NPLEX Combination Review Concepts in Pharmacology Pharmacognosy and

NPLEX Combination Review Concepts in Pharmacology, Pharmacognosy and Nutrition Paul S. Anderson, ND Medical Board Review Services Copyright MBRS

Review Synopsis: • *With the exception of the introductory section, each organ system will be integrated in the manner the cases will likely come on the Board Exams: ================== GENERAL SCHEDULE: – Introduction through Pulmonology / Hematology – Hematology through Neurology – Emergency Medicine through Dermatology / Gastro – Gastro through GYN

Pharmacodynamics and Pharmacokinetics

They are reactions between the body, the drug and possibly other substances that can potentially affect the availability and usefulness of the drug administered.

Pharmacology of Interactions: • Pharmacokinetic Reactions – Absorption – Distribution • Additive to or Displacing from Albumen • Cellular Effects – Distribution / Receptor Activity – Metabolism – Elimination • Pharmacodynamic Reactions – Antagonist – Synergist / Additive / Agonist
 suffer")
Interactions: Absorption • p. H Alteration – Drugs that require ionization (Antifungal, Minerals) suffer in higher p. H gastric environments. • Direct Blockade – Binding / Chelating agents • GI Motility Alteration – Increased motility = Increased absorption – Decreased motility = Decreased absorption – (To a point).

Interactions: Distribution • Albumen Effects – Most drugs / Hormones are transported on albumens – The “Free” portion (unbound) is the bio-available portion – Substances that increase binding DECREASE availability of drug to tissues – Substances that decrease binding INCREASE availability of drug to tissues • Cellular Effects – Distribution / Receptor activity • Actions by one substance on another substance at the receptor level. • May include displacement from cellular binding site • May include receptor blockade • May include enzyme modification (common with poisons)

Interactions: Metabolism • Induction Errors – Substances that INDUCE hepatic metabolism REDUCE plasma availability of the drug • Inhibition Errors – Substances that SLOW hepatic metabolism INCREASE plasma availability of the drug • Substrate Errors – Some substances supply substrate for the hepatic detoxification pathways – These substances induce metabolism, REDUCING plasma availability
 Pathways: Generally render Non-polar (Lipid Soluble) substances")
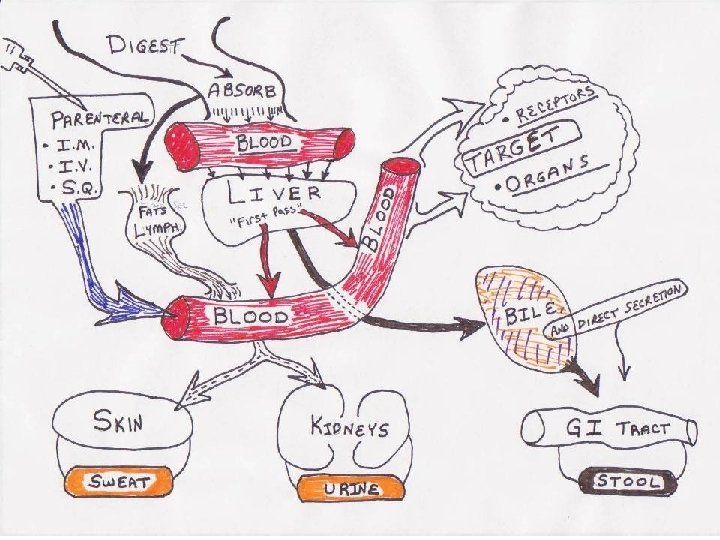
Hepatic Detoxification Pathways: PHASE-1 (Cytochrome P 450) Pathways: Generally render Non-polar (Lipid Soluble) substances Polar Reactions: Oxidation, Reduction, Hydrolysis, Hydration… Co-factors / Substrates: B 2, 3, 6, 12, Folate, GSH, AA’s… This process NATURALLY creates peroxide and superoxide free radicals! PHASE-2 (Conjugation) Pathways: Take intermediary (more-polar) P 450 metabolites and conjugate them with Amino Acids. EXCRETION: BILE SERUM URINE
 Phase-2 Water")
LIVER DETOXIFICATION PATHWAYS Fat – Soluble Compounds Phase-1 CYP 450 (-OH added) Phase-2 Water – Soluble compounds Enzymatic Conjugation Excreted derivatives Glycine Hippurates Glutathione Mercapturates Glucuronic Acid Glucuronides Natural creation of Hydroxyl and Superoxide Radicals leading to Lipid Peroxidation.

Interactions: Elimination • Kidney Clearance Issues: – Reduced GFR can result in Increased plasma levels of RENALLY CLEARED DRUGS. – Increased GFR will cause lower effect of chronically prescribed drugs, due to increased excretion.

Calculated GFR Changes and drug elimination considerations: • Healthy Kidneys: 60 or higher • Stage 1 Chronic Kidney Disease (CKD): – 90 or higher with HTN, Proteinuria, Ab. N Ki anatomy • Stage 2 Chronic Kidney Disease (CKD): – 60 -89 with the above • Stage 3 Chronic Kidney Disease (CKD): – 30 -59 • Stage 4 Chronic Kidney Disease (CKD): – 15 -29 • Stage 5 – 15 or less / Dialysis

The Bottom Line: • Use caution applying typical dosing for substances in patients with any pathologic alteration in the physiologic parameters of drug metabolism: – Kidney disease – Liver disease – GI disease – Any patient over 65

Interactions: Antagonist • Antagonistic Pharmacologic Properties – Must have opposite actions of drugs at same time – Different sites of action in the body – Drugs of equal strength (of action) will have uniform antagonism – Unequal antagonism will favor the stronger acting drug.

Interactions: Synergist / Additive / Agonist • Additive effects of drugs • May have: – Common receptor activity • I. e. Alcohol and Benzodiazepines – Synergistic receptor activity • I. e. H-1 Blockers and Skeletal Muscle Relaxants

Half Life • The biological half-life of a substance is the time required for half of that substance to be removed from an organism by either a physical or a chemical process. • Biological half-life is an important pharmacokinetic parameter and is usually denoted by the abbreviation t-1/2.

Half Life and Elimination • First-order elimination Fast. This process is usually a first-order logarithmic process - that is, a constant proportion (percent) of the agent is eliminated per unit time.

Half Life and Elimination • In practice, this means that it takes just over 4. 7 times the half-life for a first order eliminated drug's serum concentration to reach steady state after regular dosing is started, stopped, or the dose changed. – “The 5 X rule” • So, for example, digoxin has a half-life (or t½) of 2436 hours; this means that a change in the dose will take the best part of a week to take full effect. • For this reason, drugs with a long half-life (e. g. amiodarone, elimination t½ of about 90 days) are usually started with a loading dose to achieve their desired clinical effect more quickly.

First Order Elimination. Concentration after stopping the drug plotted over time: 1 t½ 2 t½ 3 t½ 4 t½ 5 t½

Peak and Trough Repeated doses give a “steady state” of drug in the system which is not linear, it has peaks and troughs based on elimination dynamics of the drug and the body. This timing is also important in drugs that require lab levels for monitoring.

Half Life and Elimination • Zero-order elimination Slow. There are circumstances where the half-life varies with the concentration of the drug. – First-order kinetics is to be distinguished from zeroorder kinetics, in which a constant amount (rather than percent) of drug is eliminated during each unit of time. Zero-order processes imply that the clearance mechanism has been saturated or overloaded. – For example, Aspirin, Phenytoin (High Dose IV Vitamin C) and Ethanol may be consumed in sufficient quantity to saturate the metabolic enzymes in the liver, and so is eliminated from the body at an approximately constant rate (zero-order elimination).
 – Saturable quality of")
Half Life and Elimination • Michaelis – Menten (and Hill) – Saturable quality of Enzyme reactions: – Estimating the speed of enzymatic reaction based on [substrate. ] – Once the enzyme system is saturated (by substrate) the kinetics (e. A) change (First order to Zero order elimination. )
 Saturable quality of Enzyme reactions: Estimating the speed of")
Michaelis – Menten (and Hill) Saturable quality of Enzyme reactions: Estimating the speed of enzymatic reaction based on [substrate. ] Once the enzyme system is saturated (by substrate) the kinetics (e. A) change (First order to Zero order elimination. ) Shows drug in and drug out over time, initially as first order. Once the enzymatic elimination pathways are saturated the kinetics of elimination (and build-up) in the body change to zero order, often causing overdose. Vmax Maximum elimination under MM kinetics:

DRUG INTERACTIONS / SIDE EFFECTS Increase plasma drug level Decrease plasma drug levels Increase plasma drug levels

DRUG INTERACTIONS / SIDE EFFECTS - 2

DRUG INTERACTIONS / SIDE EFFECTS - 3 Gent. , Tobra. , and Streptomycin Antidepressants should not be combined due to possible additive effects, but often are now prescribed in combination.

DRUG INTERACTIONS / SIDE EFFECTS - 4

DRUG INTERACTIONS / SIDE EFFECTS - 5

• Physiologic Actions Prefix recognition: – Cholinergic: • Muscarinic • Nicotinic jct. – Adren___ • Beta 1&2 • Alpha 1&2 Acetylcholine receptor. Found at postsynaptic parasympathetic locations Autonomic ganglia. Adrenal medulla. Neuromuscular “Adrenal acting” (Epi. N. E. ) acting receptor: Cardio-pulmonary postsynaptic sympathetic GI, Vascular, CNS presynaptic sympathetic • Suffix recognition: – __mimetic: Mimics / acts like the physiologic substance. • I. e. Sympathomimetic substances – __lytic Blocks the action of the physiologic substance. • I. e. Parasympatholytic substances • Receptor activity: – Agonist: – Antagonist: Stimulates that receptor to action. Blocks that receptor from action.

Autonomic Nervous System Activity: • Sympathetic N. S. • Parasympathetic N. S. – Generally stimulating – GI & GU Tract Depressing • Sympathomimetic – Drug (i. e. Epinephrine) that acts at one or more sympathetic receptor site. – Actions of the drug mimic sympathetic activity to the extent that receptors are activated • Sympatholytic – Drug (i. e. Reserpine) that blocks or otherwise decreases catecholamines. Thus increasing some parasympathetic tone. – Generally relaxing – GI & GU Tract Stimulating • Parsympathomimetic – Drug (i. e. Pilocarpine) that acts at one or more parasympathetic receptor site. – Actions of the drug mimic parasympathetic activity to the extent that receptors are activated • Parasympatholytic – Drug (i. e. Atropine) that blocks one or more parasympathetic receptor sites. – Actions of the drug effectively block parasympathetic activity and thus increase some sympathetic tone.

Excitable Membrane Physiology The resting membrane potential is predicated on the ionic balance between the ICF and the ECF. Changes in those ion concentrations create AP generation and cellular activation. ICF ECF [Na] [K] [Na] [Mg] [Ca] Cl(Cl- influx hyperpolarizes the cell, inactivating it. )
 RECEPTORS")
CHOLINERGIC (ACh) RECEPTORS
 CHANNEL (A Ligand Gated Ion Chanel)")
THE ACETYLCHOLINE (ACh) CHANNEL (A Ligand Gated Ion Chanel)

Acetylcholine • Multiple sites of action in the body – Acts as a neurotransmitter (PNS / CNS) – Acts as a hormone (Cornea) • Peripherally acts at the neuromuscular junction, and elsewhere via Nicotinic and Muscarinic receptors • Centrally seems to be involved in memory and other neurological counter regulation
![Acetylcholine Metabolism SERINE Pyruvate Phosphatidylethanolamine SAMe Betaine [Folate / B 3 / B 6]](http://slidetodoc.com/presentation_image_h2/db01fba359d161188ca9a7f491da932f/image-36.jpg "Acetylcholine Metabolism SERINE Pyruvate Phosphatidylethanolamine SAMe Betaine [Folate / B 3 / B 6]")
Acetylcholine Metabolism SERINE Pyruvate Phosphatidylethanolamine SAMe Betaine [Folate / B 3 / B 6] SAMh Phosphatidylcholine Acetate [B 2 / B 5 / B 6] Acetyl-Co. A Choline [Choline Acetylase] Acetylcholine (ACh) Diet [Acetylcholine esterase] Choline Acetate
 RECEPTORS")
ADRENERGIC (Epi. / NE) RECEPTORS

Plant Medicine Prototypes - 1 • Rauwolfia serpentina – Acts by decreasing activity of neuronal storage vessicles. • CNS: Decreases Catecholamines • PNS: Decrease Norepinephrine and Serotonin • Digitalis lanata (leaf) – Decreases aberrant SA to AV conduction • Positive Inotrope and Dromotrope – Blockade of Na/K ATPase pump (Increases intracellular Ca. results in elongated plateau on cardiac AP) – Improves atrial dysfunction • Chincona (bark) – Two primary chincona alkaloids: – Mild to moderate anticholinergic effects, direct toxic effects. • Quinine (Anti spasmodic [noctournal leg cramps], antipyretic, Ameobacide) • Quinidine (Antiarrhythmic) • Atropa belladonna – Acetylcholine antagonist (Parasympatholytic) • Muscarinic receptor blocade (Post-synaptic parasympathetic) • Slows digestion, decreases secretions, dilates pupils…
 – Physostigmine • Reversible inhibition of")
Plant Medicine Prototypes - 2 • Calabar (bean) – Physostigmine • Reversible inhibition of Acetylcholine Esterase • Increases Acetylcholine levels (Parasympathomimetic) – Increases secretions, digestion, constricts pupils… • Pylocarpus mycrophyllus / jaborandi – Pilocarpine • Cholinergic (Parasympathomimetic) • Used as eye drop in glaucoma treatment • Erythroxylon coca – Cocaine • Dilates pupils • Anesthetic to mucous membranes • Increases Dopamine (reuptake inhibition) especially active in the nucleus accumbuns / pleasure centers.

Plant Medicine Prototypes - 3 • Eschscolizia californicum – California poppy • Used in pain control tincture formulas etc. • Papaver somniferum – Opium, Codeine, Morphine… • The “Opiates” – Analgesic pain medications, centrally acting – Also block parasympathetic activity – Papaverine • Papaver alkaloid – Used for angina (vasodilatation) • Claviceps purpurea (Ergot – Rye or Wheat fungus) – Primarily vasoconstrictive agents (Ergonovine, DHE …) • Post partum / abortive hemorrhage – Also Bromocriptine (Dopamine agonist) and LSD family.

Amino Acids – General Information • In bowel dybiosis beta-AA’s are formed (via bacterial metabolism) Perpetuate poor GI flora, Increase B-6 need, Increase Taurine loss in the urine. • If patients experience HEADACHE or DIZZINESS with amino acid supplementation, they are deficient in co-factors, and or dehydrated. There should be no GI or Neurological side effects with amino acids.

Amino Acid Absorption • All absorbed by Na+ dependent cotransport • Di and Tripeptides are hydrolyzed to Amino Acids by peptidases • Cell to Blood transport via Facilitated Diffusion
")
Glutathione The Glutathione Redox Cycle and Peroxide H 2 O 2 2 GSH (Red) Glut. Peroxidase [Se] GSSG (Ox) 2 H 2 O NADP+ [B 2 -FAD] Glut. Reductase NADPH+H HMP Shunt

LIPID METABOLISM AND CARNITINE

PROTEINS: Amine Transfer

B 6 and Transaminase Reactions

Amino Acid Management • Consider and include all reasonable cofactor nutrients either prior to or with AA therapy • Many patients will find a reasonable AA dose that corrects their symptoms and can be maintained for 3 -9 months on the same dose. • Often they will be able to taper the AA dose SLOWLY over time as they replete with the AA. Some can do without the AA and some will require smaller maintenance dosing. • Most patients will need the cofactor nutrients the whole time, regardless of the AA taper. They may however require less of the cofactor nutrients over time.

Amino Acid Management • Therapeutic amino acid doses should be given away from other amino acids and protein foods if possible. – This allows for increased therapeutic efficacy and blood levels. – Daily doses over 1000 mg for amino acids typically need to be divided. • Amino acid transport in the GI tract and at the blood brain barrier is stimulated by Insulin, and in many instances by triiodothyronine (T 3) – Correction of hypothyroidism is crucial in all neuropsychiatric conditions – The addition of a small carbohydrate dose with the amino acid will help increase amino acid uptake.

VITAMINS-1 • WATER SOLUBLE – B-1, B-2, B-3, B-5, B-6, B-12 –C – FOLACIN – BIOTIN • FAT SOLUBLE –A –D –E –K

VITAMINS-2 VITAMIN FUNCTION DEFICIENCY A D E K Part of RHODOPSIN / VISION GI (Incr. Calcium absorption) Antioxidant CARBOXYLATION (of glutamate) / Calcium “chelation” with glutamate. NIGHT BLINDNESS Rickets / Osteomalacia Ataxia Factor 2/7/9/10 bleeding disorders B-1 B-2 B-3 B-5 B-6 B-12 ALDEHYDE transfer / DECARBOXYLATION H+ Transfer / FMN – FAD (Flavins) H+ Transfer / NAD – NADP ACYL Group Transfer / Co-A AMINO Group transfer / De-& Trans “aminations” BERI CHEILOSIS / GLOSSITIS VIT-C BIOTIN H+ Transfer / Hydroxylation of Lysine CARBOXYLATION FOLATE METHYL Transfer / Methionine Synth. Proline& PELLEGRA (Dementia/Diarrhea/Dermatitis) Burning Feet / HA / Nausea Microcytosis / Neuropathy Macrocytosis / Pernicious Anemia / Neuropathy SCURVY Seborrheic Dermatitis, Nervous disorders, Bound by Avidin (in egg white) Macrocytosis / Glossitis / Colitis
 Thiamin pyrophosphate - active – Beri-beri. Oxidative decarboxylation – Wheat")
VITAMINS-3 • B-1 (THIAMIN) Thiamin pyrophosphate - active – Beri-beri. Oxidative decarboxylation – Wheat germ, fish, meat, eggs, milk, cereals, green veggies. – Cardiac and neurological effects. • B-2 (RIBOFLAVIN) – FMN (flavinoidmononucleotide), FAD (flavinadeninedinucleotide) – Fish, meat, eggs, milk, greens. – Angular stomatitis, glossitis, seborrhea, anemia • B-3 (NIACIN / NIACINAMIDE) – – Pellagra. NAD / NADH formation. Part of the GTF. Used in Dehydrogenase reactions. Aka. Nicotinic acid / Nicotinamide. Wheat germ, fish, liver, peanuts.
 – Ubiquitous in foods. – Deficiency not common. Part")
VITAMINS-4 • B-5 (Pantothenic acid) – Ubiquitous in foods. – Deficiency not common. Part of Acetyl~S~Co. A. (Co. A) • B-6 (Pyridoxine) Pyridoxal-5 -Phosphate (active) – Magnesium is a cofactor. Used for amino acid metabolism. – Cereals, fish, meat, eggs, greens. – Anemia, dermatitis, neurological deficits (peripheral) • B-12 (Cyanocobolamin) – – – Meat, dairy, fermented foods. (Bacterial action) Intrinsic Factor facilitates absorption. Pernicious anemia. Macrocytic (megaloblastic) anemia. Activates the conversion of Homocystiene to Methionine Terminal Ileum absorption

Vitamin B-6 Notes: • Dosing acutely may require up to 2000 mg / day – This is for the pyridoxine form – P 5 P dose ½ to 1/3 this level • Dose until the patient remembers their last dream • Some patients tolerate better at night • Activates many neurological pathways • Neuropathy data: Most patients who developed peripheral neuropathies – Did not need supplementation – Were on 500 mg / day or MORE chronically

B-6 Vitamin B 6 in clinical neurology. Bernstein AL. Annals of the New York Academy of Sciences, 1990, 585: 250 -60. Vitamin B 6 supplementation may be useful in treating a number of conditions. For instance, headache, chronic pain, and depression, all associated with serotonin deficiency, have, in some studies, been shown to have been helped by B 6, which raises serotonin levels. In addition, B 6 may reverse the effects of toxic substances associated with hyperactivity and aggressive behavior.

CBS and B-6 In 1967, Barber and Spaeth reported that 3 cystathionine beta-synthase-deficient patients responded to high doses of pyridoxine (vitamin B 6), with decrease of plasma methionine levels to normal and virtual elimination of homocystine from plasma and urine.

Methylation Support • The two primary methyl transfer agents B 12 and Folic Acid are also intricately related to connective tissue health. • B-12 and Folate aid in transfer of Methyl groups which support amino acid metabolism, formation of nucleotides (cell repair), and multiple other supports to healing.
 is active in")
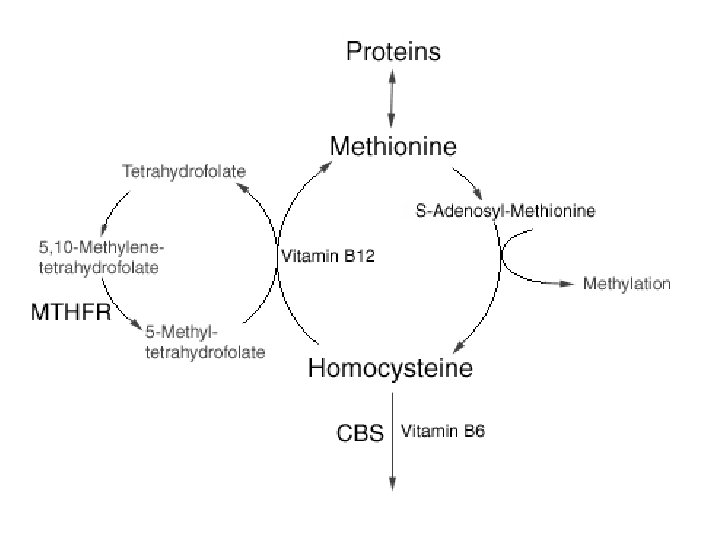
Methyl Transfer - B 12 & FOLATE THF (Tetra. Hydro. Folate) is active in methyl group transfer. The CH 3 transfer helps DNA in new cell production. MTHFR enzyme reduces the 5 -10 Methylene form to the 5 Methyl form, making B 12 activity possible B 12 frees FOLATE from its bound form (5 -Methyl-THF) to its coenzyme form (THF). It does this via a CH 3 release in the following reaction: CH 3 5 -10 -METHYLENE-THF MTHFR 5 -METHYL-THF METHIONINE HOMOCYSTIENE CH 3

MTHFR • The MTHFR gene provides instructions for making an enzyme called methylenetetrahydrofolate reductase. This enzyme plays a role in processing amino acids, the building blocks of proteins. • Methylenetetrahydrofolate reductase is important for a chemical reaction involving forms of the vitamin folate (also called folic acid or vitamin B 9). Specifically, this enzyme converts 5, 10 methylenetetrahydrofolate to 5 methyltetrahydrofolate. This reaction is required for the multistep process that converts the amino acid homocysteine to another amino acid, methionine. • http: //ghr. nlm. nih. gov/gene/MTHFR
![Methyl Cycle – Sulfur AA Interactions 5 -10 -Methyl-THF Folate [B-3] DHF [B-3—DHF reductase]](http://slidetodoc.com/presentation_image_h2/db01fba359d161188ca9a7f491da932f/image-60.jpg "Methyl Cycle – Sulfur AA Interactions 5 -10 -Methyl-THF Folate [B-3] DHF [B-3—DHF reductase]")
Methyl Cycle – Sulfur AA Interactions 5 -10 -Methyl-THF Folate [B-3] DHF [B-3—DHF reductase] Tetra. Hydro. Folate [B-3 ---MTHFR / B 2] Methionine / SAM-e CH 3 5 -MTHF [Betaine / B 12 ----Meth. Synth] Homocysteine [B 6 ------- CBS] Cystathionine (Toxic-S) [B 6] Sulfite Cysteine [Mg---GSH Synthase] [B 3] [Mo ------Sulfite Oxidase] [B 6] Sulfate (Helpful-S) Taurine Glutathione

MTHFR Diagnosis Concern: Symptoms / Elevated homocystiene / low uric acid / megaloblastosis… – “The common MTHFR alleles can be identified by direct sequencing. These alleles ‘create’ (C 677 T) or ‘abolish’ (A 1298 C) • It should be noted, however, that diagnosis of severe MTHFR deficiency on the basis of DNA analysis alone is not sufficient. This is because there is no single mutation linked to this severe form of the disease, and thus testing for known mutations may fail to recognize an unknown severe mutation. • Botto, L. D. & Q. Yang. 5, 10 -Methylenetetrahydrofolate Reductase Gene Variants and Congenital Anomalies: a Hu. GE Review. American Journal of Epidemiology 151, 862 -877 (2000).

MTHFR Sn / Sx • • • Developmental delay Motor abnormality Gait abnormality Mental retardation Seizures Psychiatric manifestations / Atypical dementia Moderate homocystinuria Homocystinemia (CVD…) Premature death Asymptomatic • http: //www. wrongdiagnosis. com/m/methylene_tetrahydrofolate_reductase_defici ency/symptoms. htm#symptom_list

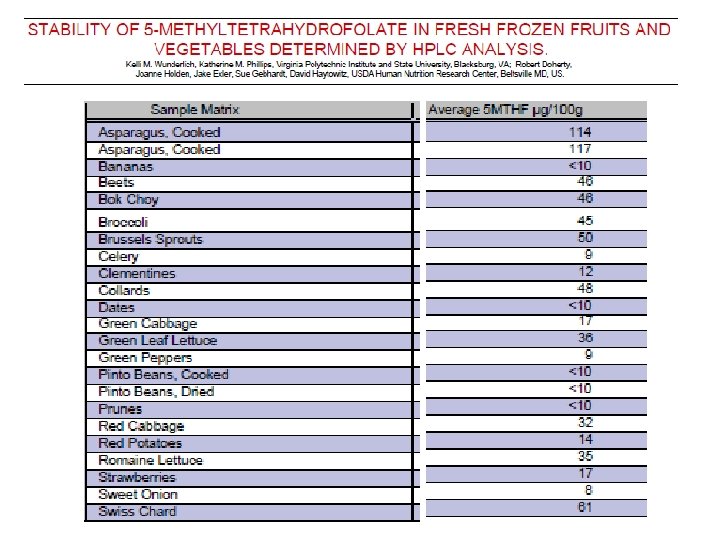
5 -MTHF in food and after Boiling • Spinach, Chinese cabbage, lettuce, cauliflower, and broccoli contained more than 50 μg of 5 -MTHF/l. OOg – less than 25 μg/100 g was found in potatoes, carrot, white cabbage, green and yellow pepper. • Individual vegetables differed in the folate retention during their boiling under constant conditions. – The highest retention was found in Brussels sprouts, cauliflower, and broccoli. After 8 min boiling more than 75% of the initial amount of 5 -MTHF remained in these vegetables. – Lower values of 5 -MTHF retention, between 37% and 52% of their initial content, were found in spinach, savoy cabbage, and carrot. • Holasova M, Fiedlerova V, Vavreinovav Slavomira. Determination of Folates in Vegetables and their Retention During Boiling. Czech journal of food sciences. 2008, vol. 26, no 1, pp. 31 -37 [7 page(s) (article)]ISSN 1212 -1800

MTHFR Therapy – Earlier Recommendations • MILD - MTHFR deficiency treatment diet control and folate. – This is due to previous studies indicating that folates will protect mild MTHFR mutant proteins from losing their FAD, thus restoring enzyme function to near normal levels [1]. • SEVERE - MTHFR deficiency is aimed at decreasing homocysteine levels and maximizing any residual enzyme activity. – The first line of treatment is the use of folate compounds, including folic or folinic acid [2] which work by maximizing residual enzyme activity via protecting the enzyme from losing. FAD cofactor [1]. – A second therapy included is 5 -MTHF which is used to compensate for MTHFR inability to produce 5 -MTHF. • Also used in treatment are two compounds aimed at compensating for the low methionine levels that result from MTHFR deficiency: – 1) Methionine – 2) Betaine (as substrate for betaine methyltransferase an enzyme that provides alternate route for conversion of homocysteine to methionine) [2]
![References – Prior Slide [1] Guenther, B. D. , C. A. Sheppard, P. Tran,](http://slidetodoc.com/presentation_image_h2/db01fba359d161188ca9a7f491da932f/image-66.jpg "References – Prior Slide [1] Guenther, B. D. , C. A. Sheppard, P. Tran,")
References – Prior Slide [1] Guenther, B. D. , C. A. Sheppard, P. Tran, R. Rozen, R. G. Matthews, and M. L. Ludwig. The structure and properties of methylenetetrahydrofolate reductase from Escherichia coli suggest how folate ameliorates human hyperhomcyseinmia. Nature Structural Biology 6, 359 -365 (1999). [2] Rosenblatt, D. S. Inherited disorders of folate transport and metabolism. In The Metabolic Basis of Inherited Disease (eds Scriver, C. R. , Beaudet, A. L. , Sly, W. S. , & Valle, D. ) 2049 -2063 (Mc. Graw. Hill, New York, 1989).

Another Opinion: • Cobalamin defective patients must be treated with parenteral supplementation of hydroxocobalamin (1 -2 mg per dose). • MTHFR patients could be folate responsive and must have a high-dosage folate trial. • Oral betaine supplementation (2 -9 g per day depending on age) appears an effective means to prevent further neurological deterioration. Ogier de Baulny H, Gérard M, Saudubray JM, Zittoun J. Remethylation defects: guidelines for clinical diagnosis and treatment. Eur J Pediatr. 1998 Apr; 157 Suppl 2: S 77 -83.
 X 10")
And Another: • 45 mg i. v. 5 -MTHF (Prefolic – Abbott) X 10 weeks plus 500 mcg s. q. Hydroxy-B-12 for the last 2 weeks. Trial done in Normal MTHFR and MTHFR variant patients. – On normal subjects plasma homocysteine fell 47% and fell ADDITIONALLY to 60. 6% after the addition of B-12 • Results were greater in MTHFR defective subjects – % Reduction Plasma Homocysteine • Homozygous MTHFR = 66% • Heterozygous MTHFR = 54% • Normal MTHFR = 29% • “Our study demonstrated that 5 MTHF administration not only reduced plasma homocysteine but also improved endothelial function…” Buccianti G, et. al. 5 -methyltetrahydrofolate restores endothelial function in uraemic patients on convective haemodyalisis. Nephrol Dial Transplant (2002) 17: 857 -864

Some Reasonable Recommendations for Tx: • Direct 5 -MTHF Support – 5 -MTHF, B-2 & B-3 • Collateral Pathway Support – Cystathionine Beta Synthase = B-6 (as P-5 -P) – Betaine Methyltransferase = Betaine / B-12 • Methyl Donor Support – Methyl B-12

Some Reasonable Recommendations for Tx: Dosing and Order of implementation • Methyl Donor Support – Methyl B-12 1 -5 mg SL / QD • Or 3 -5 mg IM weekly • Collateral Pathway Support – Pyridoxal-5 -phosphate 50 – 100 mg BID – Betaine HCl 3 – 9 grams divided doses with meals • Direct 5 -MTHF Support – 5 -MTHF ramp up 1 to 5 or 10 mg QD – B-2 & B-3 as obtained in a high potency bcomplex.

Forms of Folate: • Folic Acid requires DHFreductase FOL NADH/B 3 THF B 3+DHF-reductase • Folinic Acid / Leukovorin (formyl-THF) No DHFreductase required • 5 -Methyltetrahydrofolate (Graphics) http: //web 2. iadfw. net/uthman/nutritional_anemia. html
 – Fruit / Vegetables – Reducing agent (antioxidant). Large amounts")
VITAMINS-6 • C (ASCORBATE) – Fruit / Vegetables – Reducing agent (antioxidant). Large amounts convert to oxalate. Hydroxylation Reaction cofactor. (Bile, Proline, Dopamine) – Collagen integrity, immune function. • FOLATE – Converted to the active form (Tetrahydrofolate – THF) by B 12. Required for nucleotide synthesis. Methyl donor. – Cereals, liver, fruit, greens. – Macrocytic anemia, like B-12, without the neurologic deficits. • BIOTIN – – Many foods, produced by intestinal bacteria. Dermatitis. Carries CO 2 in carboxylase reactions Avidin (from raw eggs) will bind Biotin.
![Oxidation of Ascorbic Acid Ascorbyl Radical Ascorbate [ASC*] [ASC] Dehydroascorbic Acid [DHA]](http://slidetodoc.com/presentation_image_h2/db01fba359d161188ca9a7f491da932f/image-73.jpg "Oxidation of Ascorbic Acid Ascorbyl Radical Ascorbate [ASC*] [ASC] Dehydroascorbic Acid [DHA]")
Oxidation of Ascorbic Acid Ascorbyl Radical Ascorbate [ASC*] [ASC] Dehydroascorbic Acid [DHA]

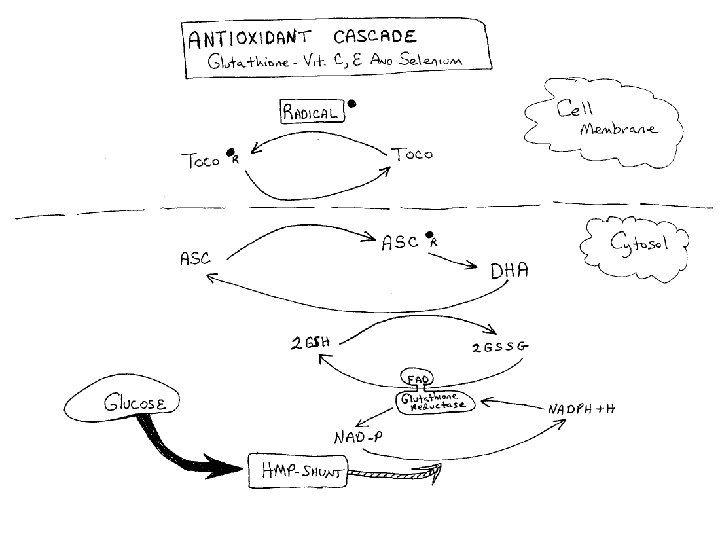
LDL Oxidation: The LDL has the potential to carry an incredible load of free radical. Anti-Oxidant effects of Vitamins E, C, GSH and the RBC - Lipid – Plasma Interaction RBC Plasma Reduced Glutathione LDL ASC Toco R Oxidized Glutathione DHA ASC R LDL + R = “oxidized LDL” Toco
![GLUTATHIONE • A TRIPEPTIDE (thiol glutathione [GSH]) • Poor oral absorption • Cofactor for](http://slidetodoc.com/presentation_image_h2/db01fba359d161188ca9a7f491da932f/image-75.jpg "GLUTATHIONE • A TRIPEPTIDE (thiol glutathione [GSH]) • Poor oral absorption • Cofactor for")
GLUTATHIONE • A TRIPEPTIDE (thiol glutathione [GSH]) • Poor oral absorption • Cofactor for antioxidant enzymes – Mitochondrial protection from endogenous oxygen radicals – High electron donating capacity, coupled with its high intercellular concentration give it extreme reducing power. • Two forms: – Reduced (the antioxidant) and Oxidized • Production: – Step 1: {[methionine cysteine] + glutamate}GGCS enz gamma-glutamylcysteine – Step 2 : {gamma-glutamylcysteine+glycine–GSH enz GSH – Glutathione is preserved by Ascorbate
")
Glutathione The Glutathione Redox Cycle and Peroxide H 2 O 2 2 GSH (Red) Glut. Peroxidase [Se] GSSG (Ox) 2 H 2 O NADP+ [B 2 -FAD] Glut. Reductase NADPH+H HMP Shunt

VITAMIN - K Vitamin K serves as an essential cofactor for a carboxylase that catalyzes carboxylation of glutamic acid residues on vitamin K-dependent proteins. Normally synthesized by bacteria in the gut. Newborns are deficient. The key vitamin K-dependent proteins include: 1. Coagulation proteins: factors II (prothrombin), VII, IX and X 2. Anticoagulation proteins: proteins C, S and Z 3. Others: bone proteins osteocalcin and matrix-Gla protein, and certain ribosomal proteins

Copyright IVNTP 78

VITAMIN - E

Vitamin E a-Tocopherol Vitamin E is a mixture of several related compounds known as tocopherols. The a-tocopherol molecule is the most potent of the tocopherols. Vitamin E is absorbed from the intestines packaged in chylomicrons. The liver can export vitamin E in VLDLs. Due to its lipophilic nature, vitamin E accumulates in cellular membranes, fat deposits and other circulating lipoproteins. The major site of vitamin E storage is in adipose tissue. The major function of vitamin E is to act as a natural antioxidant by scavenging free radicals and molecular oxygen. In particular vitamin E is important for preventing peroxidation of polyunsaturated membrane fatty acids. The vitamins E and C are interrelated in their antioxidant capabilities. Active a-tocopherol can be regenerated by interaction with vitamin C following scavenge of a peroxy free radical. Alternatively, a-tocopherol can scavenge two peroxy free radicals and then be conjugated to glucuronate for excretion in the bile.

VITAMIN - A
")
Vitamin A Use RBP (Retinol Binding Protein)

VITAMIN - D

VITAMIN D • This slide shows the bioconversion of a cholesterol residue by ultraviolet light in the skin circulation to Vitamin D-3 (cholecalciferol) • This pro-vitamin is then activated into 25 -OH-D 3 in the liver. (25 -OH-D 3 is the kind of Vitamin D most commonly tested medically as status of Vitamin D stores. ) • The kidneys then further convert it: – Under normal calcium blood levels to two active Vitamin D 3 forms which balance bone calcium metabolism – or– Under low blood calcium (with the help of parathyroid hormone) to 1 -25 -OH 2 -D 3 which helps bring low blood calcium back up to normal

MACROMINERALS

MACROMINERALS

MACROMINERALS • Magnesium Mg++

MACROMINERALS

MACROMINERALS

MICROMINERALS

MICROMINERALS

MICROMINERALS

MICROMINERALS

MICROMINERALS

OTHER NUTRIENTS - FLAVINOIDS • Phenols are universal in plant material • Flavinoids are polyphenolic compounds – Act as antioxidant to foods in storage – Protect Ascorbate and Tocopherol from oxidative decomposition during digestion – Have various levels of activity after absorption, based on the form taken in the plasma. • Some forms stabilize mast cells – (anti histaminic) – Hesperidin, Quercetin, Rutin…

OTHER NUTRIENTS – Co-Q-10 • Aka. Ubiquinone – Dose for Cardio Effect 75 mg + – Absorption is better with fat intake (either in the supplement or taken with dietary fats) • Powerful antioxidant – Helps in the preservation of Vitamin E – Found in Fish and other Meats (low quantity) • Body ability to synthesize drops after 30 • Formed in the Cholesterol / HMG pathway – Decreased by the “statin” class of drugs

OTHER NUTRIENTS – ALPHA-Lipoic-acid • Cofactor for mitochondrial energy reactions • Substrate production for Krebs cycle – Catalyses the metabolism of the branch chain AA’s • Leucine, Isoleucine, Valine – Supports glycine cleavage which supports 5 -10 -Methyl Tetrahydrofolate production • Used in nucleic acid synthesis • Antioxidant capabilities – Complexes with arsenic as an antioxidant – Regenerates other antioxidants (C, E, Q 10, GSH) – Repairs oxidative damage • Inhibits the enzyme elastase which degrades pulmonary elastin in COPD • Metal ion chelation ? ? (in vitro only? )

In order of number of prescriptions written in 2010, the 10 most-prescribed drugs in the U. S. are: • • • Hydrocodone (combined with acetaminophen) -- 131. 2 million prescriptions Generic Zocor (simvastatin), a cholesterol-lowering statin drug -- 94. 1 million prescriptions Lisinopril (brand names include Prinivil and Zestril), a blood pressure drug -- 87. 4 million prescriptions Generic Synthroid (levothyroxine sodium), synthetic thyroid hormone -- 70. 5 million prescriptions Generic Norvasc (amlodipine besylate), an angina/blood pressure drug -- 57. 2 million prescriptions Generic Prilosec (omeprazole), an antacid drug -- 53. 4 million prescriptions (does not include over-the-counter sales) Azithromycin (brand names include Z-Pak and Zithromax), an antibiotic -- 52. 6 million prescriptions Amoxicillin (various brand names), an antibiotic -- 52. 3 million prescriptions Generic Glucophage (metformin), a diabetes drug -- 48. 3 million prescriptions Hydrochlorothiazide (various brand names), a water pill used to lower blood pressure -- 47. 8 million prescriptions. IMS Institute for Healthcare Informatics: "The Use of Medicines in the United States: Review of 2010, " April 2011.
- Slides: 99