Normal Menstruation Dr SHUBHANGI MANDE Definition Menstruation is

Normal Menstruation Dr. SHUBHANGI MANDE

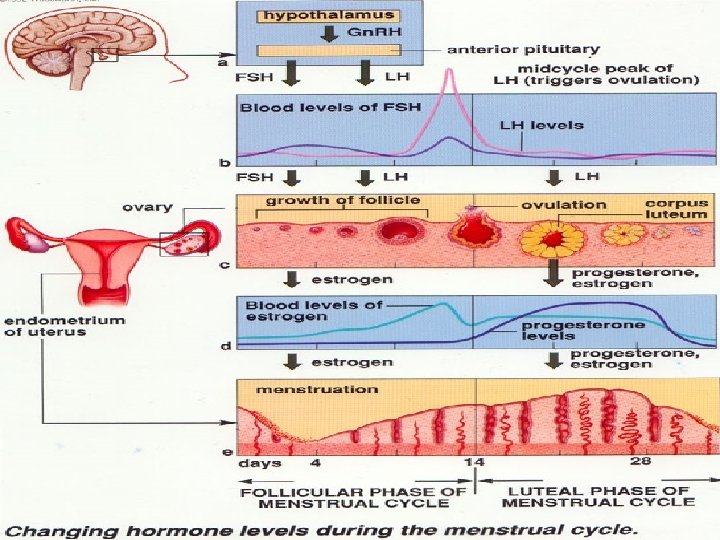
Definition – Menstruation is the visible manifestation of cyclical physiologic uterine bleeding due to shedding of the endometrium. � Menarche occurs between 11 -15 years with a mean at 13 years. � Once, the menstruation starts it continues clinically at intervals of 21 -35 days with a mean of 28 days. � Duration is about 4 -5 days with a blood loss of 20 -80 ml with a average of 50 ml. � Menopause occurs between 45 -50 yrs; mean at 47 yrs
 Follicular Phase 2) Ovulation 3) Luteal Phase Endometrial 1)Regenerative phase 2)Proliferative")
Phases Ovarian 1) Follicular Phase 2) Ovulation 3) Luteal Phase Endometrial 1)Regenerative phase 2)Proliferative phase 3)Secretory phase 4)Menstrual phase

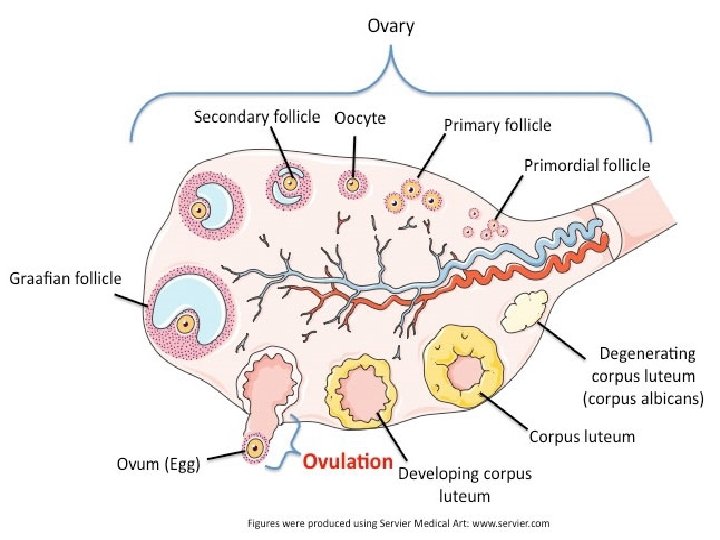
Follicular Phase =>Primordial Follicle. Primordial follicle consist of an oocyte which is surrounded by a single layer of flattened granulosa cells. Follicle measures about 0. 03 – 0. 05 mm. Total number of oocyte at 20 wks of intrauterine – 6 to 7 million. At birth - 2 million; remaining. At puberty - 40, 000; left behind. Out of these some 400 are likely to ovulate during the entire reproductive period.

� Apoptosis is a greek word meaning shedding of a leaf from a tree. � Recruitment has been traditionally used to describe the continuing growth of antral follicles in response to FSH. � The cohort of follicles responding to FSH at the beginning of a cycle is rescued from apoptosis. � At this time small gap junction develop between the granulosa cell and the oocyte this acts as the pathway for nutritional , metabolite and signal interchange between the granulosa cells and the oocyte.

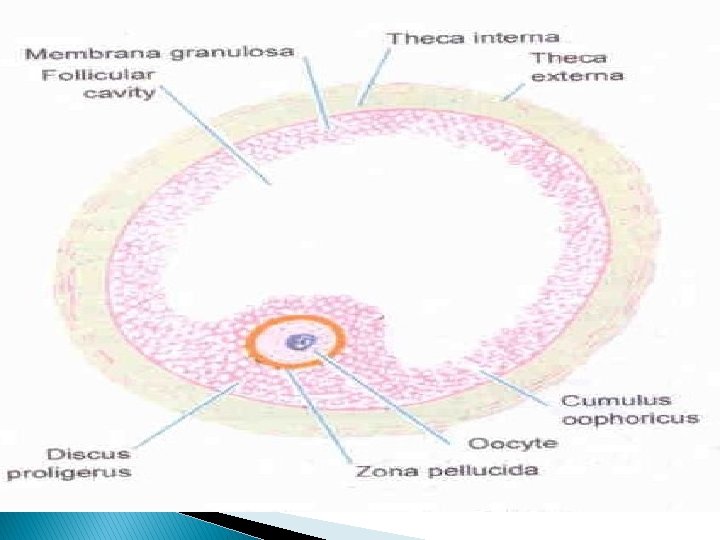
� Activin and AMH promotes primordial follicle � Inhibin and Bone morphogenic protein retards primordial follicle. � With multiplication of the cuboidal granulosa cells , the primordial follicle become a primary follicle. � The granulosa layer is seperated from the stromal cells by a basement membrane called the basal lamina. � It forms Theca interna and externa.
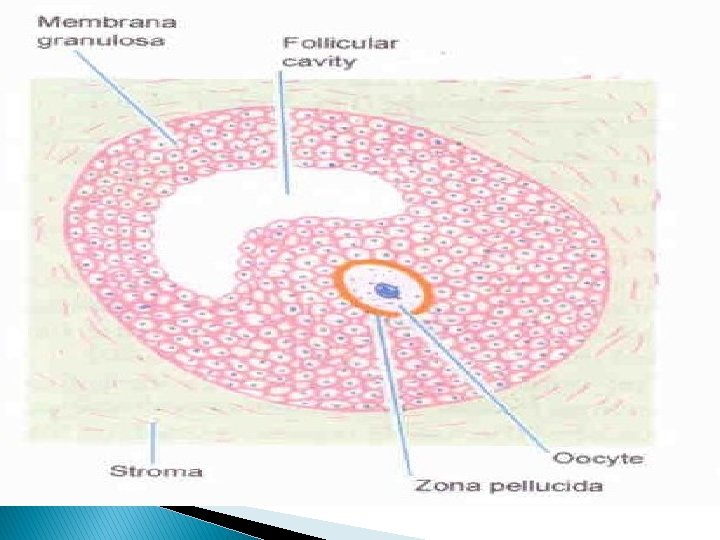

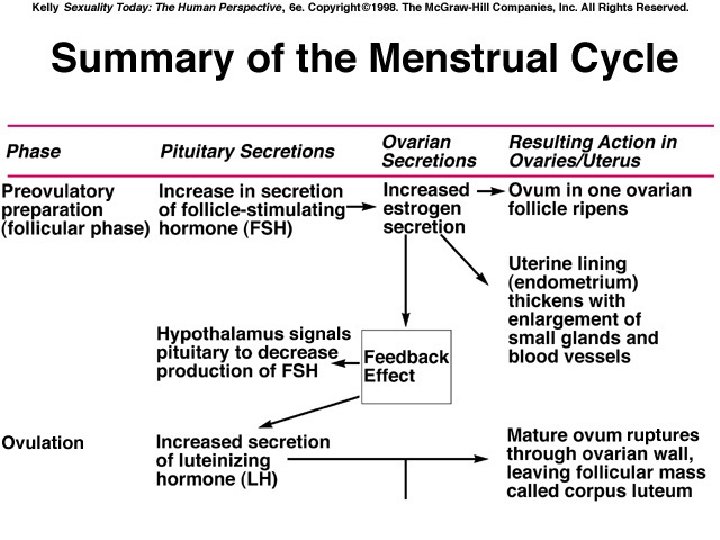
Preantral Follicle � Primordial follicle progresses to preantral stage as the oocyte enlarges with surrounding membrane, the zona pellucida dependent upon gonadotropins and estrogen. � Aromatase enzyme system converts androgen to estrogen and is a factor limiting the ovarian estrogen production. � Specific receptor for FSH are formed at preantral stage. � Preantral follicle requires presence of FSH in order to aromatize androgens and generate its own estrogenic microenvironment. � FSH combine synergistically with estrogen to exert a mitogenic action on granulosa cells to stimulate their proliferation.

Antral Follicle � Under the synergistic influence of estrogen and FSH, there is increase in the production of follicular fluid. The granulosa cell surrounding the oocyte are now designated as ‘cumulus oophorus’. Selection of dominant follicle depends on� 1)a local interaction between estrogen and FSH within the follicle � 2)effect of estrogen on pituitary secretion of FSH

� The negative feedback effect of estrogen on FSH serves to inhibit the development at all stages except the dominant follicle. � The dominant follicle has two significant advantages 1) a greater content of FSH receptors acquired because of a rate of granulosa proliferation that surpasses its cohort 2) enhancement of FSH action because of its high intra folllicular estrogen concentration, a consequence of local autocrine and paracrine molecules

� The accumulation of a greater mass of granulosa cells is accompanied by advanced development of theca vasculature. � By day 9, theca vasularity is twice in the dominant follicle as that of other antral follicles. � In order to respond to the ovulatory surge and to become a successful corpus luteum, the granulosa cell must acquire LH receptors. � FSH induces LH receptors development on the granulosa cells of the large antral follicle.

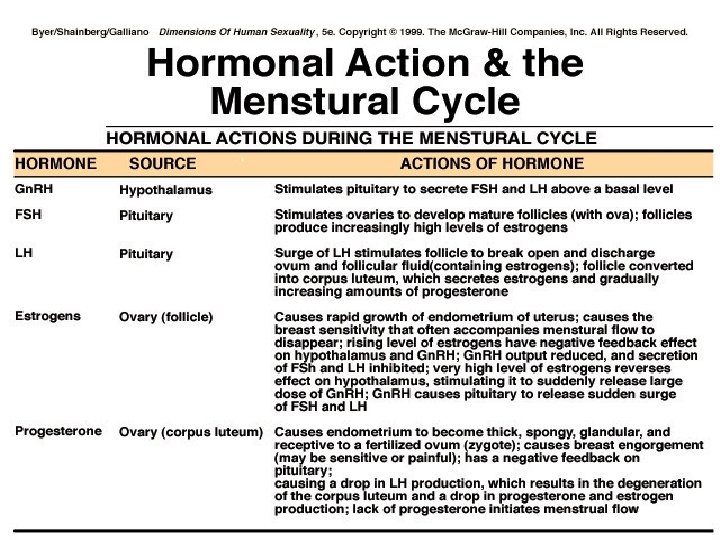
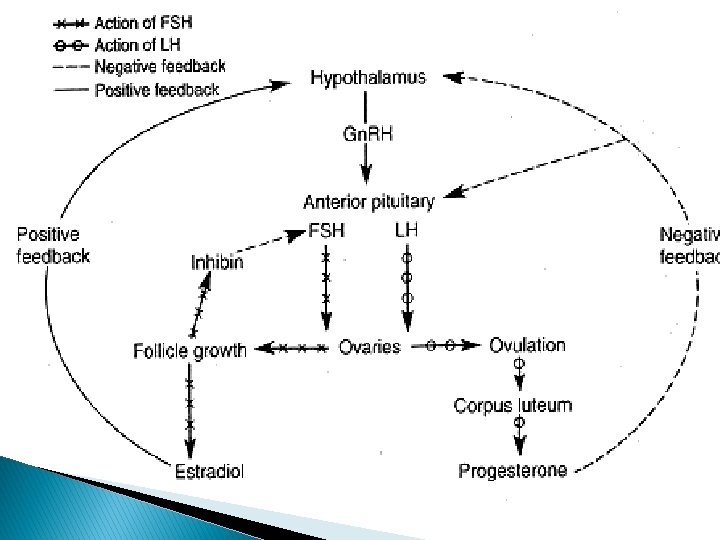
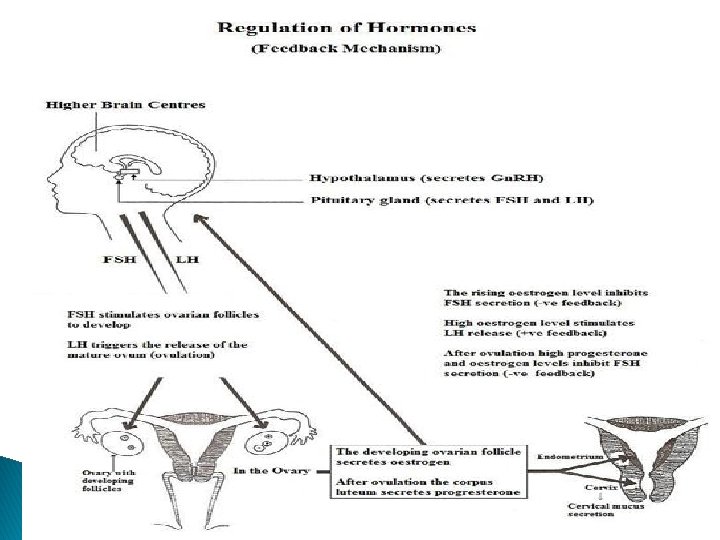
� LH plays a critical role in the late stages of follicle development, providing support for final maturation and function of the dominant follicle. � Estrogen exerts inhibitory effect in both the hypothalamus and anterior pituitary decreasing both Gn. RH pulsatile secretion and Gn. RH pituitary response. � Progesterone has its inhibitory action at the hypothalamic level and positive action is directly on the pituitary gland.

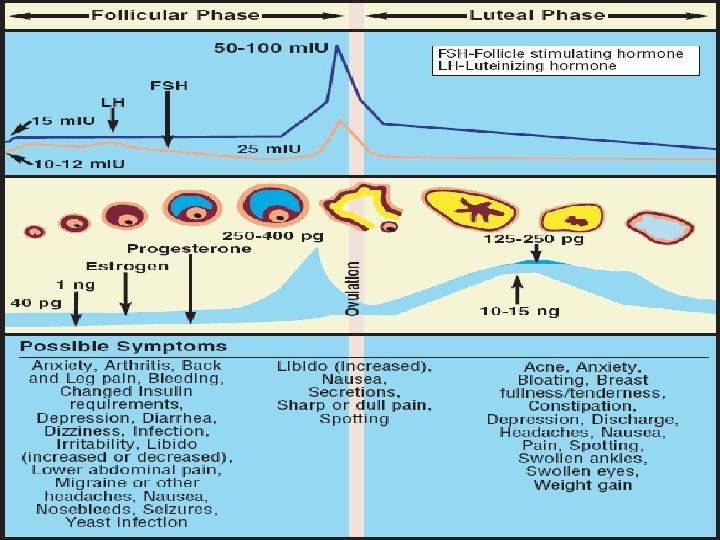
In women, the estradiol concentration necessary to achieve a positive feedback is more than 200 pg/ml and this concentration must be sustained for approximately 50 hrs. Pulsatile secretion of gonadotropins are more frequent but smaller in amplitude during follicular phase compared to the luteal phase with a slight increase in frequency observed as the follicular phase progress to ovulation.

Follicular Growth and Development in the Primate ovary Autocrine – paracrine peptides , not estrogen play the major role in regulating ovarian follicle growth and development in the primate. In the early follicular phase activin produced by granulosa in immature follicles enhances the action of FSH, an aromatase activity and FSH and LH receptor formation while simultaneously suppressing theca androgen synthesis.

Early Follicular Phase Activin FSH stimulation FSH and LH receptor formation
 Greater estrogen")
Late Follicular Phase Inhibin Androgen synthesis ( LH and IGF – 2) Greater estrogen production in granulosa
 Activin Premature Luetinization and progesterone production.")
Preovulatory Follicle (prevents) Activin Premature Luetinization and progesterone production.

• Inhibin B • Suppress FSH • Ensures the dominance of a single follicle

The Preovulatory Follicle Granulosa cells in the preovulatory follicle enlarge and acquire lipid inclusions while theca becomes vacuolated and richly vascular , giving the preovulatory follicle a hyperemic appearance. During the late follicular phase , estrogen rise slowly at first , then rapidly , reaching a peak approximately 24 -36 hrs prior to ovulation. Acting through its own receptors LH promotes luteinization of the granulosa in the dominant follicle , resulting in production of progesterone.

� An increase in progesterone can be detected in the venous effluent of the ovary bearing the preovulatory follicle as early as day 10 of the cycle. � The preovulatory period is associated with a rise in plasma levels of 17 alpha hydroxyprogesterone. � A mid cycle increase in local and peripheral androgens occurs derived from theca tissue of lesser unsuccessful follicles.

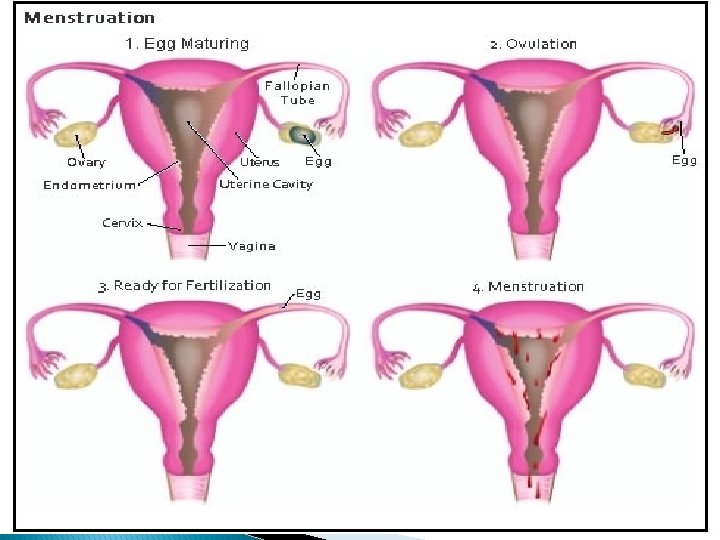
OVULATION The preovulatory follicle, through the elaboration of estradiol , provides its own ovulatory stimulus. � A reasonable and accurate estimate places ovulation approximately 10 -12 hrs after the LH peak and 24 -36 hrs after peak estradiol levels are attained. � The onset of the LH surge appears to be the most reliable indicator of impending ovulation, occurring 34 -36 hrs prior to follicle rupture. �

Ovulation occurs more frequently in the right ovary compared with the left, and oocytes from the right ovary have a higher potential for pregnancy. � With the LH surge , levels of progesterone in the follicle continue to rise up to the time of ovulation. � The progressive rise in progesterone may act to terminate the LH surge as a negative feedback effect is exerted at higher concentration. �

� FSH , LH , and progesterone stimulate the activity of proteolytic enzyme resulting in digestion of collagen in the follicular wall and increasing its distensibility. � The granulosa and theca cells produce plasminogen activator in response to gonadotropin surge. � Plasminogen activator produced by granulosa cells activate plasminogen in the follicular fluid to produce plasmin.

� Plasmin in turn generates active collagenase to disrupt the follicular wall. � Ovulation is the result of proteolytic digestion of the follicular apex , a site called the stigma � Prostaglandin E 2 and F 2 alpha , but mainly prostaglandin E 2 and other eicosanoids increase markedly in the preovulatory follicular fluid in response to the LH surge reaching a peak concentration at ovulation.

� The ovulatory role of prostaglandin is so well demonstrated that the infertility patients should be advised to avoid the use of drugs that inhibit prostaglandin synthesis. � The granulosa cells attached to the basement membrane and enclose the follicle become luteal cells. � The mechanism that shuts off the LH surge is unknown. Within hours after the rise in LH , there is a precipitous drop in the plasma estrogens. � Suppression of steroidogenesis at midcycle prevented ovulation , but not resumption of oocyte meiosis.

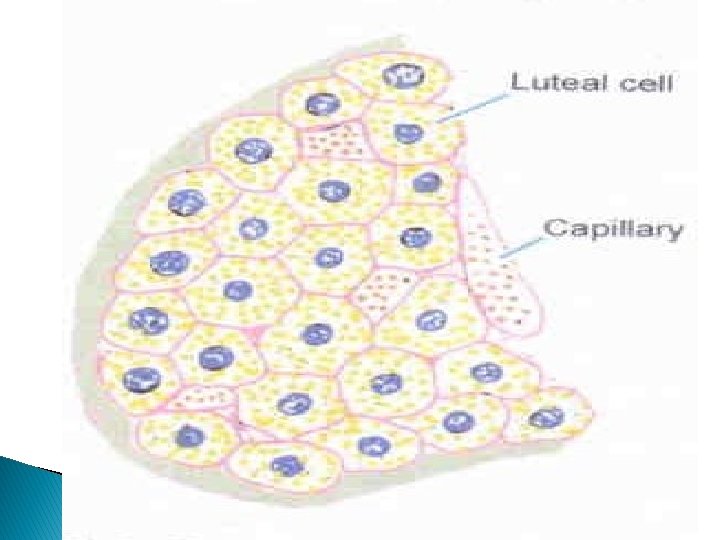
THE LUTEAL PHASE Before rupture of the follicle and release of the ovum , the granulosa cells begin to increase in size and assume a characteristic vacuolated appearance associated with the accumulation of a yellow pigment , luetin, which lends its name to the process of luteinization and the anatomical subunit corpus luteum. Ø By day 8 or 9 , a peak of vascularization is reached, associated with peak levels of progesterone and estradiol in the blood. � The corpus luteum has one of the highest blood flows per unit mass in the body. Ø

� Normal luteal function requires optimal preovulatory follicular development. � Progesterone level normally rise sharply after ovulation , reaching a peak approximately 8 days after the LH surge � In the normal cycle the time period from the LH midcycle surge to menses is consistently close to 14 days. � The corpus luteum rapidly declines 9 -11 days after ovulation , and the mechanism of the degeneration remains unknown.

� The lifespan and the steroidogenic capacity of the corpus luteum are dependent on continued tonic LH secretion. � The survival of the corpus lutuem is prolonged by the emergence of a new stimulus of rapidly increasing intensity , h. CG. � The early luteal phase is marked by active angiogenesis mediated by VEGF. � New vessel growth is held in check by angiopoietin -1 working through its receptors Tie-2 on endothelial cells.
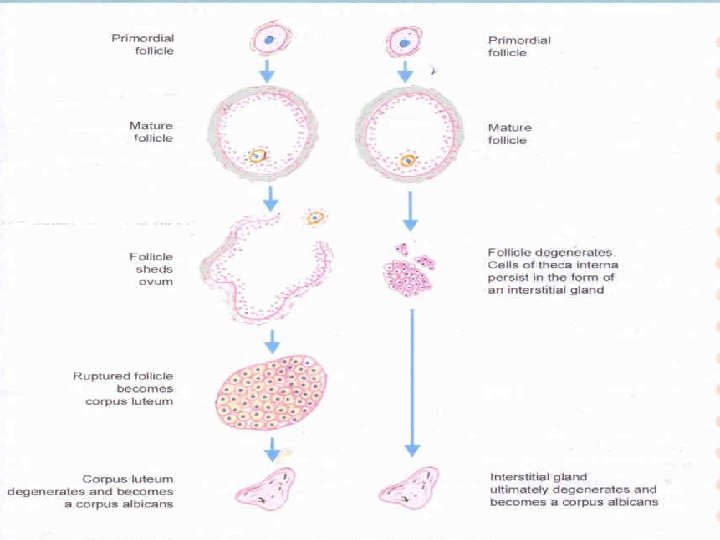

Corpus luteum fate � 1. 2. 3. 4. Unfertilised Last for 14 days. Secretes progesterone Called as CORPUS LUTEUM OF MENSTRUATION. Fibrous mass corpus albicans. � Fertilised 1. 2. 3. Last for 3 -4 months. Secretes progesterone till 4 th month. Called as CORPUS LUTEUM OF PREGNANCY.

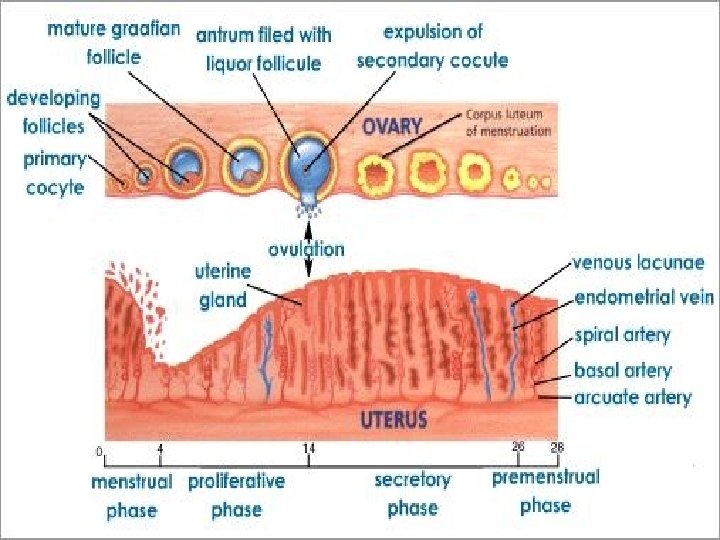
ENDOMETRIAL CYCLE � Endometrium – Basal zone � Functional Zone. � Basal zone – It forms 1/3 rd of the total zone. � It is uninfluenced by hormones and measures about 1 mm. � It consist of stromal cells , basal & base of endometrial glands. � It does not shed during menses & regeneration occurs from this layer.

� Functional Zone – This zone is under the influence of fluctuating oestrogen & progesterone. � It shows changes according to level of these hormones and hence divided as � REGENERATIVE PHASE. � PROLIFERATIVE PHASE � SECRETORY PHASE � MENSTRUAL PHASE

Regenerative Phase � It starts before menstruation ceases and completed 2 -3 days after the end of the menstruation. � Cubical surface epithelium is developed from stromal cells and gland lumina. � Glands. Arteries , stromal cells develop from their respective remenants. � Thickness – 2 mm

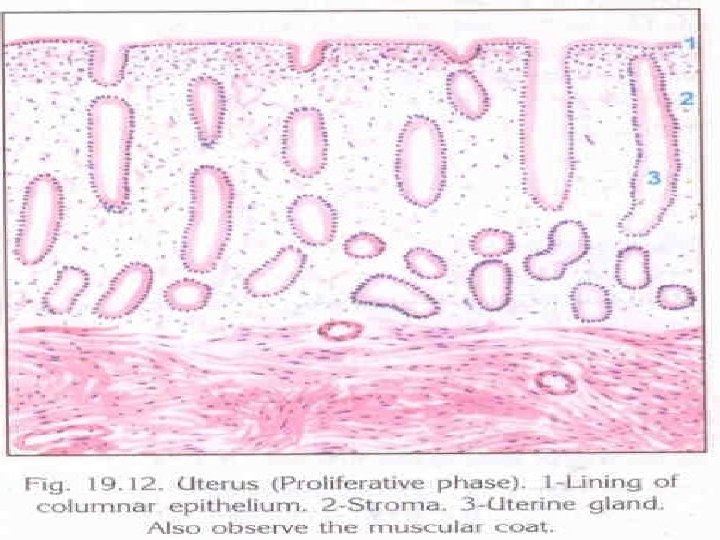
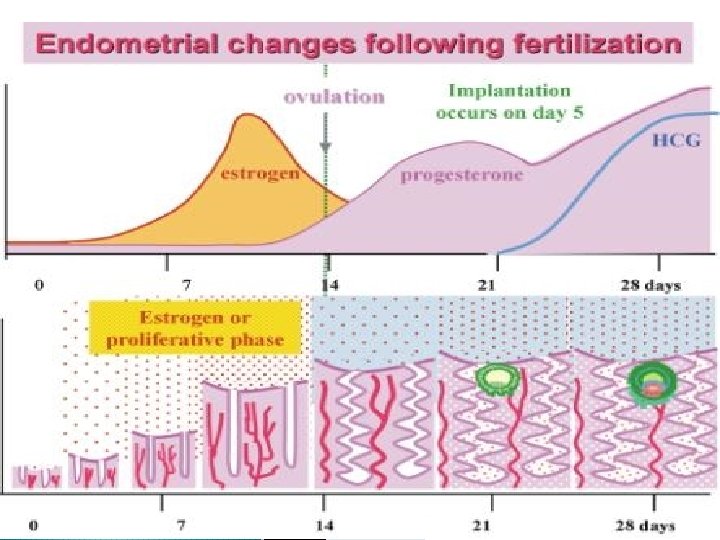
Proliferative Phase � IT starts from 5 th-6 th day to 14 th day. � Thickness – 3 -4 mm. � Its under the effect of rising oestrogen. � The gland become tubular and lie perpendicular to the surface. � Epithelium becomes columnar with nuclei at the bases. � Stromal cells are compact and spindle shaped � Spiral vessels extend unbranched upto a region below endometrium and form a loose capillary network.

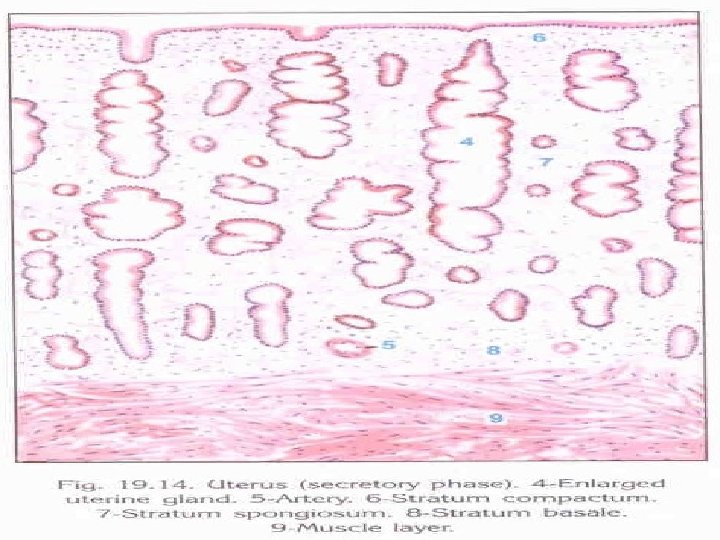
Secretory Phase � It is under effect of both oestrogen and progestrone. but, progesterone can only act on the endometrium previously primed by oestrogen. � Begins on the day 15 and ceases 5 -6 days prior to menstruation. � There occurs stimulation of glycogen in cells called subnuclear vacuolation , earliest sign of ovulation. � The endometrial growth ceases 5 -6 days prior to menstruation in an infertile cycle. � The regressive changes in the endometrium are pronounced 24 -48 hrs prior to menstruation.

Menstrual Phase � Withdrawal of hormones and regression of corpus luteum occurs. � Dengeneration and casting of the endometrium

Mechanism Vessels degenerative changes Stasis of blood Spasm of arterioles, damage to wall

Escape of blood through damaged walls Stromal hematoma Separation of superficial layer and release of proteolytic enzymes

Blood coagulates in uterine cavity liquefies by action of plasmids
 myometrial contraction & prolonged vasoconstriction � 2) clots formation")
Menstrual flow stops � 1) myometrial contraction & prolonged vasoconstriction � 2) clots formation by local aggregation of platelets & fibrin deposition � 3) repair of endometrium

THANK YOU
- Slides: 55