NON MALIGNANT LESIONS OF ORAL CAVITY DR DEEPIKA





 or malabsorption (poor absorption of nutrients")
 is the recurrent appearance of mouth ulcers")

 of the lips. � In children")


 hypersensitivity reaction - when")

















Primary--lesions exclusively on the oral and perioral area, � Five")







 infection.")
 and electron")
 � Definition-ranula is an")


















 or congenital (rare). � Acquired syphilis is classified as")
 , macular syphilids, and condylomata lata (rare).")




 �")




- Slides: 72
NON MALIGNANT LESIONS OF ORAL CAVITY DR DEEPIKA PATIL
STOMATITIS Greek word- “stoma means mouth , itis means inflammation” Definition-Inflammation of mouth and lips affecting the mucus membrane with or without oral ulcers. Gingivostomatitis- Gums and mucus membrane.
Organisms causing Bacteria� Streptococcus viridans � Staphylococcus aureus � Haemophilus aphrophilus � Aggregatibacter � Actinomycetemcomitans � Cardiobacter hominis � Eikenella corrodens � Kingella kingae
Virus� Human herpes virus-1 � Human papillomavirus-16 � Coxsackievirus Fungii� Candida albicans
Predisposing factors � Bitting cheeks/tongue � Chewing tobacco � Allergy � Waring dentures � Consuming hot food/drink and spicy items � Nutritional deficiency � Immunosuppressed � Chemotherapy � Radiotherapy � Diabetes mellitus � HIV infection � Tuberculosis � Autoimmune disease like lupus, crohn’s disease, behcet’s disease.
TYPES Nutritional deficiency � Malnutrition (improper dietary intake) or malabsorption (poor absorption of nutrients into the body). � Deficiencies of iron, vitamin B 2 (riboflavin), vitamin B 3 (niacin), vitamin. B 6 (pyridoxine), vitamin B 9(folic acid) or vitamin B 12 (cobalamine) may all manifest as stomatitis. � Iron is necessary for the upregulation of transcriptional elements for cell replication and repair. Lack of iron cause genetic downregulation of these elements, leading to ineffective repair and regeneration of epithelial cells, especially in the mouth and lips.
Aphthous stomatitis � Aphthous stomatitis (canker sores) is the recurrent appearance of mouth ulcers in otherwise healthy individuals. � The cause is not completely understood. � T cell mediated immune response which is triggered by a variety of factors. � Ulcers (aphthae) recur periodically and heal completely. � More severe forms- new ulcers may appear in other parts of the mouth before the old ones have finished healing. � Most common diseases of the oral mucosa. � Incidence 20%
Treatment -no cure and therapies are aimed at alleviating the pain, reducing the inflammation and promoting healing of the ulcers, but there is little evidence of efficacy for any treatment that has been used
Angular stomatitis � Inflammation of the corners (angles) of the lips. � In children a frequent cause is repeated lip-licking, and in adults it may be a sign of underlying iron deficiency anemia, or vitamin B deficiencies. � Patient's jaws at rest being 'overclosed' due to deformity or tooth wear, causing the jaws to come to rest closer together than if the complete/unaffected dentition were present. � This causes skin folds around the angle of the mouth which are kept moist by saliva, which in turn favours infection; mostly by candida albicans or similar species.
Treatment usually involves the administration of topical nystatin or similar antifungal agents
Denture-related stomatitis � Reddened but painless mucosa beneath the denture. 90% of cases are associated with candidia species, and it is the most common form of oral candidiasis. � Treatment is by antifungal medication and improved dental hygiene, not wearing the denture during sleep.
Allergic contact stomatitis/allergic gingivostomatitis/allergic contact gingivostomatitis � Type IV (delayed) hypersensitivity reaction - when allergens penetrate the skin or mucosa. � Allergens--combine with epithelial-derived proteins, forming haptens which bind with langerhans cells in the mucosa, which in turn present the antigen on their surface to T ymphocytes, sensitizing them to that antigen and causing them to produce many specific clones.
� Mouth is coated in saliva, which washes away antigens and acts as a barrier. � The oral mucosa has a better blood supply than skin. � Less keratin in oral mucosa , meaning that there is less likelihood that haptans will form. � Non-specific inflammation, burning or soreness of the mouth and ulceration. � Chronic exposure --lichenoid lesion.
Common allergens� Cinnamaldehyde, � Peppermint, � Mercury, � Gold, � Pyrophosphates, � Zinc citrate, � Free acrylic monomer, � Nickel, and � Sodium lauryl sulfate etc. �Patch test
Migratory stomatitis/geographic stomatitis/stomatitis areata migrans � Is an atypical presentation of a condition which normally presents on the tongue, termed geographic tongue. � Geographic tongue is so named because there atrophic, erythematous areas of depapillation that migrate over time, giving a map-like appearance. � In migratory stomatitis, other mucosal sites in the mouth, such as the ventral surface (undersurface) of the tongue, buccal mucosa, labial mucosa, soft palate, or floor of mouth may be afflicted with identical lesions, usually in addition to the tongue.
HERPES STOMATITIS Primary herpetic gingivostomatitis � Relatively common � Etiology -herpes simplex virus type 1 (HSV-1), and rarely type 2 (HSV-2). � Clinical features � Age --6 months and 6 years. � Abrupt onset, � High fever, headache, malaise, anorexia, irritability, bilateral sensitive regional lymphadenopathy, and sore mouth lesions. � The affected mucosa is red and edematous, with numerous coalescing vesicles, which rapidly rupture, leaving painful small, round, shallow ulcers covered by yellow fibrin.
� The ulcers heal in 10– 14 days. � Both the movable and nonmovable oral mucosa may be affected. � Gingival lesions are almost always present, resulting in enlargement and edematous and painful erosions. � Diagnosis-clinical grounds. � Laboratory tests -smear, biopsy, serological tests. � Treatment- symptomatic. � In severe cases, systemic aciclovir or � valaciclovir.
Secondary herpetic stomatitis Definition and etiology -relatively common due to reactivation of HSV-1. � It is commonly precipitated by fever, trauma, cold, heat, sunlight, emotional stress, and HIV infection. Clinical features -the most common sites --lips and perioral skin, the palate, and the attached gingiva. � Lesions present as multiple small vesicles arranged in clusters � The vesicles soon rupture, leaving small ulcers that heal spontaneously within 6– 10 days.
� Prodromal symptoms are burning, itching, tingling, and erythema. � Characteristically, fever, generalized regional lymphadenopathy, and constitutional symptoms are absent. � Treatment -symptomatic
Herpes zoster Definition-is an acute self-limiting viral disease. Etiology -reactivation of varicella-zoster virus. � Predisposing factors -Aids, leukemia, lymphoma and other malignancies, radiation, immunosuppressive and cytotoxic drugs, and old age. Clinical features – � The thoracic, cervical, trigeminal, and lumbosacral dermatomes are most commonly affected, characteristically one dermatome. � Pain and tenderness, headache, malaise, and fever, are prodromal symptoms before the appearance of oral or skin lesions, or both. � After two to four days, clusters of vesicles develop, and within two or three days evolve into pustules and ulcers, covered by crusts.
� The lesions persists for two to three weeks. � Unilateral location—typical pattern of herpes zoster. � Oral manifestations occur when the second and third branches of the trigeminal nerve are involved. � Postherpetic trigeminal neuralgia is a common complication, and rarely osteomyelitis, jawbone necrosis, and tooth loss are seen. � Treatment- analgesics and sedatives to control the pain. � Aciclovir, valaciclovir, and famciclovir.
Nicotinic Stomatitis � Definition--is a common tobacco- related type of keratosis that occurs exclusively on the hard palate, and is classically associated with heavy pipe and cigar smoking. � Etiology -The elevated temperature, rather than the tobacco chemicals, is responsible for this lesion. � Clinical features –redness, wrinkled and takes on a diffusely grayish-white color, with numerous micronodules with characteristic punctate red centers, which represent the inflamed and dilated orifices of the minor salivary gland ducts.
� The lesions are not premalignant, in contrast to the “reverse smoker’s palate” lesion, which is associated with reverse smoking. � Laboratory tests-not required. � Treatment-Cessation of smoking.
Uremic Stomatitis � Definition- rare disorder that may occur in acute or chronic renal failure. � Etiology- increased concentration of urea and its products in the blood and saliva. � Pathogenesis --not clear. � Blood concentration of urea exceeds 30 mmol/1. � The degradation of oral urea by the enzyme urease forms free ammonia, which may damage the oral mucosa. � Clinical features- four forms (a) the ulcerative form, (b) the hemorrhagic form, (c) the nonulcerative, pseudomembranous form- as painful diffuse erythema covered by a thick whitish-gray pseudomembrane. (d) the hyperkeratotic form-presents as multiple painful white hyperkeratotic lesions with thin projections.
� The tongue, and the floor of the mouth are more frequently affected. � Xerostomia, foul breath odor, unpleasant taste, and a burning sensation are common symptoms. � Treatment- the oral lesions usually improve after hemodialysis. � Oral hygiene, mouthwashes with oxygen release agents, and artificial saliva. � Antimycotic, antiviral, and antimicrobial agents if necessary.
Cinnamon Contact Stomatitis � Definition-common oral mucosal reaction to continuous contact of substances with cinnamon. � Etiology-artificial cinnamon flavoring especially in the form of chewing gum, candies, toothpaste, drops, etc. � Clinical features-erythema of the oral mucosa, desquamation and erosions. � White hyperkeratotic plaques are very common. � Burning sensation and pain. � The lateral borders of the tongue, the buccal mucosa, and the gingiva are more frequently affected.
� Exfoliative cheilitis and perioral dermatitis may occur. � Treatment -Discontinuation of any cinnamon product improves the Signs and symptoms in approximately two weeks. � In severe and extended lesions with erosions, low doses of steroids (e. g. , 10 mg/day � prednisolone) for one week help the lesions to heal.
CANDIDIASIS/MONILIAL INFECTION � Definition -most common oral fungal infection. � Etiology --Candida albicans, and � less frequently by � C. glabrata, � C. krusei, � C. tropicalis, � C. parapsilosis.
� Predisposing factors – � � � poor oral hygiene, xerostomia, mucosal damage, dentures, antibiotic mouthwashes and broad-spectrum antibiotics, steroids, immunosuppressive drugs, radiation, HIV infection, hematological malignancies, neutropenia, iron-deficiency anemia, cellular immunodeficiency, endocrine disorders.
�Clinical features- classified as 1)Primary--lesions exclusively on the oral and perioral area, � Five clinical varieties: � Pseudomembranous-most common, creamy-white, slightly elevated, removable spots or plaques , localized or generalized, and appear more frequently on the buccal mucosa, soft palate, tongue, and lips, Xerostomia, a burning sensation, and an unpleasant taste are the most common symptoms. � Nodular-chronic form of the disease, white, firm, and raised plaque that usually does not detach
� Eyrthematous � Papillary hyperplasia of the palate, and � Candida-associated lesions (angular cheilitis, median rhomboid glossitis, denture stomatitis). 2)Secondary—consisting of oral lesions of mucocutaneous disease. � Laboratory tests -cytology and tissue culture examination; biopsy only in chronic cases. � Treatment- Antifungal like flucanozole iv or oral.
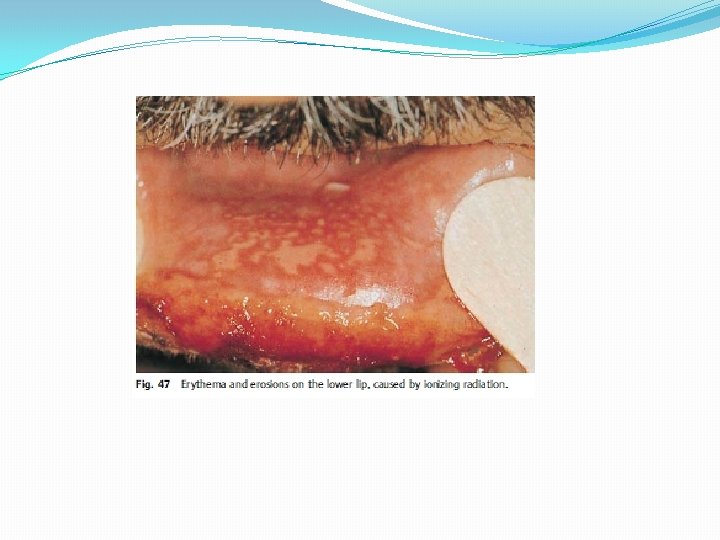
Radiation Mucositis � Definition and etiology--side effect of radiation treatment of head and neck tumors. � Clinical features --early and late. � Early reactions -first week of radiotherapy � erythema and edema of the oral mucosa. � erosions or ulcers covered by a whitish-yellow exudate. � Xerostomia, loss of taste, and burning and pain during mastication, swallowing, and speech are common. � Late -- 4 -5 weeks after radiation. � Treatment- Supportive. Cessation of the radiation. � B-complex vitamins, steroids.
ORAL MUCOSA HYPERKERATOSIS SYNDROME � Definition -This is a rare mucocutaneous disorder. � Etiology -Genetic. It is inherited as an autosomal dominant trait. � Clinical features-The main clinical manifestations are focal hyperkeratosis on the weight-bearing and pressure-related regions of the palms, soles, and oral mucosa. � The oral lesions present as white hyperkeratotic plaques (leukoplakia), mainly on the attached gingiva, the lateral border of the tongue, and the palate. � develop in early childhood. � Treatment -Supportive. Retinoids may be helpful.
LEUKOPLAKIA � Definition-leukoplakia is a clinical term, and the lesion is defined as a white patch or plaque, firmly attached to the oral mucosa, that cannot be classified as any other disease entity. � It is a precancerous lesion. � Etiology-unknown. Tobacco, alcohol, chronic local friction, and candida albicans and human papilloma virus (HPV) infection, six ‘S’. � Clinical features� Three clinical varieties � Homogeneous (common), � Speckled (less common), and � Verrucous (rare).
� Speckled and verrucous leukoplakia have a greater risk for malignant transformation than the homogeneous form. � Common in males (3: 1). � Malignant transformation --4% - 6%. � white or greyish coloured, well-localised patch. � Buccal mucosa and oral commissures are most common sites.
Incidence –smoker or pan chewer- 20%, whereas in non-smokers is 1%. Laboratory tests -histopathological examination. Histology: Parakeratosis with widening of rete pegs. Histological staging I. Acanthosis – elongation of rete pegs – smooth, white, dry patch II. Parakeratosis III. Widening of rete pegs IV. Dyskeratosis – keratin cell layer formation deep to epidermis V. Dysplasia VI. Carcinoma in situ
Treatment • Pan chewing and smoking has to be stopped. • Excision, if required skin grafting has to be done. • Regular follow-up is necessary. • Isoretinoin is helpful. Beta-carotene, tocoferol • CO 2 laser excision.
Hairy leukoplakia � Definition-most common and characteristic lesions of human immunodeficiency virus (HIV) infection. � Rarely, after organ transplantation. � Etiology --epstein–barr virus seems to play an important role in the pathogenesis. � Clinical features--white asymptomatic, often elevated and unremovable patch. Almost always found bilaterally on the lateral margins of the tongue, and may spread to the dorsumand the ventral surface. � The lesion is not precancerous.
� Laboratory tests- histological examination, in situ hybridization, polymerase chain reaction (pcr) and electron microscopy. � Treatment -not required; however, in some cases aciclovir or valaciclovir can be used with success.
RANULA (Rana = frog, ranula looks like belly of frog) � Definition-ranula is an extravasation cyst arising from sublingual gland or mucus glands of nuhn or glands of blandin in the floor of the mouth. � Occasionally--submandibular salivary gland. � Initially there is blockage of the duct (of sublingual gland) causing retention cyst, which causes rupture of the acini due to increased pressure leading into extravasation cyst. � Etiology --trauma or ductal obstruction.
� Clinical features � Presents as a bluish smooth, soft, fluctuant, brilliantly transilluminant swelling in the lateral aspect of the floor of the mouth. � The color ranges from normal to a translucent bluish, and the size is usually in the range of 1– 3 cm, or larger. � It often extends into the submandibular region through the deeper part of the posterior margin of mylohyoid muscle and is called as plunging ranula. � It is intraoral ranula with cervical extension. It is cross fluctuant across mylohyoid. � Diagnosis -- clinical
Treatment –marsupialization and excision or If ranula is small it can be excised without marsupialisation. Excision of sublingual salivary gland is often needed
SUBLINGUAL DERMOID CYST � Definition and etiology –they are sequestration dermoids lined by squamous epithelium containing keratin. Types 1. Median sublingual dermoid: it is derived from epithelial cell rests at the level of fusion of two mandibular arches. It may be supramylohyoid or inframylohyoid. � Located between two genial muscles, in relation to mylohyoid muscle. � Midline swelling which is smooth, soft, cystic, non-tender, nontransilluminant.
2. Lateral sublingual dermoid: it develops in relation to submandibular duct, lingual nerve and stylohyoid ligament. � Derived from first branchial arch, � Swelling in the lateral aspect of the floor of the mouth � Clinical features- it presents as a slow-growing, painless swelling with a normal or yellowish-red color and a characteristic soft doughlike consistency , few millimeters to 10 cm in diameter, and the lesion usually occurs in the midline of the floor of the mouth. � Difficulty in mastication, speech, and swallowing. � Treatment- surgical removal through oral route or submandibular route.
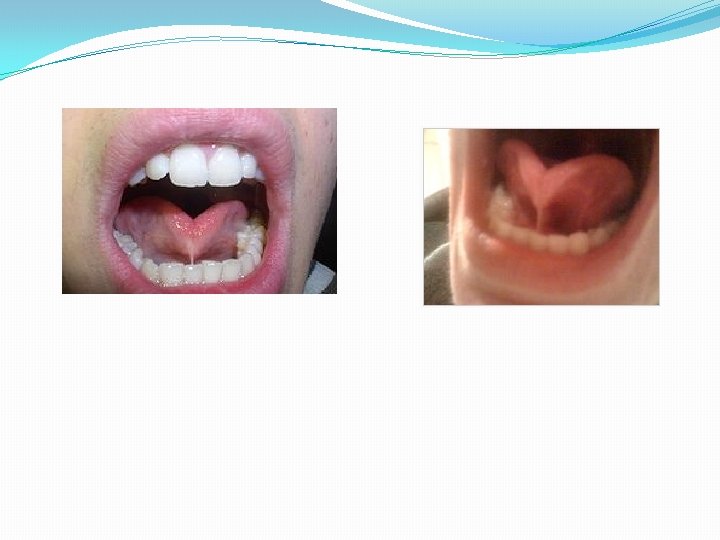
TONGUE TIE � Ankyloglossia-- is a congenital oral anomaly that may decrease mobility of the tongue tip and is caused by an unusually short, thick lingual frenulum, a membrane connecting the underside of the tongue to the floor of the mouth. � Ankyloglossia varies in degree of severity from mild cases characterized by mucous membrane bands to complete ankyloglossia whereby the tongue is tethered to the floor of the mouth.
Effects � Can affect feeding, speech, and oral hygiene as well as have mechanical/social effects. � Adversely affect breastfeeding in certain infants. � Do not, have such big difficulties when feeding from a bottle. � Prevent the tongue from contacting the anterior palate. � This can then promote an infantile swallow and hamper the progression to an adult-like swallow which can result in an open bite deformity. � It can also result in mandibular prognathism, this happens when the tongue contacts the anterior portion of the mandible with exaggerated anterior thrusts.
Speech � Phonemes likely to be affected due to ankyloglossia include sibilants and lingual sounds such as 'r’. � Common speech abnormalities include mispronunciation of words, the most common of which is pronouncing l as w; for example, the word "lemonade" would come out as "wemonade".
Diagnosis � Difficult; it is not always apparent by looking at the underside of the tongue, but is often dependent on the range of movement permitted by the genioglossus muscles. � For infants, passively elevating the tongue tip with a tongue depressor may reveal the problem. For older children, making the tongue move to its maximum range will demonstrate the tongue tip restriction. In addition, palpation of genioglossus on the underside of the tongue will aid in confirming the diagnosis. � A severity scale for ankyloglossia, which grades the appearance and function of the tongue, is recommended for use in the academy of breastfeeding medicine.
Intervention � Include surgery in the form of frenotomy (also called a frenectomy or frenulectomy) or frenuloplasty. � This relatively common dental procedure done by laser or cautery. � Patients --any age with a tight frenulum, as well as a history of speech, feeding, or mechanical/socia difficulties. � Wait-and-see approach. � Frenulum naturally recedes during the process of a child's growth between six months and six years of age.
EPULIS � Swelling arising from the mucoperiosteum of gums. � Means “on the gingiva” Congenital epulis/granular cell tumor/neumann’s tumor � Rare benign condition seen in a newborn arising from gum pads. � It is a variant of granular cell myoblastoma originating from gums. � Common in girls and upper jaw, (canine or premolar area). � It is not a malignant condition. Clinical feature � Well localised swelling from the gum which is firm and � Bleeds on touch. Treatment � Excision.
Fibrous epulis � Benign condition, can occur in any individual with caries tooth. � It is seen in the gum, adjacent to the caries tooth. � Sessile or pedunculated. � It is commonest type. � It is fibroma arising from periodontal membrane. Clinical features � Painless, well localised, hard, non-tender swelling in � The gum which bleeds on touch. � Caries tooth adjacent to the lesion.
Differential Diagnosis � Squamous cell carcinoma from the gum. Investigations � X-ray jaw. � Orthopantomogram � Biopsy from the lesion. Treatment � Excision with extraction of the adjacent tooth.
Pregnancy Epulis/granuloma gravidarum � It occurs in pregnant women due to inflammatory gingivitis � Usually during 3 rd month of pregnancy. � Clinically it resembles fibrous epulis or pyogenic granuloma. � It usually resolves after delivery. Otherwise it should be excised.
Myelomatous Epulis � It is seen in leukaemic patients. Investigated for leukaemia by peripheral smear, bone � marrow biopsy. Treatment: For leukaemia Granulomatous Epulis � It is a mass of granulation tissue in the gum around a caries tooth. It forms a localised soft/firm/fleshy mass in the gum which bleeds on touch.
Giant Cell Epulis � Osteoclastoma causing ulceration and haemorrhage of gum. Carcinomatous Epulis � Squamous cell carcinoma of the alveolus and gum presenting as localised, hard, indurated swelling with ulceration. Fibrosarcomatous Epulis � Fibrosarcoma arising from fibrous tissue of the gum.
DIFFERENTIAL DIAGNOSIS OF TONGUE ULCERS Traumatic/dental ulcers � Clinically diverse, but usually appear as a single, painful ulcer with a smooth red or whitish-yellow surface and a thin erythematous halo. � � They are usually soft on palpation, and heal without scarrin within 6– 10 days, spontaneously or after removal of the cause. � May clinically mimic a carcinoma. � The tongue, lip, and buccal mucosa � Diagnosis--history and clinical features. � Ulcer persists over 10– 12 days a biopsy must be taken to rule out cancer.
Syphilitic ulcer � Acquired (common) or congenital (rare). � Acquired syphilis is classified as primary, secondary and tertiary. � The characteristic lesion in the primary stage is the chancre that appears at the site of inoculation, usually three weeks after the infection. � Oral chancre appears in about 5– 10% of cases, and clinically presents as a painless ulcer with a smooth surface, raised borders, and an indurated base. � Regional lymphadenopathy is a constant finding. � The secondary stage begins 6– 8 weeks after the appearance of the chancre, and lasts for 2– 10 weeks.
� Oral lesions are mucous patches (common) , macular syphilids, and condylomata lata (rare). � Constitutional symptoms and signs (malaise, low-grade fever, headache, lacrimation, sore throat, weight loss, myalgias and multiple arthralgias, generalized lymphadenopathy) as well as cutaneous manifestations (macular syphilids, papular syphilids, condylomata lata, nail involvement, hair loss, atypical rash, etc. ) Are constant findings tertiary syphilis begins after a period of 4– 7 years. Oral lesions are gumma, atrophic or luteic glossitis, and interstitial glossitis. � The most common oral lesions in congenital syphilis are a high-arched palate, short mandible, rhagades, hutchinson’s teeth, and moon’s or mulberry molars.
Tubercular ulcer � The oral lesions are rare, and usually secondary to pulmonary tuberculosis. � Ulcer is the most common feature. � Clinically, the ulcer is painless and irregular, with a thin undermined border and a vegetating surface, usually covered by a gray-yellowish exudate. � The surrounding tissues are inflamed and indurated. � The dorsum of the tongue is the most commonly affected site, followed by the lip, buccal mucosa, and palate. � Osteomyelitis of the jaws, periapical granuloma, regional lymphadenopathy, and scrofula are less common oral manifestations.
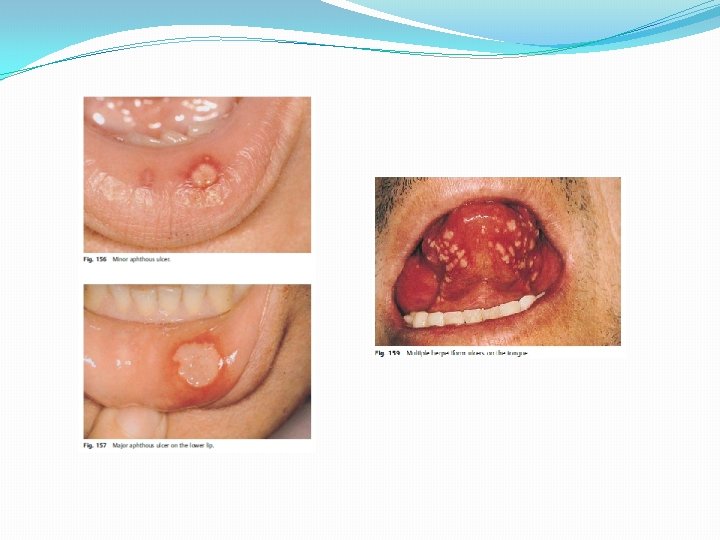
Aphthous ulcer � Minor, major and herpetiform ulcers. � Minor --small, painful, round ulcers 3– 6 m m in diameter, covered by a whitish-yellow membrane and surrounded by a thin red halo. � The lesions may be single or multiple (two to six), and they heal without scarring in 7– 12 days. � Major- deep painful ulcers, 1– 2 cmin diameter, that persist for 3– 6 weeks and may cause scarring , lesions 1 -5 � Herpetiform--small, painful, shallow ulcers, 1– 2 mm in diameter, with a tendency to coalesce into larger irregular ulcers. � Characteristically, the lesions are multiple (10– 100), persist for one or two weeks, and heal without scarring. � The non-keratinized movable mucosa is most frequently affected. � The diagnosis-- clinical criteria.
Malignant � Oral squamous-cell carcinoma � men : women (ratio 2 : 1) � Over 40 years of age. � varied clinical presentation, and may mimic several diseases. � Early--white lesion, a red lesion, or both, or even as an exophytic mass, the most common clinical presentation is an erosion or an ulcer. � irregular papillary surface, elevated borders, and a hard base on palpation. � chronic and indurated. � The lateral border, the ventral surface of the tongue, and the lips are the most commonly affected areas followed by the floor of the mouth, the gingiva, the alveolar mucosa, the buccal mucosa, and the palate. � The prognosis depends on the tumor stage and the histopathological pattern.
Eosinophilic ulcer � Painful inflammatory ulcers with an irregular surface, a raised border, and covered with a whitish-yellow pseudomembrane. � Single or multiple, and develop suddenly.
Leukemic ulcer � Acute and chronic, depending on the clinical course, and � Myeloid or lymphocytic, according to the histogenetic origin. � The main clinical signs and symptoms of leukemias are weakness, fatigue, weight loss, fever, chills, headache, night sweats, skin and mucous membrane pallor, bleeding, infections, bone pain, lymphadenopathy, splenomegaly, hepatomegaly, and salivary � Gland enlargement. � All forms of leukemia can have oral manifestations.
� The most common oral lesions are ulcerations , spontaneous gingival hemorrhage, petechiae, ecchymoses, tooth loosening, and delayed wound healing. � Gingival enlargement is a characteristic pattern, frequently seen in patients with myelomonocytic leukemia � Candidiasis and herpetic infections are relatively common oral complications of leukemia.