Non Invasive Ventilation and Mechanical Ventilation in the





 e.")

, OD, … everything except Asthma/COPD O 2 +/NIV/BPAP CO 2 Mode: S/T")











, OD, … everything except Asthma/COPD O 2 +/NIV/BPAP CO 2 Mode: S/T")





 = lung protection")





 = lung protection")

 = lung protection")










- Slides: 74
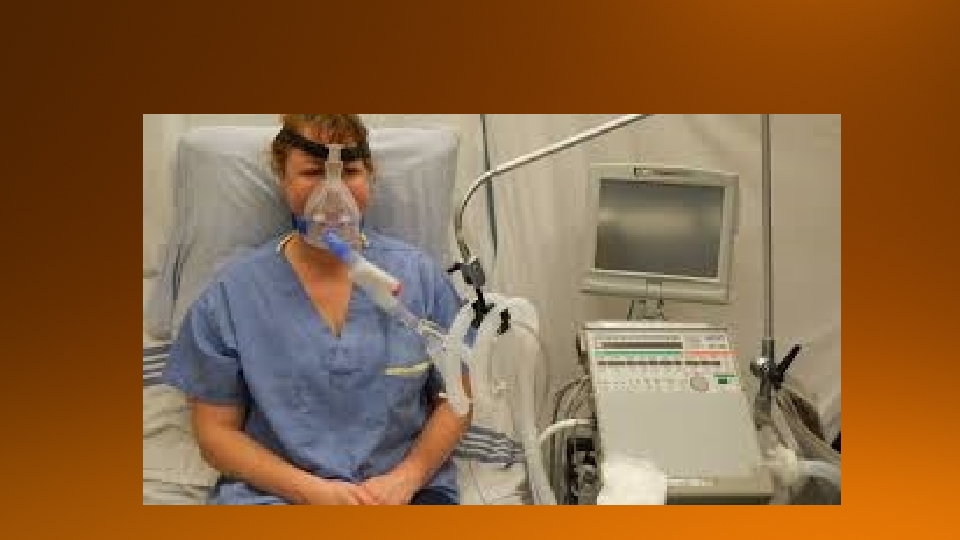
Non Invasive Ventilation and Mechanical Ventilation in the ER
A/C io Pa. CO 2 Fi. O 2 ure s s re P u a late P P A P BI RR PEEP at : I E r a Tid ual d i s Re me Volu Fo Ca rced pa V cit ita l y S ARD l IPAP SIMV me u l Vo A-a Bi. PAP gra dien t EPAP 2 Pa. O NIV IBW
Acute Pulm Edema, Pneumonia, OD, … Asthma/COPD everything except Asthma/COPD O 2 NIV/BPAP Mechanical Ventilation +/- CO 2 Type 1 CO 2 +/- O 2 Type 2 Mode: S/T PEEP 5 cm H 2 O IPAP(PSV) 5 - 10 cm H 2 O (max 20) Fi. O 2 100% Rate 14 (Backup Rate) Mode: S/T PEEP O cm H 2 O IPAP (PSV) 10 -15 cm H 2 O (max 20) Fi. O 2 40% Rate 14 (Backup Rate) Mode: A/C Volume Vt 6 -8 cc/kg IBW RR 18 bpm PEEP 5 cm H 2 O - initially Fi. O 2 100% - initially After 5 min, do ABG, follow ARDSnet chart Goal: Pa. O 2 55 -80 or Sa. O 2 90% Mode: A/C Volume Vt 8 cc/kg IBW RR 10 bpm PEEP O-4 cm H 2 O Fi. O 2 40% Goal: keep p. H above 7. 1
Acute Pulm Edema, Pneumonia, OD, … Asthma/COPD everything except Asthma/COPD O 2 +/- CO 2 Type 1 CO 2 +/- O 2 Type 2
Type 2 – failure of Ventilation = HYPERCAPNIA (“respiratory muscle fatigue” or “obstruction”) e. g. : COPD, Asthma Both Type 1 and 2 can be treated with non invasive or invasive (intubation) ventilation depending on patient condition
Remember Patients can obviously have combined failure!
APE, Pneumonia), OD, … everything except Asthma/COPD O 2 +/NIV/BPAP CO 2 Mode: S/T PEEP 5 cm IPAP (PSV) 5 - 10 Fi. O 2 100% (Backup) Rate 14 Asthma/COPD CO 2 +/- O 2 Mode: S/T PEEP O cm IPAP (PSV) 10 -15 Fi. O 2 40% (Backup) Rate 14
Don’t worry, PEEP, EPAP and IPAP will be explained later! For patients in the ER, we will be using “Bi-level” positive pressure settings on the Ventilator.
The way to fix this is to keep the alveoli ‘open’ during expiration to allow time for the oxygen to get into the vascular system. Easiest way to do this is to provide continuous pressure into the lung, especially during expiration. (often referred to as ‘splinting’ the alveoli)
Since it is positive pressure, we can call it: Continuous Positive Pressure. We can specify that the pressure is going into the airways, so lets call it : Continuous Positive Airway Pressure – ie CPAP.
Since it is during expiration, we could also call it: Expiratory Positive Airway Pressure – or EPAP So basically: CPAP = PEEP = EPAP (conceptually, not mathematically)
In this scenario, the patient needs inspiratory help So if the patient is awake and breathing, we can use “Bilevel” ventilation. We want both ‘Inspiratory Positive Airway Pressure’ (sometimes call “Pressure Support Ventilation – PSV) along (maybe) with ‘Expiratory Positive Airway Pressure’ This is called IPAP (PSV) and EPAP respectively.
So for both Type 1 and Type 2 Respiratory Failure all we need to know is how to set up the S/T Mode! Then if we want we can ‘finesse’ some of the settings or easier yet, call the RT!
Bi. PAP and BIPAP are registered trade names from Ventilator companies. So we should actually be using the terms “Bi Level” or “BPAP” Or make it really simple and call anyone on a mask as getting Non Invasive Ventilation (NIV)!
If you are a purest though, for Oxygenation failure, you really only need PEEP – so you could actually set the IPAP to equal EPAP For Ventilation failure, you really need IPAP, which is using the S/T mode and setting the PEEP very low or zero – why?
Patients needing NIV with COPD or Asthma 1. Use S/T mode with IPAP and EPAP or or 2. Use S/T mode but with low/nil EPAP setting, call the RT
APE, Pneumonia), OD, … everything except Asthma/COPD O 2 +/NIV/BPAP CO 2 Mode: S/T PEEP 5 cm IPAP (PSV) 5 - 10 Fi. O 2 100% (Backup) Rate 14 Asthma/COPD CO 2 +/- O 2 Mode: S/T PEEP O cm IPAP (PSV) 10 -15 Fi. O 2 40% (Backup) Rate 14
Push the start button on the ventilator
APE, Pneumonia, OD, … everything except Asthma/COPD O 2 +/- Mechanical Ventilation CO 2 Mode: A/C Volume Vt 6 -8 cc/kg IBW RR 18 bpm PEEP 5 cm Fi. O 2 100% After 5 min, do ABG, follow ARDSnet chart Goal: Pa. O 2 55 -80 or Sa. O 2 90% Asthma/COPD CO 2 +/- O 2 Mode: A/C Volume Vt 8 cc/kg IBW RR 10 bpm PEEP O-4 cm Fi. O 40% Goal: keep p. H above 7. 1
The ‘control’ is that we set the rate, volume etc. The assist part is if the patient is able or does take an extra breath, that is fine. The ventilator will give an additional breath at whatever parameters we have set.
APE, Pneumonia, OD, … everything except Asthma/COPD O 2 +/- Mechanical Ventilation CO 2 Asthma/COPD CO 2 +/- O 2 Mode: A/C Volume Vt 8 cc/kg IBW RR 10 bpm PEEP O-4 cm Fi. O 40% Goal: keep p. H above 7. 1
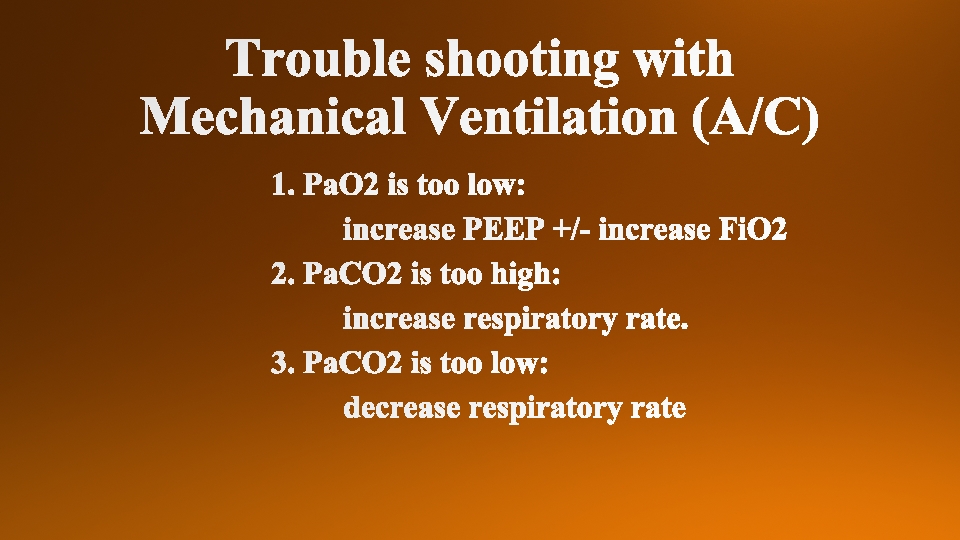
Only FOUR settings you have to consider: 1. Tidal Volume (Vt) = lung protection 2. Respiratory Rate (RR) = ventilation (CO 2) 3. Fi. O 2 = oxygenation 4. PEEP (EPAP) = oxygenation
Vt
Height 5 5’ 1 5’ 2 5’ 3 5’ 4 5'5 5’ 6 5’ 7” 5’ 8” 5’ 9” 5’ 10” 5’ 11” 6’ 6’ 1” 6’ 2” 6’ 3” 6’ 4” Male Kg 52 53 55 57 59 61 63 65 66 68 70 72 74 76 78 79 81 Female Kg 49 50 52 54 55 57 59 60 62 64 65 67 68 70 72 75 77
RR
Fi 02, PEEP
Only FOUR settings you have to consider: 1. Tidal Volume (Vt) = lung protection 2. Respiratory Rate (RR) = ventilation (CO 2) 3 & 4. Fi. O 2/PEEP = oxygenation (the most important setting)
APE, Pneumonia, OD, … everything except Asthma/COPD O 2 +/- Mechanical Ventilation CO 2 Mode: A/C Volume Vt 6 -8 cc/kg IBW RR 18 bpm PEEP 5 cm/Fi. O 2 100% After 5 min, do ABG, follow ARDSnet chart Goal: Pa. O 2 55 -80 or Sa. O 2 90% Asthma/COPD CO 2 +/- O 2 Mode: A/C Volume Vt 8 cc/kg IBW RR 10 bpm PEEP O-4 cm Fi. O 40% Goal: keep p. H above 7. 1
Only FOUR settings you have to consider: 1. Tidal Volume (Vt) = lung protection - 6 -8 cc/kg IBW 2. Respiratory Rate (RR) = ventilation - 18 3 & 4. Fi. O 2/PEEP = oxygenation - 100% and 5
Vt
Vt
RR
Fi 02/PEEP
Fi. O 2 0. 3 0. 4 0. 5 0. 6 0. 7 0. 8 0. 9 1. 0 PEEP 5 5 8 10 10 10 12 14 14 14 16 18 18 -24 8
Fi. O 2 0. 3 0. 4 0. 5 0. 6 0. 7 0. 8 0. 9 1. 0 PEEP 5 5 8 10 10 10 12 14 14 14 16 18 18 -24 8 So you have now set things to Fi. O 2 of 40% (. 4) and a PEEP of 5. If the Sp. O 2 is say 75, then you move one step up to Fi. O 2 0. 4 and PEEP of 8. Then after a minute or so check the Sp. O 2. You keep going up by steps until you get to your goal of Sp. O 2 90 +/-
= Auto PEEP
The END!