Non Communicable Diseases NCDs Introduction introduction Today chronic
 Introduction")
Non Communicable Diseases (NCDs) Introduction
 represent a leading threat to human health")
introduction � Today, chronic non-communicable diseases (NCDs) represent a leading threat to human health and development. � They include: cardiovascular diseases, cancers, type 2 diabetes and chronic respiratory diseases (such as chronic obstructive pulmonary disease and asthma). � Globally these four diseases are the leading cause of death globally

introduction �NCDs kill 40 million people each year, equivalent to 70% of all deaths globally. �Almost three quarters of all NCD deaths, and 82% of the 16 million people who died prematurely (between the ages of 30 and 69 years ), or before reaching 70 years of age, occur in low- and middleincome countries.

introduction � Cardiovascular diseases account for most NCD deaths, or 17. 9 million people annually, followed by cancers (9. 0 million), respiratory diseases (3. 9 million), and diabetes (1. 6 million). � These 4 groups of diseases account for over 80% of all premature NCD deaths. � Tobacco use, physical inactivity, the harmful use of alcohol and unhealthy diets all increase the risk of dying from a NCD.
, also known as chronic diseases, tend to be of")
introduction � Noncommunicable diseases (NCDs), also known as chronic diseases, tend to be of long duration and are the result of a combination of ◦ genetic, ◦ physiological, ◦ environmental and ◦ behaviour factors.

introduction �NCDs disproportionately affect people in low- and middle-income countries where more than three quarters of global NCD deaths – 32 million – occur.

introduction � Regional estimates indicate that chronic diseases are more frequent causes of death than communicable diseases worldwide, with the exception of the African region. � Injuries – accounting for almost one in ten deaths – feature prominently in all regions, caused mostly by traffic crashes, occupational injuries and interpersonal violence. The burden of injuries is increasing in most lowand middle-income countries.

introduction � Mental health problems are leading contributors to the burden of disease in many countries and contribute significantly to the incidence and severity of many chronic diseases, including cardiovascular diseases and cancer. � Visual impairment and blindness, hearing impairment and deafness, oral diseases and genetic disorders are other chronic conditions that account for a substantial portion of the global burden of disease.

introduction � People of all age groups, regions and countries are affected by NCDs. � These conditions are often associated with older age groups, but evidence shows that 15 million of all deaths attributed to NCDs occur between the ages of 30 and 69 years. � Children, adults and the elderly are all vulnerable to the risk factors contributing to NCDs, whether from unhealthy diets, physical inactivity, exposure to tobacco smoke or the harmful use of alcohol.

introduction � These diseases are driven by forces that include ◦ rapid unplanned urbanization, ◦ globalization of unhealthy lifestyles ◦ and population ageing. � Unhealthy diets and a lack of physical activity may show up in people as raised blood pressure, increased blood glucose, elevated blood lipids and obesity. � These are called metabolic risk factors that can lead to cardiovascular disease, the leading NCD in terms of premature deaths.

introduction � Risk factors � Modifiable behavioural risk factors � Modifiable behaviours, such as ◦ ◦ tobacco use, physical inactivity, unhealthy diet and the harmful use of alcohol, all increase the risk of NCDs.

introduction � Risk factors � Modifiable behavioural risk factors � Tobaccounts for 7. 2 million deaths every year (including from the effects of exposure to second-hand smoke), and is projected to increase markedly over the coming years. � 4. 1 million annual deaths have been attributed to excess salt/sodium intake. � More than half of the 3. 3 million annual deaths attributable to alcohol use are from NCDs, including cancer. � 1. 6 million deaths annually can be attributed to insufficient physical activity.

introduction � Risk factors � Metabolic risk factors contribute to four key metabolic changes that increase the risk of NCDs: ◦ ◦ raised blood pressure overweight/obesity hyperglycemia (high blood glucose levels) and hyperlipidemia (high levels of fat in the blood). � In terms of attributable deaths, the leading metabolic risk factor globally is elevated blood pressure (to which 19% of global deaths are attributed), followed by overweight and obesity and raised blood glucose.

introduction � The socioeconomic impacts of NCDs � Poverty is closely linked with NCDs. The rapid rise in NCDs is predicted to impede poverty reduction initiatives in low-income countries, particularly by increasing household costs associated with health care. � Vulnerable and socially disadvantaged people get sicker and die sooner than people of higher social positions, especially because they are at greater risk of ◦ being exposed to harmful products, such as tobacco, or ◦ unhealthy dietary practices, and ◦ have limited access to health services.

introduction � The socioeconomic impacts of NCDs � In low-resource settings, health-care costs for NCDs quickly drain household resources. � The exorbitant (excessive) costs of NCDs, including often ◦ lengthy and expensive treatment and ◦ loss of breadwinners, force millions of people into poverty annually and stifle (suffocate) development.

introduction � Without greater attention to prevention, it has been estimated that by 2030 myocardial infarct, stroke and diabetes will account for four in ten deaths among adults (35– 64 years) in low- and middle-income countries, compared with one in eight deaths in the same age group in the United States of America and other high-income countries.

introduction � Projections suggest that over the next 10 years deaths due to chronic noncommunicable diseases will increase by 17%. � However, large-scale prevention is feasible, as ◦ the causes of the major chronic diseases are known and ◦ are the same in all regions and population subgroups.

introduction �These diseases are preventable. �A small number of modifiable risk factors explain most new cases, � and evidence-based interventions ◦ are available, ◦ cost-effective and ◦ widely applicable.

introduction �Up to 80% of heart diseases, stroke, and type 2 diabetes and over a third of cancers could be prevented by eliminating shared risk factors, ◦ mainly tobacco use, ◦ unhealthy diet, ◦ physical inactivity and ◦ the harmful use of alcohol

introduction Recent trends in death rates � The respective contributions of chronic and infectious conditions to total mortality has changed in the last century. For example, in Brazil infectious diseases accounted for 45% of all deaths in 1930, but only 5% in 2003. � In contrast, the proportion attributed to cardiovascular diseases increased from 12% in 1930 to 31% in 2003. � However, mortality rates are influenced over time by the changing age structure of the population, as well as by waxing and waning epidemics. � The changes in mortality rates in high-income countries have been particularly dramatic in the youngest age groups, where infectious diseases used to account for most mortality. Traffic crashes are now the leading cause of death in childhood in many high-income countries. �

introduction � � � � Recent trends in death rates In the last decades of the twentieth century, the declines in death rates from cardiovascular disease have accelerated in highincome countries. Since the 1970 s, death rates from heart disease and stroke have fallen by up to 70% in Australia, Canada, Japan, the United Kingdom and the United States of America. There have also been improvements in cardiovascular mortality rates in middle-income countries, such as Poland. These gains have been the result of a wide range of measures directed at both whole populations and individuals. The preventive potential for chronic diseases is enormous. A decline in death rates of an additional 2% per annum over 10 years has the potential to avert the untimely deaths of 35 million people.

introduction � Preventive potential � The changing patterns of mortality and morbidity indicate that major causes of disease are preventable. � Yet even the healthiest person will succumb at some age, and the lifetime mortality risk for any population is 100%. � However, most populations are affected by specific diseases which can be prevented. � Studies of migrants show that they often develop the patterns of disease of host populations. For example, the rates of gastric cancer in people born in Hawaii to Japanese parents are lower than those of people born in Japan. After two generations in the USA, people of Japanese heritage have the same gastric cancer rate as the US population in general.

introduction � Preventive �The potential fact that it takes a generation or more for the rates to fall suggests the importance of an exposure – such as diet – in early life. � Geographical variation in disease occurrence within and between countries also provides important clues to preventive potential.

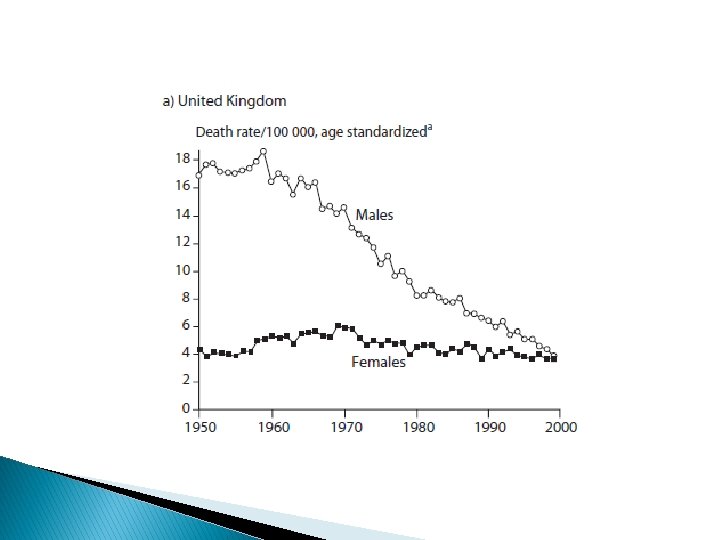
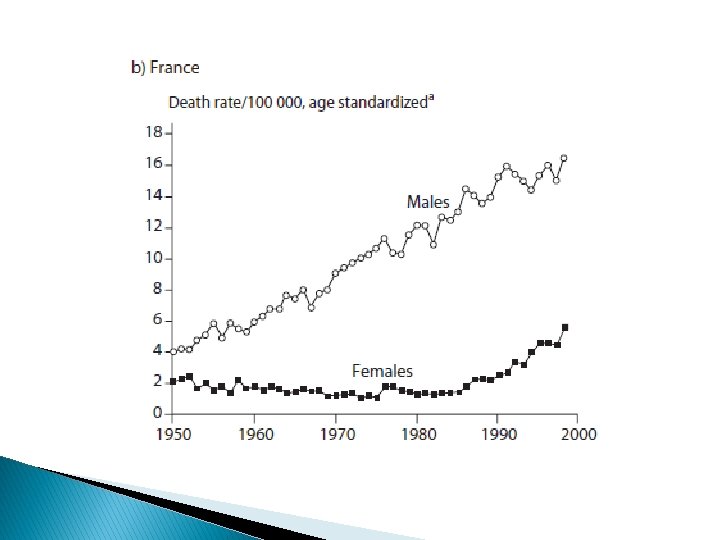
introduction � Preventive potential � In the United Kingdom age-standardized male lung cancer rates fell from 18 per 100 000 in 1950 to 4 per 100 000 by 2000. � In contrast, over the same period of time in France, male lung cancer rates increased. � In France, the increase in tobacco use occurred some decades later than in the United Kingdom, and smoking rates started to decrease only after 1990. Similarly, global lung cancer rates in women continue to rise, but this increase has been avoided in the United Kingdom.

Prevention and control of NCDs � An important way to control NCDs is to focus on reducing the risk factors associated with these diseases. � Low-cost solutions exist for governments and other stakeholders to reduce the common modifiable risk factors. � Monitoring progress and trends of NCDs and their risk is important for guiding policy and priorities.

Prevention and control of NCDs � To lessen the impact of NCDs on individuals and society, a comprehensive approach is needed requiring all sectors, including health, finance, transport, education, agriculture, planning and others, to collaborate to reduce the risks associated with NCDs, and promote interventions to prevent and control them.

Prevention and control of NCDs � Investing in better management of NCDs is critical. � Management of NCDs includes detecting, screening and treating these diseases, and providing access to palliative care for people in need. � High impact essential NCD interventions can be delivered through a primary health care approach to strengthen early detection and timely treatment. � Evidence shows such interventions are excellent economic investments because, if provided early to patients, they can reduce the need for more expensive treatment.

Prevention and control of NCDs � Countries with inadequate health insurance coverage are unlikely to provide universal access to essential NCD interventions. � NCD management interventions are essential for achieving the global target of a 25% relative reduction in the risk of premature mortality from NCDs by 2025, and the SDG target of a one-third reduction in premature deaths from NCDs by 2030.

International Efforts � Political Declaration of the High-level Meeting of the General Assembly on the Prevention and Control of Non-communicable Diseases � United Nations on 19 and 20 September 2011 � http: //www. who. int/nmh/events/un_ncd_summit 201 1/political_declaration_en. pdf

GLOBAL ACTION PLANFOR THE PREVENTION AND CONTROL OF NONCOMMUNICABLE DISEASES 2013 - 2020 � VISION: � A world free of the avoidable burden of noncommunicable diseases. � GOAL: � To reduce the preventable and avoidable burden of morbidity, mortality and disability due to noncommunicable diseases by means of multisectoral collaboration and cooperation at national, regional and global levels, so that populations reach the highest attainable standards of health and productivity at every age and those diseases are no longer a barrier to well-being or socioeconomic development � http: //apps. who. int/iris/bitstream/10665/94384/1/9789241506236_eng. pdf? ua=1

GLOBAL ACTION PLANFOR THE PREVENTION AND CONTROL OF NONCOMMUNICABLE DISEASES 2013 - 2020 � � � � � OVERARCHING PRINCIPLES: >> Life-course approach >> Empowerment of people and communities >> Evidence-based strategies >> Universal health coverage >> Management of real, perceived or potential conflicts of interest >> Human rights approach >> Equity-based approach >> National action and international cooperation and solidarity >> Multisectoral action

GLOBAL ACTION PLANFOR THE PREVENTION AND CONTROL OF NONCOMMUNICABLE DISEASES 2013 - 2020 � � OBJECTIVES To raise the priority accorded to the prevention and control of noncommunicable diseases in global, regional and national agendas and internationally agreed development goals, through strengthened international cooperation and advocacy. To strengthen national capacity, leadership, governance, multisectoral action and partnerships to accelerate country response for the prevention and control of noncommunicable diseases. To reduce modifiable risk factors for noncommunicable diseases and underlying social determinants through creation of health-promoting environments.

GLOBAL ACTION PLANFOR THE PREVENTION AND CONTROL OF NONCOMMUNICABLE DISEASES 2013 - 2020 � � OBJECTIVES To strengthen and orient health systems to address the prevention and control of noncommunicable diseases and the underlying social determinants through people-centred primary health care and universal health coverage. To promote and support national capacity for high-quality research and development for the prevention and control of noncommunicable diseases. To monitor the trends and determinants of noncommunicable diseases and evaluate progress in their prevention and control

GLOBAL ACTION PLANFOR THE PREVENTION AND CONTROL OF NONCOMMUNICABLE DISEASES 2013 - 2020 � � � VOLUNTARY GLOBAL TARGETS A 25% relative reduction in risk of premature mortality from cardiovascular diseases, cancer, diabetes, or chronic respiratory diseases. At least 10% relative reduction in the harmful use of alcohol, as appropriate, within the national context. A 10% relative reduction in prevalence of insufficient physical activity. A 30% relative reduction in mean population intake of salt/sodium. A 30% relative reduction in prevalence of current tobacco use in persons aged 15+ years.

GLOBAL ACTION PLANFOR THE PREVENTION AND CONTROL OF NONCOMMUNICABLE DISEASES 2013 - 2020 � � � VOLUNTARY GLOBAL TARGETS A 25% relative reduction in the prevalence of raised blood pressure or contain the prevalence of raised blood pressure, according to national circumstances. Halt the rise in diabetes and obesity. At least 50% of eligible people receive drug therapy and counselling (including glycaemic control) to prevent heart attacks and strokes. An 80% availability of the affordable basic technologies and essential medicines, including generics, required to treat major noncommunicable diseases in both public and private facilities.

https: //public. tableau. com/profile/willistowerswatson#!/vizhome/ Global. Burdenof. Non-communicable. Disease/GBD 2015_1 http: //gamapserver. who. int/gho/interactive_charts/ncd/mortality /total/atlas. html https: //www. who. int/ncds/surveillance/steps/riskfactor/en/ http: //apps. who. int/nmh/ncd-map-toolkit/developing/tooltemplate. html#ch_1 https: //ncdalliance. org/global-ncda-forum-2020 https: //apps. who. int/iris/bitstream/handle/10665/94384/97892 41506236_eng. pdf? sequence=1

SUSTAINABLE DEVELOPMENT GOAL 3 Ensure healthy lives and promote well-being for all at all ages https: //sustainabledevelopment. un. org/sdg 3

SUSTAINABLE DEVELOPMENT GOAL 3 �TARGET 3. 4 �By 2030, reduce by one third premature mortality from non-communicable diseases through prevention and treatment and promote mental health and well-being

SUSTAINABLE DEVELOPMENT GOAL 3 �INDICATORS � 3. 4. 1 �Mortality rate attributed to cardiovascular disease, cancer, diabetes or chronic respiratory disease � 3. 4. 2 �Suicide mortality rate

PROGRESS OF GOAL 3 IN 2017 � Non-communicable diseases and mental health � Premature deaths (before 70 years of age) owing to cardiovascular disease, cancer, chronic respiratory disease or diabetes totalled about 13 million in 2015, accounting for 43 per cent of all premature deaths globally. � From 2000 to 2015, the risk of dying between 30 and 70 years of age from one of those four causes decreased from 23 per cent to 19 per cent, falling short of the rate required to meet the 2030 target of a one-third reduction.

PROGRESS OF GOAL 3 IN 2017 Non-communicable diseases and mental health � Tobacco and alcohol use contributes to the burden of noncommunicable diseases. � The World Health Organization (WHO) Framework Convention on Tobacco Control has been ratified by 180 parties, which represent 90 per cent of the global population. � Still, more than 1. 1 billion people, mostly men, consumed tobacco in 2015. � The prevalence of smoking among those individuals 15 years of age and older dropped from 23 per cent in 2007 to 21 per cent in 2013. � In 2016, the average consumption of pure alcohol was 6. 4 litres per year person among those individuals 15 years of age or older. �

PROGRESS OF GOAL 3 IN 2017 � Non-communicable diseases and mental health � Indoor and ambient air pollution is the greatest environmental health risk. � Globally in 2012, household air pollution from cooking with unclean fuels or inefficient technologies led to an estimated 4. 3 million deaths, while ambient air pollution from traffic, industrial sources, waste burning or residential fuel combustion resulted in an estimated 3 million deaths.

From Burden to “Best Buys”: Reducing the Economic Impact of Non. Communicable Diseases in Low- and Middle-Income Countries https: //www. who. int/nmh/publications/best_buys_summary. pdf
 � � � � �")
STEPwise approach to noncommunicable disease risk factor surveillance (STEPS) � � � � � Introduction The STEPS approach focuses on obtaining core data on the established risk factors that determine the major disease burden. It is sufficiently flexible to allow each country to expand on the core variables and risk factors, and to incorporate optional modules related to local or regional interests. Purpose The WHO STEPwise approach to noncommunicable disease (NCD) risk factor surveillance is designed to help countries build and strengthen their surveillance capacity. Design The STEPS Instrument covers three different levels of "steps" of risk factor assessment. These steps are: Questionnaire Physical measurements Biochemical measurements

STEPwise approach to surveillance � STEPS conceptual framework � The STEPS approach focuses on obtaining core data, at each level, on the established risk factors that determine the major disease burden. � It is sufficiently flexible to allow each country to expand on the core variables and risk factors, and to incorporate optional modules related to local or regional interests.

STEPwise approach to surveillance � � � Step 1 - Questionnaire-based assessment The STEPS approach has three levels and within each level, risk factor assessment is divided into core, expanded, and optional modules. Step 1 contains as the core or “minimum set”, selfreport measures that all countries should obtain. In addition to socio-economic data, data on tobacco and alcohol use, some measure of nutritional status and physical inactivity are included as markers of current and future health status. Standard WHO definitions for measuring the prevalence of tobacco use and alcohol consumption and internationally derived measures of physical activity are recommended. The information can be used not only for within-country trends, but also for comparisons across countries. The questionnaires used in the core data set are simple and few in number and are not intended to give a complete picture of each behaviour but rather to provide information on the population distribution of risk.

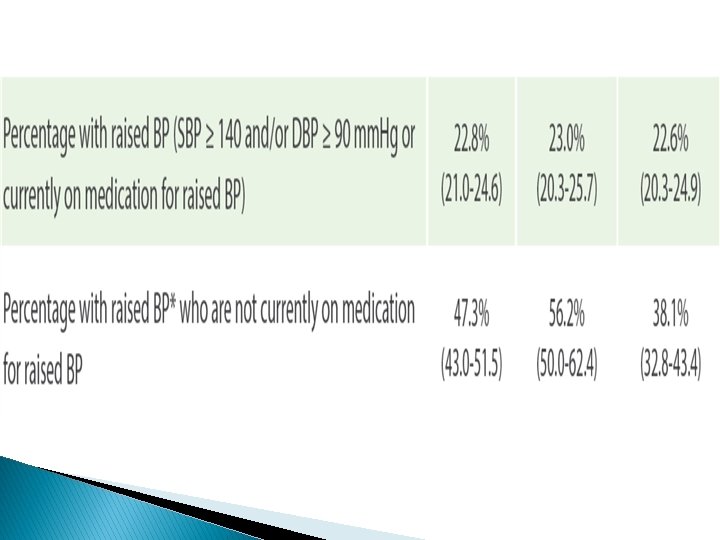
STEPwise approach to surveillance � Step 2 - Simple physical measurements � Step 2 adds to Step 1 by the inclusion of simple physical measurements, such as height, waist circumference, and blood pressure. Step 1 and Step 2 are desirable and appropriate for most developing countries.

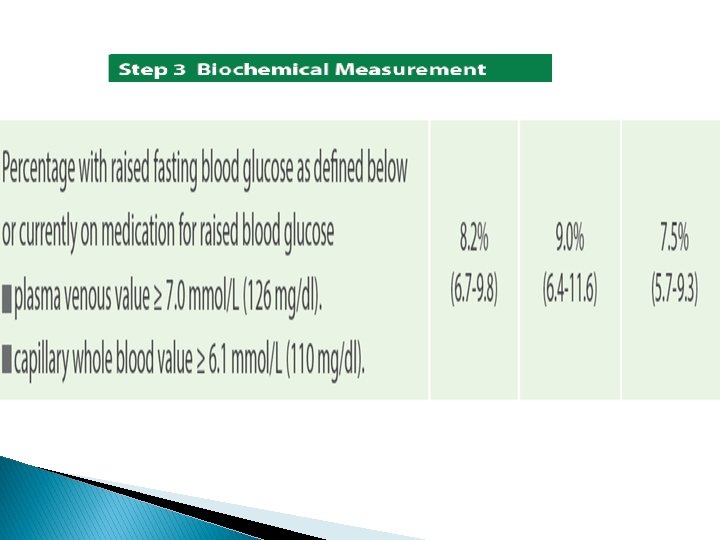
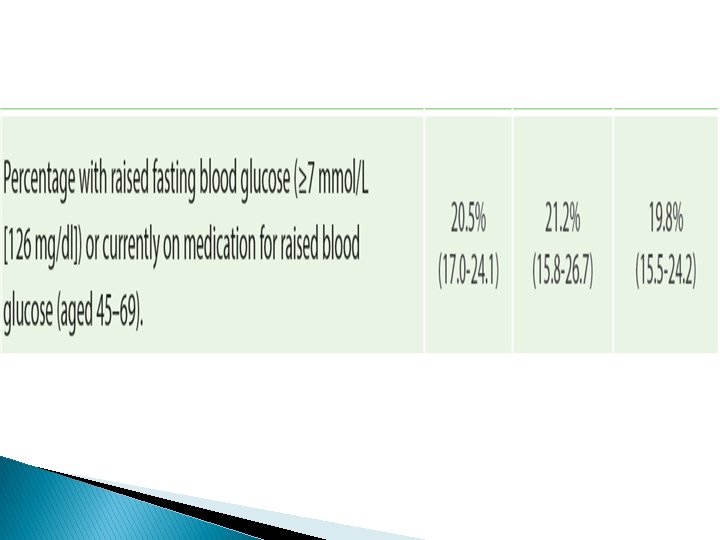
STEPwise approach to surveillance � Step 3 - Biochemical Measurements � Step 3 includes Steps 1 and 2 and adds biochemical measurements. All the core items from Steps 1 and 2 can be readily assessed and are not made more complex if the expanded items are added. However, additional information at Step 3 is of a biochemical nature and requires access to the appropriate standardized laboratories. Collecting and analysing blood samples is a relatively complex process and can be done only in the context of a comprehensive survey and in settings where appropriate resources are available. The addition of Step 3 can increase the cost and complexity of data collection.

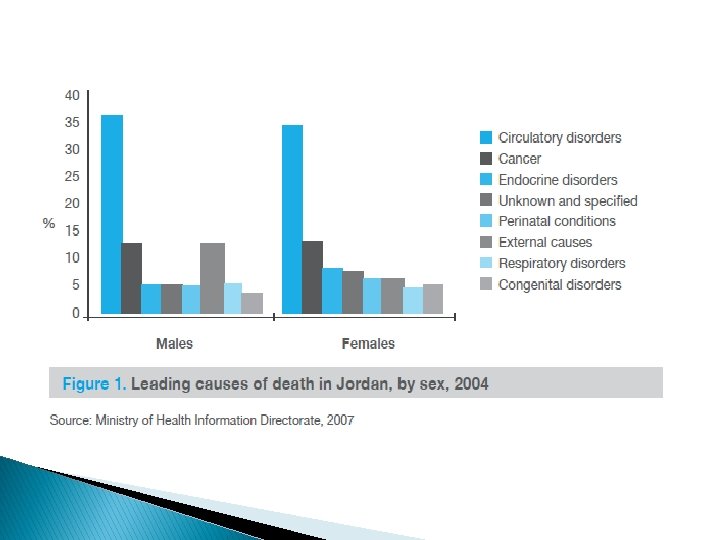
NCDs in Jordan � Mortality levels and trend analysis indicate that cardiovascular diseases are the main cause of death, accounting for 38% of all deaths in 2004. � Cancer ranks second (14%) and � External causes including injuries (11%) ranks third.
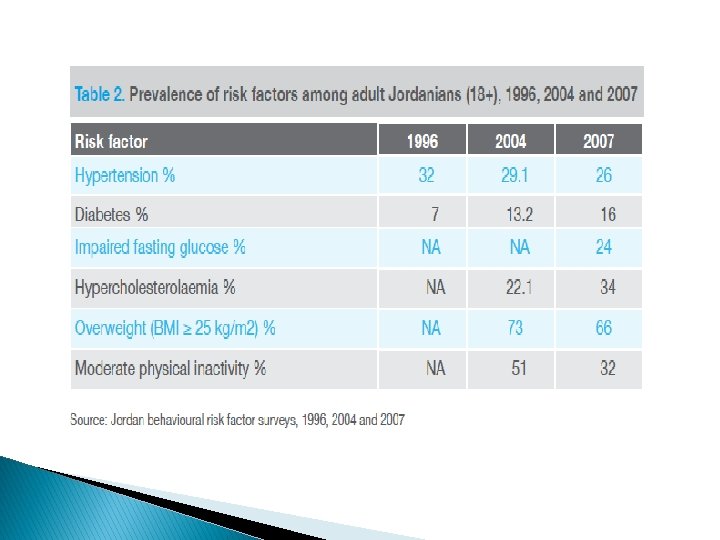

NCDs in Jordan � Chronic and noncommunicable diseases, lifestyle and behavioural risk factors � Jordan is witnessing an increasing trend in the number and severity of noncommunicable diseases, particularly cardiovascular diseases, cancer, diabetes and chronic respiratory conditions. � The major cardiovascular diseases prevalent in Jordan are hypertension, coronary heart disease and stroke. � There is an increasing prevalence of risk factors when compared to 2004 data.

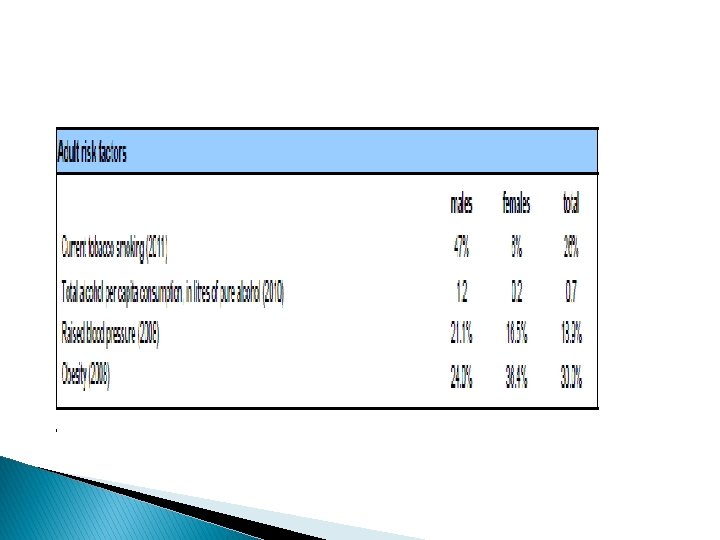
NCDs in Jordan � Chronic and noncommunicable diseases, lifestyle and behavioural risk factors � A 2007 survey conducted among adult Jordanians 18 years or older found ◦ the prevalence of hypertension to be 26% (31% in males, 22% in females), ◦ diabetes 16%, impaired fasting glucose 24% (50% increase from 2005) and ◦ hypercholesterolaemia 34%.

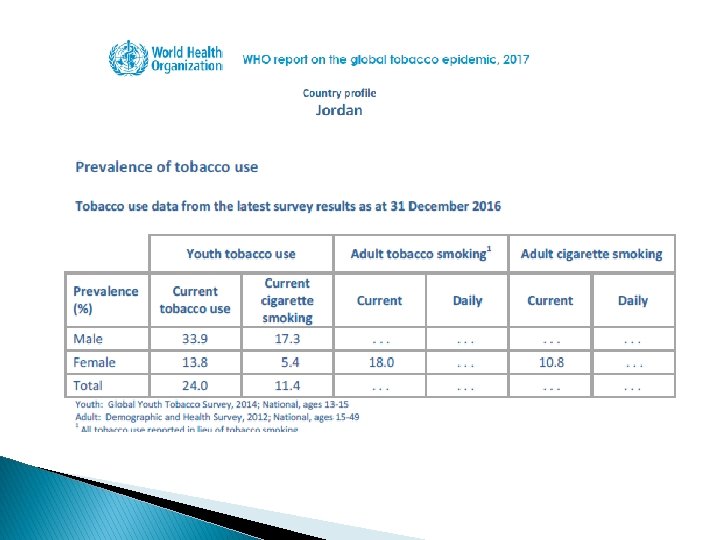
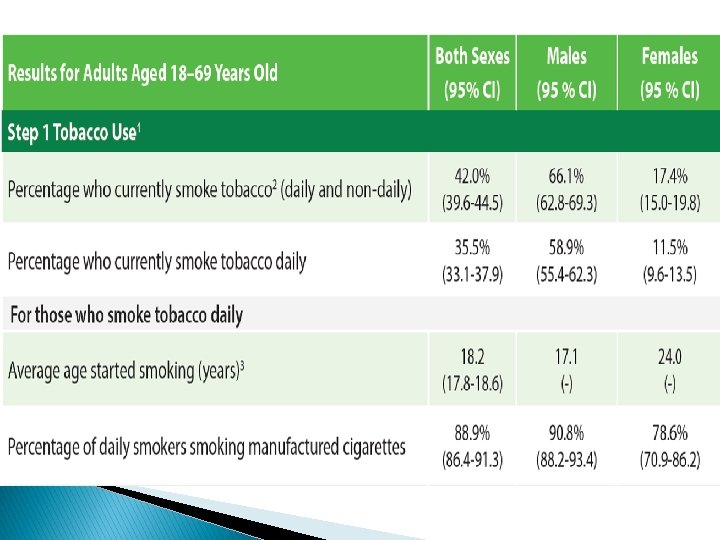
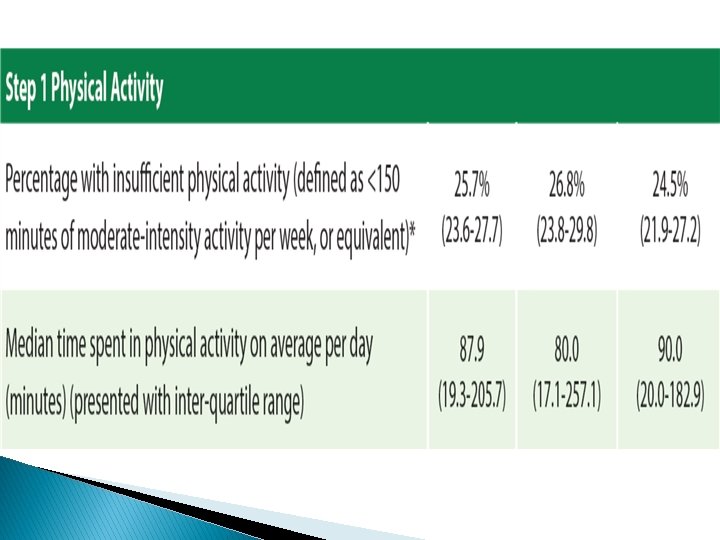
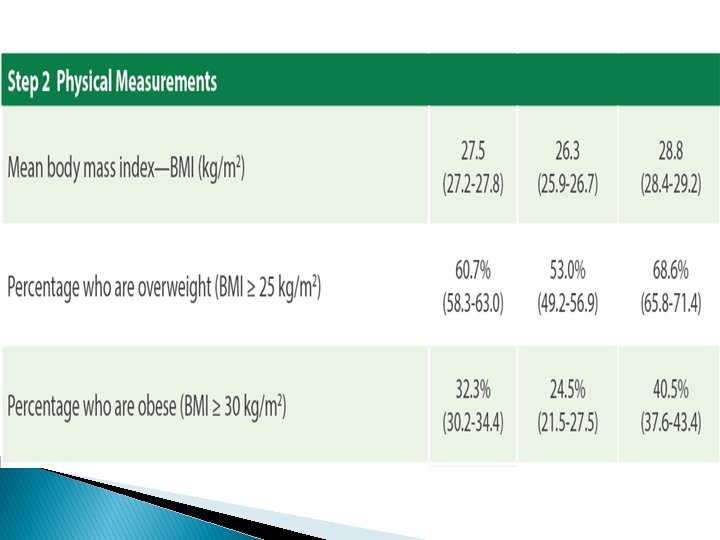
NCDs in Jordan � Chronic and noncommunicable diseases, lifestyle and behavioural risk factors � The prevalence of overweight (BMI ≥ 25 kg/m 2) was 66% (63% in males, 70% among females). � Levels of physical inactivity are high and estimates show moderate inactivity at 32% (improved from 50% in 2005). � Almost 29% of the Jordanians smoke cigarettes regularly (50% males, 6% females) and another 9% smoke waterpipe. � About 60% of smokers started smoking before the age of 18.

NCDs in Jordan � Chronic and noncommunicable diseases, lifestyle and behavioural risk factors � Based on FAO statistics, the average daily per capita dietary energy supply increased by 25% during the period 1962– 2002, with the carbohydrate share of the dietary energy supply decreasing (though it remains high, at 62%). � The decrease was accompanied by an increase in the share of energy supply from fat. � The protein share remained relatively stable, fluctuating around 10%. � This increasing share of fat may contribute to the epidemiological shift towards noncommunicable diseases.

NCDs in Jordan Chronic and noncommunicable diseases, lifestyle and behavioural risk factors � The National Cancer Registry was established in 1996. � The crude incidence rate for all cancers among Jordanians in 2004 was 67. 1 per 100 000 population (63. 9 for males and 70. 5 for females). � However, when rates are adjusted to the world standard population, gender differences disappear (agestandardized rates per 100 000: males 112. 5 and females 112. 6). � Breast cancer ranked first among females, accounting for 32. 9% of all female cancers, while colorectal cancer was the commonest among males, 14. 1% of all male cancers. � The majority of cancer cases are diagnosed in late stages of the disease. �

NCDs in Jordan � The main challenges of health sector in Jordan fall within the following two clusters: � health system (governance, financing, human resources, evidence and research); � and epidemiological transition (chronic and noncommunicable diseases, lifestyle and behavioural risk factors).
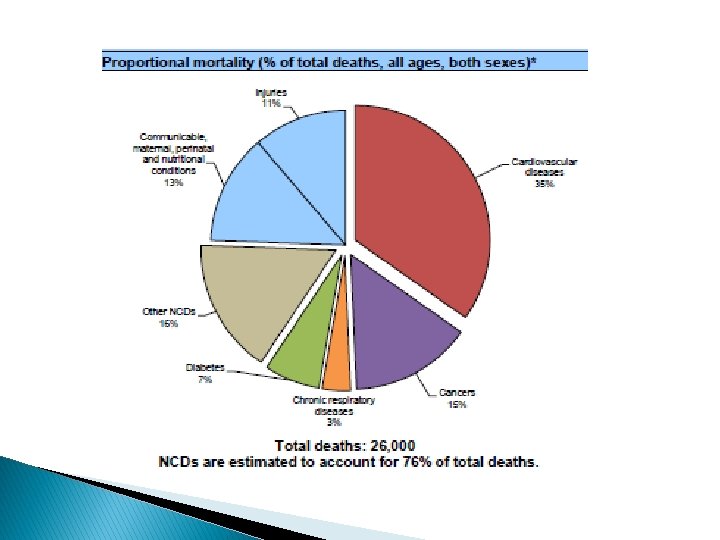
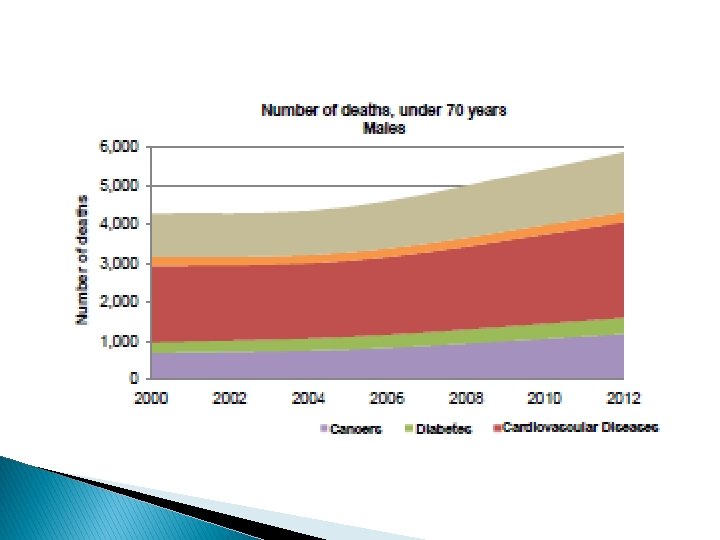
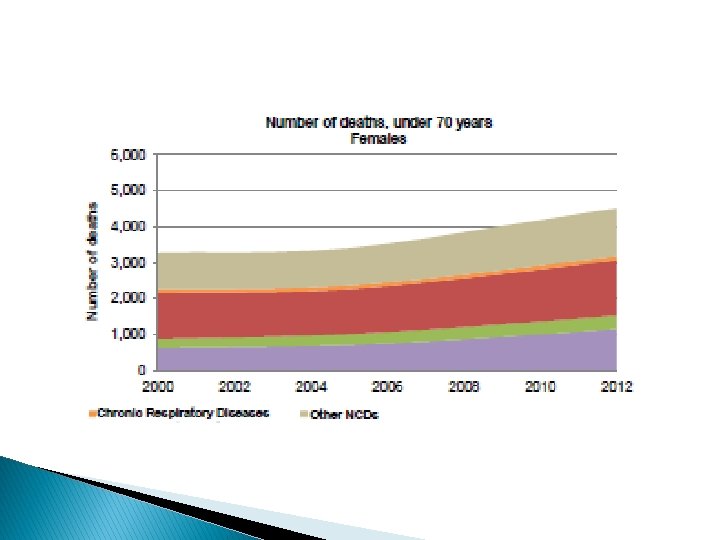

NCDs in Jordan � There were 29, 855 deaths in Jordan in 2016. � Of these deaths, an estimated 22, 690 (76%) were caused by NCDs. � By 2025, this number will rise to an estimated 29, 487 deaths caused by the top four noncommunicable diseases in Jordan: cardiovascular disease, cancer, chronic respiratory diseases, and diabetes. � In fact, the probability of dying between the ages of 30 and 70 of an NCD in Jordan is 20%.

https: //www. who. int/nmh/countries/2018/jor_en. pdf? ua=1

https: //www. who. int/nmh/countries/2018/jor_en. pdf? ua=1

� � http: //applications. emro. who. int/docs/CCS_Jordan_2010_EN_14473. pdf? ua=1 http: //www. moh. gov. jo/Echo. Bus. V 3. 0/System. Assets/PDFs%20 AR/Strategies_AR/% D 8%A 7%D 9%84%D 8%A 7%D 8%B 3%D 8%AA%D 8%B 1%D 8%A 7%D 8%AA%D 9%8 A%D 8%AC%D 9%8 A%D 8%A 9%20%D 8%A 7%D 9%84%D 9%88%D 8%B 7%D 9%86%D 9%8 A%D 8%A 9%20%D 9%84%D 9%88%D 9%82%D 8%A 7%D 9%8 A%D 8%A 9%20%D 9%85%D 9%86%20%D 8%A 7%D 9%84% D 8%A 7%D 9%85%D 8%B 1%D 8%A 7%D 8%B 6%20%D 8%BA%D 9%8 A%D 8%B 1%20%D 8%A 7%D 9%84 %D 8%B 3%D 8%A 7%D 8%B 1%D 9%8 A%D 8%A 9. pdf



Recommendations � The surge in NCDs risk factors reported in the STEPS 2019, explains the high prevalence of NCDs that Jordan is experiencing. � This requires a prompt and effective response that adopts a multi-sectoral approach to convene efforts of all relevant stakeholders to curb NCDs and their risk factors. � Primarily, strict measures to combat ◦ ◦ ◦ tobacco consumption, dietary salt, physical inactivity, obesity, hypertension, and diabetes.
 � � People living with or affected by the")
COVID-19 and NCDs (WHO 2020) � � People living with or affected by the major (NCDs) appear to be more vulnerable to becoming severely ill with the virus. In particular, they will be put at a higher risk of the consequences of bilateral viral pneumonia. Risk factors for NCDs can make people more vulnerable to becoming severely ill with COVID 19. ◦ Smokers are likely to be more vulnerable to COVID-19 as the act of smoking means that fingers (and possibly contaminated cigarettes) are in contact with lips which increases the possibility of transmission of virus from hand to mouth. ◦ Smokers may also already have lung disease or reduced lung capacity which would greatly increase risk of serious illness. ◦ Smoking products such as water pipes often involve the sharing of mouth pieces and hoses, which could facilitate the transmission of COVID-19 in communal and social settings. ◦ https: //www. who. int/teams/noncommunicable-diseases/covid-19
 �Persons with disabilities may be impacted more significantly by")
COVID-19 and NCDs (WHO 2020) �Persons with disabilities may be impacted more significantly by COVID-19. �This impact can be mitigated if simple actions and protective measures are taken. ◦ https: //www. who. int/teams/noncommunicable-diseases/covid-19

COVID-19 and NCDs � The response to this virus requires extraordinary measures may include significant disruption of access to – or even critical shortages of -- medicines for people living with or affected by NCDs. It is imperative to immediately ensure that the supply chains for essential NCD medicines are protected, prioritized and continue to function efficiently, and that these products are distributed on the basis of need and/or equitability. � https: //www. who. int/teams/noncommunicable-diseases/covid-19

COVID-19 and NCDs �Health services will be disrupted in many settings. This will impact the detection and diagnosis of NCDs. Elective procedures and other services for NCDs may be affected or delayed and can lead to consequences. � https: //www. who. int/teams/noncommunicable-diseases/covid-19

COVID-19 and NCDs � To ensure access to care for people living with or affected by NCDs, both for people infected with the virus and people who are not, ◦ governments can reduce access barriers to essential health services for people living with NCDs, and ◦ manage referral systems between primary and other levels of care, so that the most at risk can access life-saving care. � https: //www. who. int/teams/noncommunicable-diseases/covid-19

COVID-19 and NCDs �It is also a critical part of the response to halt the transmission of the virus by ensuring that people living with NCDs and affected by the virus can be detected, isolated and cared for as rapidly as possible. � https: //www. who. int/teams/noncommunicable-diseases/covid-19

COVID-19 and NCDs � Recognizing the interconnectedness of COVID-19 and NCDs, there is an urgent need to coordinate and cooperate on all aspects of the NCD component of the COVID-19 public health response, at the three levels of WHO, including implementation of preparedness and response policies, response financing, management of global supply stockpiles, and data analysis. � There is also a need to align risk communications and good practices to inform communities and counter misinformation. ◦ https: //www. who. int/teams/noncommunicable-diseases/covid-19

COVID-19 and NCDs � Epidemiological investigations, trend analysis and forecasting will be necessary to better understand the relationship between NCDs, their risk factors, and predisposition to the COVID-19 as well as their influence on the course and outcome of the disease, and the broader impact of the pandemic on avoidable mortality and disability for NCDs. Together with reviews of evidence and better knowledge management, these will feed into more a more robust evidence base to inform help understand spread, severity, spectrum of disease, impact on the community, and to inform operational models for implementation of countermeasures and planning for recovery. ◦ https: //www. who. int/teams/noncommunicable-diseases/covid-19

COVID-19 and NCDs � � � The COVID-19 outbreak and response has been accompanied by an “infodemic: ” an overabundance of information — some accurate and some not — that makes it hard for people living with NCDs to find trustworthy sources and reliable guidance when they need it. WHO and partners will coordinate efforts to ensure that recommendations for people living with NCDs are evidence informed and can be applied at the community level and that people affected by NCDs have a voice and are part of the response. It will be necessary to regularly update these recommendations, as gaps in our knowledge are filled. Shared platforms will be build include common repositories for data, knowledge, risk communication, and outcomes and findings, and dissemination strategies will be put in place to enable the sharing of data and information notes. ◦ https: //www. who. int/teams/noncommunicable-diseases/covid-19
- Slides: 90