; 41: 11– 12.
 Time in study WSJ 10/1/04")
COX-2 : CV events (rofecoxcib) Time in study WSJ 10/1/04

Case 4 • 52 -year-old man with destructive RA • Rx NSAID & low-dose prednisone • MTX & Remicade( anti-TNF) started 4 months ago • 3 -week history of fever, dry cough, and increasing shortness of breath • Exam: Low-grade fever, fine rales in both lungs, • Labs: normal CBC , LFTs, low alb • Chest xray: bilat. interstitial infiltrates
 • What should be done? A. Culture, treat with antibiotic for")
Case 4 (cont’d) • What should be done? A. Culture, treat with antibiotic for bacterial pneumonia B. Place PPD, sputum for AFB C. Give steroids for hypersensitivity pneumonitis and stop methotrexate D. Give a high-dose steroids and increase methotrexate for rheumatoid lung

DMARDs & Biologics Have a Dark Side Methotrexate may cause serious problems Lung Liver Bone marrow Anti-TNF (Remicade, Enbrel, Humira) assoc. with TB reactivation and other infections Don’t Miss It

Case 5 • A pre-op physical has been ordered for a routine cholecystectomy on a 43 -year-old woman with RA since age 20 • PMH: bilateral THR , left TKR • Meds: NSAID, 5 mg/d prednisone, MTX • General physical exam normal • MS exam, extensive deformities, mild synovitis • In addition to routine tests, what test should be ordered before surgery?

Subluxation of C 1 on C 2 RA can cause asymptomatic instability of the neck Manipulation under anesthesia can cause spinal cord injury Don’t Miss It

Clues for C 1 -C 2 Subluxation • Long-standing rheumatoid arthritis or JRA • May have NO symptoms • C 2 -C 3 radicular pain in the neck and occiput • Spinal cord compression • • Quadriparesis or paraparesis Sphincter dysfunction Sensory deficits TIAs secondary to compromise of the vertebral arteries Anderson. Primer on Rheum Dis. 11 th edition. 1997: 161.
 from mechanical (OA) • Treat RA early •")
Summary • Distinguish Inflammatory Disease (RA) from mechanical (OA) • Treat RA early • Know the medication side effects • Know the complications of the disease

One Last Word: Unconventional Therapies • Keep in touch with current information. The unconventional may become conventional • • • www. quackwatch. com ACR Website (www. rheumatology. org) Arthritis Foundation Website (www. arthritis. org)
- Slides: 56