Nottinghamshire COPD and Asthma Guidelines Dr Esther Gladman














")














- Slides: 33
Nottinghamshire COPD and Asthma Guidelines Dr Esther Gladman GP Prescribing Lead, Medicines Management Nottingham City CCG Feb 2012
Where to find & other resources • Google: Nottinghamshire Area Prescribing Committee – Medicines Traffic Light Classification List – Shared Care Protocols – Clinical Guidelines – Formularies – Policies and Prescribing Position Statements • E-healthscope • www. patient. co. uk • www. prodigy. nhs. uk (was CKS)
e. g. from prodigy : What simple measures can I advise to manage breathlessness for people with end-stage COPD? • Advise the person on the following simple measures to manage breathlessness. – Sitting in front of a fan or open window (or using a hand-held fan). – Positioning • For example, advise the person to sit or stand leaning forward (for example onto a table or the back of a chair) and supporting their weight with their arms and upper body. – Pursed-lip breathing • Advise the person to inhale through the nose and then exhale slowly, for 4– 6 seconds, through pursed lips. • Other simple measures, not specific to chronic obstructive pulmonary disease (COPD) but recommended in the section on Simple measures to help dyspnoea in the PRODIGY topic on Palliative cancer care - dyspnoea, may be useful for people with COPD.
• • • Nottinghamshire COPD Guideline Key points Most effective interventions Be aware other conditions Effective/cost effective prescribing Steroid dose, pneumonia & adverse Be aware side effects and adverse effects of meds Where can you make a difference?
Most Effective Interventions • 1. Stopping smoking is the only treatment that slows the progression of COPD and is the most cost effective treatment in COPD. NNT 5 –to prevent death at age 70 • Motivational questioning, cost cigs & inhalers, Allen Carr, anxiety, dopamine, worsening of symptoms, dementia
Most Effective Interventions: 2. Pulmonary Rehabilitation • MRC dyspnoea score 3, 4, 5 • or recent admission “more breathless than contemporaries when walking or gets breathless on exertion & needs to rest” – NNT 2 to improve exercise tolerance by a clinically useful amount – NNT 4 to stop readmission over 6/12 if given early after an exacerbation
Most Effective Interventions 3. Self Management Plans • NNT 10 to reduce admission in low risk patients • NNT 3 to reduce admission in high risk patients (1 previous admission or LTOT or previous use of Prednisolone) • NNT 5 for patient held “emergency supply pack” (prednisolone +/- antibiotic) to reduce admission
Beware diagnosis • >40 years old • Smoker or ex-smoker, non-smoking spouse of smoker or dusty occupation • Spirometry FEV 1 < 80% predicted and post bronchodilator FEV 1/FVC ratio < 70% and typical symptoms • NB FEV 1 – an increase of >400 ml after bronchodilator suggests asthma not COPD • Consider CXR/FBC, ECG for alternative diagnoses or red flag symptoms such as haemoptysis
Be aware: are symptoms in accord with severity of COPD? – FEV 1 Rapid decline? e. g. >200 ml in 3 years, exacerbations/Excess sputum – Re-assess for co-morbidity, treatment adherence, inhaler technique • Consider bronchiectasis • check sputum for unusual organisms/Acid & Alcohol Fast bacilli • ? Ca CXR, FBC, ECG • NB 25 % will have IHD/ cardiac failure
Effective/cost effective prescribing • Stop smoking • Optimise inhaler technique (e. g. spacers with MDIs) • Consider stopping new treatment if patient feels no improvement (4 weeks) – longer may be needed for a reduction in exacerbations • Consider stepping down/swopping
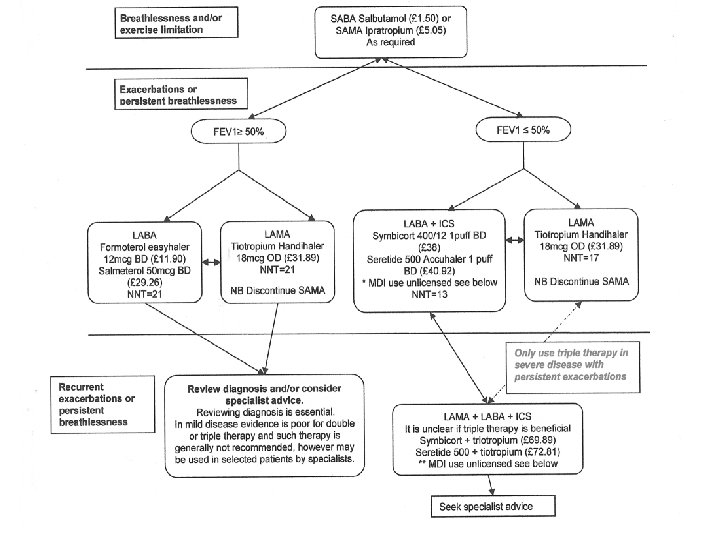
Effective/cost effective prescribing • LABA vs LAMA – there is no significant difference re: reduction in exacerbation or hospitalisation rates.
Effective/cost effective prescribing • There is no combination MDI licensed for COPD • However if patient preference: – Fostair 100/6 (2 puffs BD £ 29. 32) – or Seretide 125 + spacer (2 puffs BD, £ 35) can be considered, which gives similar ICS dose to Accuhaler 500. • NB Seretide 250 MDI is not recommended
Adverse effects of steroid • High dose ICS (ie fluticasone 1000 mcg = Seretide 250) increases the risk of pneumonia, NNH = 47 ie. Beware those with frequent exacerbations • Other steroid effects - Diab/thrush/cataracts • Osteoporosis prophylaxis for patients having 4 courses of oral steroid within 12 months
Be aware side effects and adverse effects of meds • Use tiotropium Spiriva Handihaler® (18 mcg/day) not Spiriva Respimat® (mist device) All patients must be advised not to exceed the maximum daily dose • All anticholinergics have some cardiovascular effect • Fometerol and beta agonists also have effect
NBs • Mucolytic only if troublesome phlegm: carbocisteine 750 mg TDS (£ 24. 60) can be trialled for 4 weeks. – – Stop if no effect. Drop to maintenance dose: 750 mg BD if effective. Consider using in winter months only. Mucolytics do not prevent exacerbations • Consider theophylline 3 rd line: Uniphyllin 200 mg BD (£ 2. 94) care with elderly & concomitant medications see BNF. Theophylline levels? NNT=33
NBs • 25% will have co-morbidity e. g. IHD/cardiac failure. Beta blockers can be used in COPD • Dose of emergency supply pack?
Actions Flu & pneumococcal vaccination Inhaler use/Medication /step Stop smoking advice /refer New Leaf Patient info/empowerment MRC dyspnoea score 3, 4 or 5/functional disability refer for pulmonary rehabilitation • Self management plan and anticipatory prescription pack • Weight/diet/exercise. Little & often leaflets • • •
• Oxygen Sat ≤ 92% - refer to chest clinic /oxygen assessment service • Palliative Care Planning If end-stage COPD/cor pulmonale
Nottinghamshire Adult Asthma Treatment Summary • Micro break & shake
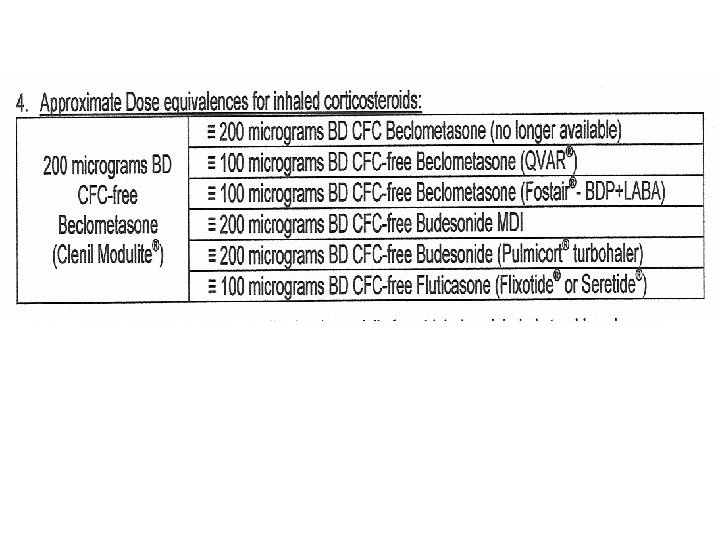
Nottinghamshire Asthma Guideline Key points • • Step up and down Use LABA and ICS in a combination inhaler Be aware of inhaler equivalent steroid doses Step 3 a is addition of LABA not increase ICS too Twitchiness of asthma Same steroid risks as for COPD Pros & cons of SMART Theophylline levels/interactions
Step Consider stepping up if: 1. Using SABA 3 times a week or more 2. Symptoms 3 or > times x week 3. An exacerbation in the last 2 years 4. Waking due to symptoms one night a week • Ensure adherence and inhaler technique Consider stepping down if : Asthma control has been good for 3 months on current therapy N. B. Steroid dose reductions should be slow as patients deteriorate at different rates. Reduce by 25 -50% & monitor
Appropriate spacer/ Other devices? Peak flow meter?
Step 3 a nb add LABA only
Step 3 b & c
Step 3 alternative
SMART Pros: opener & reliever, inc dose steroid when need it Cons: device, symptoms, side effects
Step 4 asthma nb this is where use of Seretide 250 MDI is appropriate
nb • Oral steroid - sometimes higher dose & shorter course than COPD • Same steroid risks as for COPD • Written Self-Management Plan/lifestyle/house dust mite/patient beliefs/info • Co-morbidity
Key points summary • Step up and down • Always give LABA and ICS in combination inhaler (unlike COPD) • Step 3 a is addition of LABA not increase ICS too • Be aware potency of ICS Inhaler and equivalent steroid doses