November 2018 Overview of homelessness and the homelessness

November 2018


Overview of homelessness and the homelessness service system

What is homelessness? ABS Statistical Definition of Homelessness A person who does not have suitable accommodation alternatives are considered homeless if their current living arrangement: • is in a dwelling that is inadequate; or • has no tenure, or if their initial tenure is short and not extendable; or • does not allow them to have control of, and access to space for social relations.
 For the purposes of this Act, a person")
Supported Accommodation Assistance Act 1994 (1) For the purposes of this Act, a person is homeless if, and only if, he or she has inadequate access to safe and secure housing. Inadequate access to safe and secure housing (2) For the purposes of this Act, a person is taken to have inadequate access to safe and secure housing if the only housing to which the person has access: (a) damages, or is likely to damage, the person’s health; or (b) threatens the person’s safety; or (c) marginalises the person through failing to provide access to: (i) adequate personal amenities; or (ii) the economic and social supports that a home normally affords; or (d) places the person in circumstances which threaten or adversely affect the adequacy, safety, security and affordability of that housing.

Extent of homelessness People who are homeless or at risk of homelessness: • 24, 828 people were homeless in Victoria on census night 2016: 42 in every 10, 000 people. • 41% of those people who identified as homeless on Census night in 2016 were in Melbourne’s north or west.

Why are so many people homelessness? We convey to clients that homelessness in Melbourne is not a symptom of individual failing and bad luck but is reflective of the housing crisis that we are experiencing. Melbourne has: • a housing supply problem (there are not enough houses for everyone – we need 1. 6 M more houses by 2050. Melbourne continues to grow by 1, 850 people a week); and • a housing affordability problem (for instance, no properties were considered affordable across Melbourne for someone on Newstart).

Question 1 Did you realise that so many people are experiencing homelessness? What does this mean for you?

Consumers of the homelessness service system

Consumers of the HSS Of those who present to the HSS in Victoria, • just over half are women • ¼ are under 25 • just over half are single people • 1/3 are accompanied by children • 6% are Aboriginal or Torres Strait Islanders The primary reasons people access homelessness services are: • Family violence (30%) • Eviction (18%)

Why do people present to the HSS? Key reasons cited for seeking homelessness assistance Time out from family/other situation Medical issues Mental health issues Lack of family and/or community support Previous accommodation ended Relationship/family breakdown Housing affordability stress Inadequate or inappropriate dwelling conditions Domestic and family violence Financial difficulties Housing crisis 0 2, 000 4, 000 Total clients (number) 6, 000 Females 8, 000 Males 10, 000 12, 000 14, 000 16, 000
 in Melbourne’s north and west supported: Numbers of")
In 2015/16 specialist homelessness services (SHSs) in Melbourne’s north and west supported: Numbers of households assisted: Presenting unit head by gender, North and West Homelessness Services, 2015/16 8, 000 7, 000 27, 753 households (36, 053 people), through 41, 866 support periods. • 5, 282 children accompanied their parent/s. • To March 2018 we had already supported 22, 266 this year. 6, 000 5, 000 4, 000 3, 000 2, 000 1, 000 0 0– 9 10– 14 15– 17 18– 24 25– 34 35– 44 Males Females All clients 45– 54 55– 64 65+

What is the HSS?
 across Australia are jointly funded")
Funding for the HSS • Specialist Homelessness Services (SHSs) across Australia are jointly funded through by the Commonwealth and State Governments, through the National Housing & Homelessness Agreement To provide assistance to people who are homeless or at (http: //www. federalfinancialrelations. gov. au/content/hous risk of homelessness to support them: ing_homelessness_agreement. aspx) • to find or maintain stable long term housing; and • The Commonwealth sets targets for the State but the State • to address those issues that have contributed to manages allocation of the funding. homelessness or homelessness risk to reduce the likelihood of recurring homelessness. • Funding is allocated to community organisations through a Funding and Service Agreement (FASA) by the Department of Health and Human Services. • The FASA outlines targets for each homelessness program and all guidelines, legislation and conditions of funding that the service must adhere to.

What is the role of the HSS? Broad aim: To provide assistance to people who are homeless or at risk of homelessness to support them to: ▪ find or maintain stable long term housing; and To provide assistance to people who are homeless or at ▪ address those issues that have contributed to homelessness or homelessness risk of homelessness to support them: risk to reduce the likelihood of recurring homelessness. • to find or maintain stable long term housing; and • to address those issues that have contributed to The SAA Act: the overall aim of homelessness support services is: homelessness or homelessness risk to reduce the To provide transitional supported accommodation and related support services, in likelihood of recurring homelessness. order to help people who are homeless to achieve the maximum possible degree of self-reliance and independence. Within this aim the goals are: (a)To resolve crisis; and (b)To re-establish family links where appropriate; and (c)To re-establish capacity to live independently of homelessness support.

What is the NWMR HSS? • 5 generalist, 2 family violence and 1 youth specific access point services • 5 transitional housing management services, managing 1, 100 properties • 50 homelessness support agencies providing 180 programs, targeted to: young people, single men, single women, families or cross target, including Aboriginal and Family Violence specific services • Brokerage such as: Housing Establishment Funds, Private Rental Brokerage Programs, Flexible Support Packages, CEEP • Capacity building programs such as FRMP, Living Skills, Children’s Resource Coordinators • Tenancy Plus– support for public and community housing tenants at risk of eviction

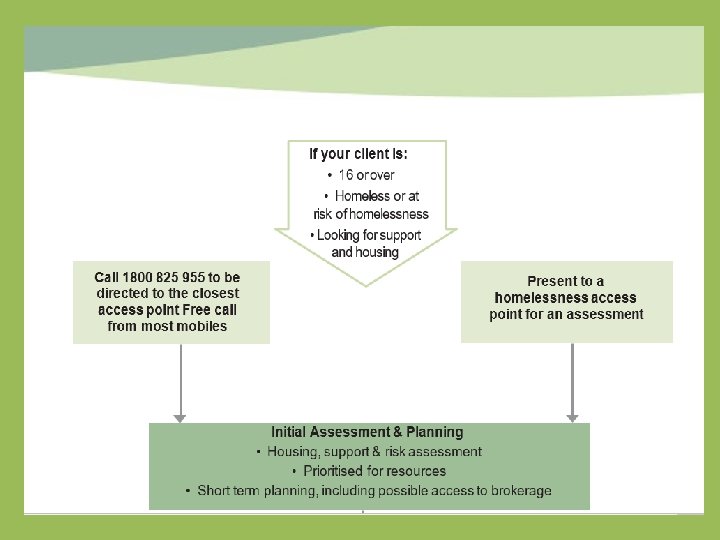
Access Point Services • Provide the first point of contact with the homelessness service system Role: • Initial assessment. • Risk assessment • Identification of immediate needs • Short term planning occurs with clients to manage future needs. • Best matching and referral to homelessness resources
: youth refuges, women’s")
Homelessness support services linked to accommodation ▪ Crisis supported accommodation (CSAs): youth refuges, women’s refuges and supported accommodation for single men, single women and families Case managed support in crisis support and crisis supported accommodation services is funded for an average of six weeks with a high ratio of staff to clients (generally 1 worker: 6 individual clients or 5. 5 households when assisting families). ▪ AO 4 F, SFAR ▪ Foyer models: Step Ahead, Ladder, Hope Street Melton and Whittlesea, Launch Broadmeadows and soon Wyndham

Brief Task Based Response Interim Response 1 • Telephone ‘check in’ with those most vulnerable • Update consent every six months • Primarily by access points Brief Task Based Response (IR 2) Short term targeted assistance to individual/households who have been assessed and are awaiting housing and/or support: • Prevention/early intervention – short term assistance to help a client maintain current housing and avoid the need to enter the HSS • Short term support/crisis intervention to provide assistance to clients to avoid an escalation of their crisis whilst awaiting access to support/housing.

Transitional support Case managed support to assist people in crisis to move to independent long term housing. • The average duration of support is 13 weeks. • Generally provided on an outreach basis: clients may be residing in temporary situations (e. g. a rooming house), exiting crisis accommodation (e. g. refuge), or in transitional housing. Support may be offered from an office base, the client’s residence or an agreed venue • 1 worker: 12 clients when supporting individuals • 1 worker: 7. 5 households when assisting families (about 2. 5/hrs a week per client) • Support provision includes: assistance to find housing, emotional support, advocacy, assistance to obtain income, parenting support, active referral to other service systems, assistance with living skills, assistance to access employment, education and training.
 • 1, 100 transitional")
Transitional Housing • Medium term accommodation (20 weeks on average) • 1, 100 transitional housing properties across the North and West. (200 are attached to ‘joined up’ initiatives) • Subject to the provisions of the Residential Tenancies Act (RTA) • Responsibilities guided by the Housing and Support Partnership Agreement. • Properties allocated proportionately to need by IA&P from the prioritisation list. • Access point data: approximately 1 in 85 clients will access transitional housing

Direct referral services You can contact these services directly: • Flat Out/ACSO/Brosnan ▪ Aboriginal homelessness services ▪ Family Violence Services ▪ Youth programs o o o Reconnect Creating Connections Private Rental Brokerage Creating Connections Intensive Case Management Creating Connections Living Skills Program Family Reconciliation Mediation Program Youth foyers • Day centres • Bright Futures and Children's Resource Program

Family Violence Services in the North and West Homelessness funded family violence programs: • Women’s Health West and Berry Street • Family Violence Outreach Support/ L 17 s • Court Support • CALD specific support • Flexible funding packages • Five women’s refuges Georgina Martina, Mary Anderson, Elizabeth Morgan, Women’s Health West and Mc. Auley Community Services for Women • Statewide: Safe Steps and In Touch Broader Integrated Family Violence Services • Men’s behavioural change programs • Women’s and children’s counselling programs

Question 2 Do you feel that you are apart of a coordinated service system? How does coordination play out for you in your role?

Framework for the homelessness service system

Why Opening Doors? • Prior to 2008, there were 400 entry points in Victoria. • People who were homeless reported that they found it hard to navigate the service system • Services were responsive to their own consumers, but without a common framework there was no sense of shared responsibility • Resources were so limited, in relation to need, that the need to manage the resources as effectively as possible was pressing. • A clear need existed to improve consistency and coordination across the State

Practice Framework: Opening Doors Practice and systems approach to provision of timely and effective access to homelessness and social housing services: • A consumer focussed and strengths based approach • Equity of access to the resources of the HSS • Reasonable care to address the risks faced by each person who is homeless • Maximising the use of available homelessness resources • Visible entry points staffed by initial assessment teams • The system ‘holds’ the client • Consistent, high quality practice that reduces multiple assessments and unsuccessful referrals • Collaboration and partnership between agencies and DHHS
 with")
Role of the LASN Homelessness services formed into local area service networks (LASNs) with shared responsibility for: • Holding consumers and assisting them to navigate the service system • Coordinated provision of services • Operating a shared prioritisation approach matching client need to available resources • Managing the limited resources of the Sector effectively • Sharing information and provide advice to DHHS & advocacy

Shared approaches Opening Doors developed common approaches and shared tools: • A shared assessment framework • A shared approach to prioritisation • Development of a resource register • Statewide and local practice guidelines The LASNs monitor these coordinated HSS arrangements, through: • Regular LASN meetings • Improvement log • Practice Advisory Group • Consumer feedback • Working Groups

Structure of the Networks Making Links Project (AOD, mental health, homelessness Allied services Information sharing and projects with allied sectors ) Western and Northern Integrated Family Violence Committees Network 300+ individuals from homelessness and allied agencies - sharing information Local Area Service Network 50 members managing 180 programs Decision making mechanism for the Network Advocacy, sector coordination and development Consumer Participation Working Group Youth Network Practice Advisory Group Steering and Reference Group approx. 10 members Monitors progress of strategic plan and Networker role BTBR Working Group Access Point/THM Working Group Homelessness Week Working Group

Navigating the HSS

Role of Consumers • All programs are voluntary • Consumers choose geographic area and programs • Consumer charter guides client rights and responsibilities • Consumers consent to transfer of information across the HSS • LASN collects and responds to consumer feedback

Access • Consumers present to any access point for assessment, short term planning and prioritisation for referral. • ADDRESS ON HEALTH CARE CARD DOES NOT DETERMINE SERVICE. • 1800 # - diverts to the nearest access point during the day – in theory • Access Points negotiated a shared approach to HEF allocation.

Assessment • Assessment is narrative based • Recorded in a standard format across the State • Two part assessment: a) Initial assessment - Access Points • Incorporates risk assessment • Assessment of support need, housing need and personal vulnerability • Informs short term planning b) Comprehensive assessment - Support Agencies • Comprehensive assessment to inform case plan

Short term planning • Ascertain need for emergency accommodation • HEF, referral to hotels and rooming houses • Co-contribution system • Identify short term goals and develop a plan in response • Undertake a risk assessment • Place on prioritisation list for referral to support and accommodation • Make referrals if possible
 is a consumer data")
Client consent and data • Specialist homelessness information system (SHIP) is a consumer data system • SHIP informed consent approach utilised • Consent obtained at the access point • Consent lasts six months • Consent applies to transfer of information across the homelessness service system

Diversion and short term responses Brief Task Based Response • Brokerage to assist • Funds to assist people to • people to access or establish/re-establish in maintain the private rental accommodation. market • Usually used to purchase • Advice to assist people emergency to access private rental • accommodation. • Family Violence Flexible Funds Very short term assistance to either divert people from homelessness or contain crisis Task based, 1 -6 contacts

Prioritisation for resources • Standard approach to prioritisation of resource allocation across State • Housing and support need and level of vulnerability determined as high, medium or low • All clients assessed included in prioritisation list for access to support and/or housing • Priority of need can be changed to better reflect client circumstance. • Clients being supported outside the HSS can still be prioritised for access to transitional housing if they have a current assessment at an Access Point • Other access points can forward assessments

Housing need

Support need

Level of vulnerability

Resource Allocation • All resources listed on Resource Register • Holder of resource responsible for ‘publishing’ and describing resource • Access Points ‘best match’ to available resources • Access Points refers to resource (support first then housing if available • Agency accepts first eligible referral • Agency contacts client and arranges access to resource • Agency advised access point whether consumer needs to remain on prioritisation list

Resource Register

Housing and Support Partnership Agreement • Tenancy and support work together to support tenant. • Clarifying shared responsibility of tenancy and support workers and tenant • Support available for duration of tenancy • Communication • 3 way meetings – client, tenancy & support • Clear information for tenants • Shared understanding and consistency of practice

Managing scarce resources o In 2015 there were 4, 176 (6, 171 people – including Transitional housing vacancies 50 2, 575 children). o In 11/12 300 new households presented to access points Case managed support vacancies 100 services each month. In 2018 300 new household present to one access point each Presenting to HSS for first time per month 300 month. o In 2018 there are 10 vacancies for support and 10 for Numbers on the PL 4000 transitional housing in the one catchment per month. 0 2000 4000 6000

Question 3 • Do you have any questions or comments about the HSS?

Guidelines Statewide: • • Guidelines and Conditions of Funding Prison Exits Protocol Cross Regional Referral Protocol Youth Justice/Homelessness Protocol In the North and West • Regional Practice Manual • Housing and Support Partnership Agreement • Family Violence Entry Point/ Homelessness Access Point Protocol • IR 2 Practice Guide • Improvement Log • Post Referral Feedback form • Intra regional HEF Guideline

For further information… Sarah Langmore Western Homelessness Network Coordinator Ph: 0407 832 169 sarah@wombat. org. au Meredith Gorman Northern Homelessness Network Coordinator Ph: 0424 112 445 meredith. gorman@launchhousing. org. au North West Homelessness Networks website: www. nwhn. net. au/subscribe (Subscribe to e bulletin): www. nwhn. net. au/subscribe

Where do the Children Fit?

CHILDREN’S RESOURCE PROGRAM The core functions of the program include: • Direct support to homelessness, family violence and allied health services and workers • Service system development • Secondary consultations • Resource distribution • Training provision & coordination • Raising awareness about the impact of homelessness and family violence on children • Community education • Networking • Brokerage • Cross sector linkages

DEFINITION Accompanying Children: “a person who is under 18 years of age; receives support, accommodation or assistance from a Specialist Homelessness Service agency; and has a parent or guardian who is a client of a Specialist Homelessness Service agency. ”

CHILDREN IN SHS Children represent 27% of people accessing the homelessness service system across Australia (Homelessness Australia(HA) 2016) Children aged 0 -12 years are one of the largest groups of service users – 17, 845 (HA 2016) Over 60% of children who were accommodated by SHS have witnessed or been victims of family violence (HA 2016) The experience of homelessness is not a one off event that children bounce back from, it can become a defining event that shapes their lives.

FLOWERS IN OUR GARDEN https: //vimeo. com/23303866

In a service system that fails to: • fund accompanying children as clients • recognise that accompanied children are the largest client group • recognise the complex and specific needs of children As workers how can we: • relate to children in their own right? • develop a curiosity about the experiences of the child rather than the experiences of the adult? • identify our strengths and attitudes that facilitate effective responses to children and their parents?

A CHILD’S EXPERIENCE Homelessness and family violence can impact on: Physical Health – chronic illness, poor dental health, access to health services Cognitive growth – interrupted neural pathway development Mental Health – low self esteem, behavioural issues, grief and loss Emotional Health – self esteem and confidence, difficulty making friends, depression, interrupted attachments Education – school refusal, interrupted schooling, bullying, learning delays Transience – disconnected from supports and community, lack of security Culture – high risk of cultural disconnection

CHILDREN NEED …… • To feel safe and secure and to be able to see a future/ hope for a future • Children need to feel important and visible. • To be able to tell their story and to feel heard • Adults around they can trust and can talk with. • To have appropriate and consistent responses to their experience, i. e. children experience trauma, loss, grief and isolation. • To be included or involved in the plans about their life. • Experiences and opportunities afforded to their peers i. e. recreational opportunities. • Timely and relevant/ specialised response to their needs i. e. counseling, assessments – Mental health, general/specialist health, Child Protection

ROLE OF SHS WORKER What does all this mean for you? • Need to understand the principles of Best Interest of the Child and Cumulative Harm (these are guiding principles that inform your work) • Have a fundamental knowledge of an assessment framework for children (you know what to look for and what to ask about) • Have a case management process (or practice approach) that is child -focussed and age appropriate (you know where and how to link in helpful resources) • Appropriate organisational documentation that supports the above (you are supported & guided by your organisation e. g. children’s policy, budget allocation, resource guide etc. )

ROLE OF SHS WORKER • You can make a positive influence in a child’s life. • Help parents identify their children’s strengths, likes and dislikes. • Be aware of children’s heightened sense of protectiveness, guilt and responsibility • Share information with the primary caregiver regarding effects of homelessness and family violence on children. • To understand the importance of play in a child’s normal development. • Make time to sight and speak with children – including babies. • Responses need to be specific to each child and their unique experience. • Need to look at crisis needs vs. short to long term needs where appropriate. • Attend child specific training.

RESOURCES North West Regional Children's Resource Program www. homelesskidscount. org State School Relief: http: //www. ssr. net. au Raising Children Network www. raisingchildren. net. au Children of Parents with a Mental Illness http: //www. copmi. net. au/ Association for Children with a Disability www. acd. org. au VACCA www. vacca. org VICSEG http: //www. vicsegnewfutures. org. au/ Australian Childhood Foundation www. childhood. org. au
- Slides: 61