Normal and Abnormal Growth Nancy J Charest MD

Normal and Abnormal Growth Nancy J. Charest, MD Pediatric Endocrinology Children’s Hospital at Dartmouth

Normal and Abnormal Growth Outline u Review the endocrine control of growth u Discuss patterns of normal growth u Outline clinical evaluation of growth disorders u Illustrate some causes of growth failure

Endocrine Regulation of Growth

Endocrine Regulation of Growth
 Somatostatin (inhibits GH secretion) Ghrelin")
Endocrine Regulation of Growth Hormone: GRF (stimulates GH secretion) Somatostatin (inhibits GH secretion) Ghrelin (stimulates GH secretion) Insulin-like growth factors (IGF-I and IGF-II) Produced in response to growth hormone Mediates most of the effects of growth hormone Binds in serum to insulin-like growth factor binding proteins (IGFBP 3) Thyroid Hormone Gonadal steroids ( estradiol and testosterone) Glucocorticoids
 Somatostatin (-) Growth Hormone")
Endocrine Regulation of Growth Hypothalamus Pituitary Liver, Mesenchyma GRF (+) Somatostatin (-) Growth Hormone Insulin Like Growth Factor 1 Bone and Cartilage

GH/IGF-1 AXIS

Endocrine Regulation of Growth u Thyroid hormone – Skeletal growth is exquisitely sensitive to thyroid hormone – Hypothyroidism impairs growth hormone release – Hypothyroidism delays bone maturation and limits linear growth – Hyperthyroidism accelerates linear growth and bone maturation

Endocrine Regulation of Growth u Gonadal steroids – Estrogen and testosterone accelerate linear growth – Both hormones work synergistically with growth hormone – Bone maturation appears to be due to estrogen (aromatized from circulating androgens in males)

Normal Growth

Stages of Human Growth u Fetal u Infancy u Childhood u Pubertal
 – Not")
Stages of Human Growth u Fetal – Extraordinary growth rates (120 cm/yr!) – Not dependent on fetal pituitary » (anencephalic infants are born at normal size) – IGF-1 and IGF-II play a role in fetal growth – Highly dependent on maternal/placental factors » e. g. mult. pregnancy, placental insufficiency, maternal diabetes

Stages of Human Growth u Infancy – Rates are initially quite high, but decelerate rapidly » 40 cm/yr down to 12 cm/yr – Transition towards pituitary dependent growth » IGF-I, mediated by growth hormone becomes increasingly important – May be a crossing of percentiles during 1 st 2 yrs of life as genetic influences in stature manifest

Stages of Human Growth u Childhood – Slowly progressive fall in growth rate from 8 cm/yr to 5 cm/yr just before puberty – Children generally track along percentiles – Exquisitely sensitive to growth hormone and thyroid hormone – Minimal (if any) effect of sex hormones

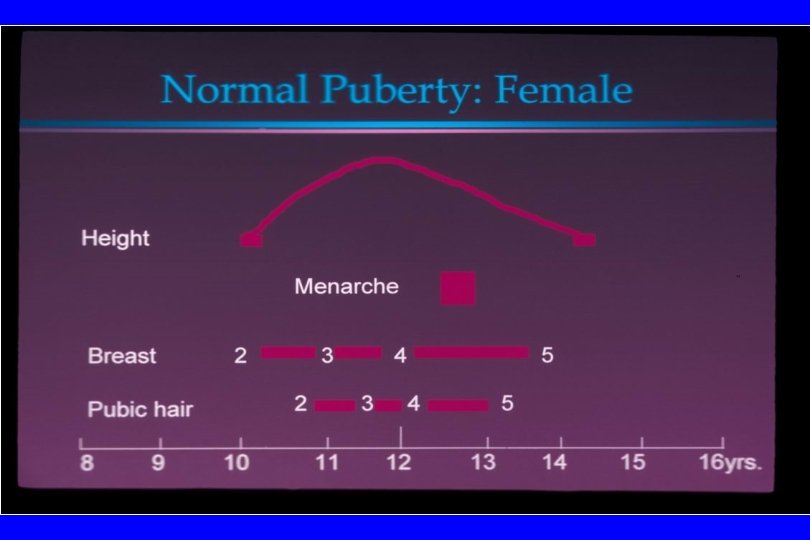
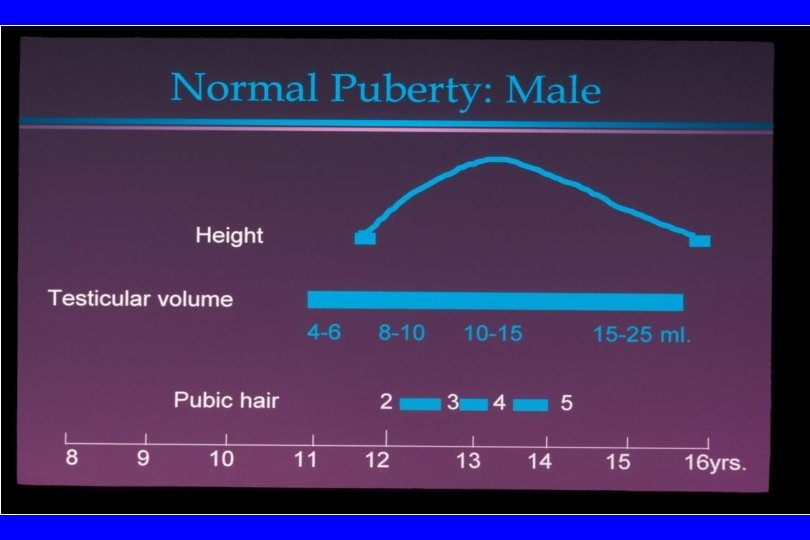
Stages of Human Growth u Pubertal – Rapid rise in growth rate due to sex hormones – Sex hormones have direct effect on linear growth, and also increase the production of growth hormone and IGF-I

Growth Velocity-Girls

Growth Velocity - Boys

Evaluation of Growth

Key Issues for PCP in evaluating growth u Accurate height and weight u Plotting of height and weight for age u Growth rate u Genetic height potential: mid-parental height calculation u Pubertal status

Correct technique to measure infant

Inconsistent measuring technique

Correct technique for measuring child

Infant Growth Charts

Children Growth Charts

Longitudinal growth chart Individual data obtained over time and pooled Note the sigmoid shape during puberty
 0 -1 Growth rate (cm/year) 18 -20")
Expected growth rates in children Age (years) 0 -1 Growth rate (cm/year) 18 -20 1 -2 8 -10 2 -4 4 -puberty 5 -7 4 -5

Growth Failure-Crossing percentiles

Growth Failure- Growth Velocity under 4 cm/year
 – For a male, add 5 inches")
Evaluation of Growth Mid-parental height (target height) – For a male, add 5 inches to mother’s height, add father’s height and divide by 2. – For a female, subtract 5 inches from father’s height, add mother’s height and divide by 2. – Children will normally fall within about 3. 5 inches of the target height
/2)=73 in +/- 3. 5 in (69. 5")
Father=74 inches, Mother= 67 inches. MPH= (74+67+5)/2)=73 in +/- 3. 5 in (69. 5 -76. 5 in)

Growth Failure and Short Stature u u u Short stature: height more than 2. 0 SD below the mean for age and gender Growth failure: decline in rate of linear growth (cross channels) Short for family: (More than 3 inches below mid-parental height percentile) Growth Hormone Research Society recommends investigation of children with the above noted definitions of growth failure/short stature Referral to pediatric endocrinologist is usually indicated.
 u Bone age u")
Evaluation of growth failure/short stature (usually performed by pediatric endocrinologist) u Bone age u Laboratory testing
 – indirect measure of the completeness")
Evaluating Growth-Bone Age u Skeletal maturation (“bone age”) – indirect measure of the completeness of endochondral ossification – correlates with growth potential – closely correlates with pubertal progression – mediated by estrogens

6 yr M 8 yr M 10 yr M

Evaluating Growth u Predicting adult stature based on bone age – Estimate skeletal age from radiograph – Read proportion of adult height complete from tables (Greulich and Pyle) – Divide current height by the proportion of growth complete

CA 8 yrs Bone age 8 yrs Ht. Pred. 70”

CA 8 yrs Bone age 6 yrs Ht prediction 74”

CA 8 yrs Bone age 10 yrs Ht. Prediction 67”

Screening labs for growth failure u IGF-1 u IGF-BP 3 u TSH, free T 4 u Karyotype in female or dysmorphic child u CBC with differential u ESR u Chemistry profile u Urinalysis u Celiac screen(Ig. A, t. TG Ig. A Ab)

Growth Disorders u Normal variants of growth u Endocrine causes of growth failure u Non-endocrine causes of growth

Familial short stature u Consistent growth pattern at lower edge of height curve u Parents are short u Growth pattern, bone age, and puberty are appropriate for chronologic age u Calculate mid-parental height or target height: – Girl = {[Fa-5 in] + Mo}/2 – Boy = {[Mo+5 in] + Fa}/2

Familial Short Stature

Constitutional growth delay u Family history of late onset puberty and slow growth until late adolescence u Normal annual growth rate for delayed bone age u Delayed puberty u Predicted height in range for family u No evidence of disease

Constitutional Delay of Growth

Growth Disorders Endocrine disorders that cause growth failure u Growth hormone deficiency u IGF-I deficiency u Hypothyroidism u Hypogonadism u Precocious puberty

Endocrine disorders that cause growth failure: Growth hormone deficiency u Decreased linear growth u Hypoglycemia (in infancy) u Increased adiposity (ripply abdominal fat) u Bone age typically delayed u Weight relatively well preserved (cherubic)

ER Growth Hormone Deficiency

Growth hormone deficiency

Endocrine Disorders that cause Growth Failure: Growth Hormone Deficiency u Making the diagnosis of GH/GRF deficiency – Document a low growth velocity – Exclude non-endocrine causes (CBC, ESR, UA, Chem panel) – Exclude hypothyroidism – Determine skeletal age – Measure IGF-I and IGFBP-3 (low levels support the diagnosis, but are not necessarily diagnostic)

Endocrine Disorders that cause Growth Failure: Growth Hormone Deficiency u Because GH secretion is pulsatile, random values are not helpful. u Most rely on provocative tests: – Insulin induced hypoglycemia (“gold standard”) – Arginine infusion – L-Dopa, clonidine, glucagon – GHRH

JT Growth Homone Deficiency

Endocrine Disorders that cause Growth Failure: Growth Hormone Deficiency u Causes – Idiopathic – Tumors (particularly craniopharyngioma) – Radiation – Genetic syndromes » Defects in growth hormone gene » Septo-optic dysplasia » Prop-1 mutation

Magnetic resonance imaging of large peri-sellar mass

Endocrine Disorders that cause Growth Failure: IGF-I deficiency u IGF-I deficiency – Defects in growth hormone receptor (Laron dwarfism) – Low levels of growth hormone binding protein (extracellular domain of the GH receptor) – High levels of growth hormone – Low levels of IGFs – Resistant to growth hormone treatment – Responsive to IGF-I infusion
")
IGF-1 Deficiency (Laron Dwarfism)

Growth Disorders Hypothyroidism Much more common than growth hormone deficiency Marked decrease in growth velocity (“crossing percentiles”) Epiphyseal fusion is delayed, preserving some growth potential Weight is well preserved or excessive Diagnosis can usually be suspected by associated signs/symptoms: cold intolerance, constipation, fatigue, bradycardia, goiter.

JR hypothyroidism

Growth Disorders Hypogonadism Without sex hormones, the pubertal growth spurt is blunted. Because epiphyseal fusion is delayed, growth continues well past puberty There are disproportionately long arms and legs a “eunuchoid body habitus”

Growth Disorders Precocious puberty results in rapid, early growth spurt There is rapid acceleration of bone age, premature fusion of growth plates, compromising adult stature

Non-Endocrine Causes of Growth Failure u Osteochondrodysplasias: - achondroplasia / hypochondroplasia u Chromosomal disorders - Turner’s syndrome, Down’s syndrome u Malabsorption – Celiac disease; Inflammatory bowel disease u Hypoxia – Cystic fibrosis, cyanotic heart disease, anemia u Iatrogenic

TM Turner Syndrome

Turner Syndrome: 45 XO / mosaic u u u Short stature due to SHOX mutation Gonadal failure, female phenotype Cubitus valgus Madelung deformity of distal radius/wrist Short, webbed neck Shield chest, wide-spaced nipples, atrophic breasts Low nuccal hairline Nevi Cardiac lesions: typically aortic coarctation & hypertension Renal lesions: typically horseshoe kidney Celiac disease Autoimmune thyroid disease

Normal and Abnormal Growth Summary u Growth is mediated primarily through the action of IGFI, which is stimulated by pituitary growth hormone secretion. u Thyroid hormone , estrogen and testosterone interact with the GH/IGF-I axis and play important roles in human growth u The timing of sex hormone secretion can have profound effects on final height, by altering the maturation of the growth plates

Normal and Abnormal Growth Summary u The PCP should accurately measure height and weights, plot data on growth charts, and calculate mid-parental height. u PCP should know that from age 2 years until puberty, children should maintain their height along the same percentile. u PCP should be able to assess growth rate in context of pubertal status.

Normal and Abnormal Growth Summary u Children who are: 1. more than 2 SD below the mean for height, or 2. crossing height percentiles over time or 3. short compared to parents, should be evaluated for a growth disorder by a pediatric endocrinologist.
- Slides: 67