NO CONFLICT INTEREST Diseases affect basement membrane which

NO CONFLICT INTEREST

Diseases affect basement membrane which leads to nephrotic syndrome= proteinuria

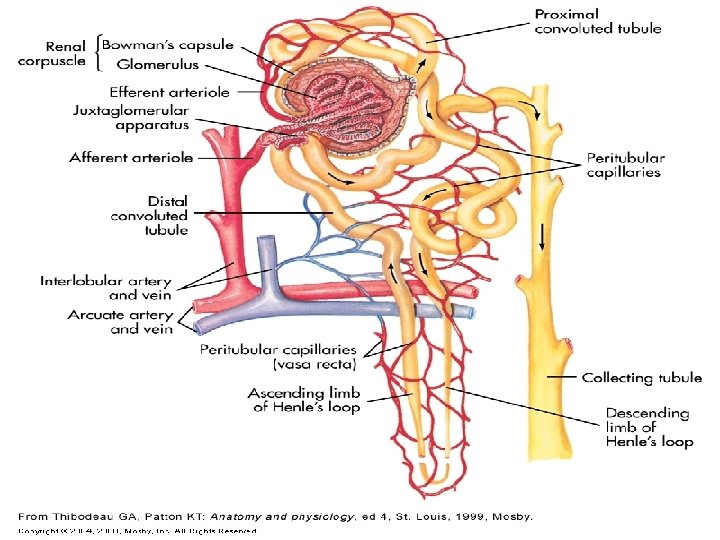
Kidney excretion o Can eliminate large amounts of acid o Can also excrete base o Can conserve and produce bicarb ions o Most effective regulator of p. H o If kidneys fail, p. H balance fails

ACID-BASE REGULATION o Kidney Regulation Excess acid is excreted by the kidneys, largely in the form of ammonia n The kidneys have some ability to alter the amount of acid or base that is excreted, but this generally takes several days n





RENIN… 1. Increasing peripheral vasoconstriction 2. Stimulating Aldosterone secretion Aldosterone promotes the reabsorption of sodium and water to correct the fluid deficit and/or inadequate blood flow (renal ischemia)


ACID-BASE REGULATION o Maintenance of an acceptable p. H range in the extracellular fluids is accomplished by three mechanisms: n 1) Chemical Buffers ¡ React very rapidly (less than a second) n 2) Respiratory Regulation ¡ Reacts rapidly (seconds to minutes) n 3) Renal Regulation ¡ Reacts slowly (minutes to hours)

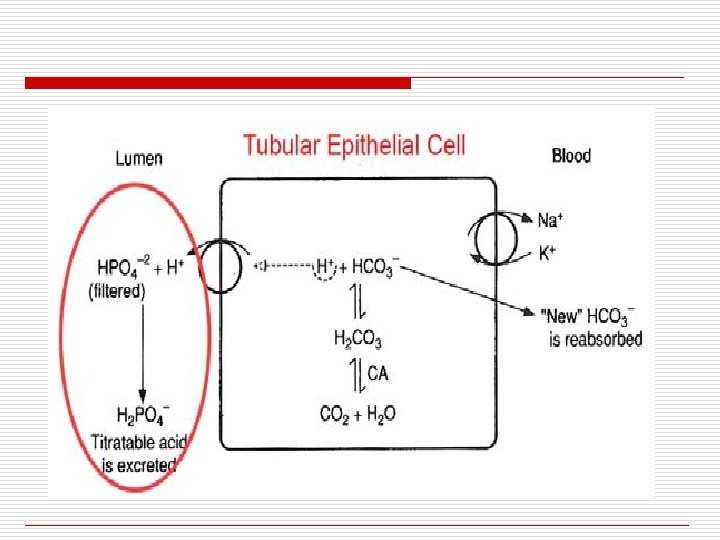


Take Home Message ü The kidney glomerulus passively filters on the order of 4000 mmol of HCO 3 - each day. This has to be reabsorbed. To lose it would be a disaster ü In order to reabsorb this filtered load of HCO 3 -. , the tubular cells must therefore secret 4000 mmol of hydrogen ions ü This allows the conversion of carbonic acid to CO 2 and water, which will passively come back into the proximal tubular cell. The secretion of titratable acid by the kidney, used to actually modify the blood p. H, goes on in the distal tubule
 is produced from the")
AMMONIUM GENERATES HCO 3 - * * Ammonium (NH 4+) is produced from the cellular metabolism of glutamine in all nephron segments. Ammonium is secreted into the lumen, and 2 HCO 3 - ions are formed and reabsorbed **

The anion gap, is really not a gap at all, it just represents the anions we don’t usually measure. a. AG = Na+ - (Cl- + HCO 3 –), typically about 10 to 12 mmol b. The AG represents anions such as proteins, phosphates, sulfates and organic anions. c. Increase in the AG i. Is most often due to increased serum lactate or acetoacetate. ii. Rarely, an increased AG may be due to a decrease in cations such as Ca+2, magnesium and/or K+ d. Decrease in the AG i. Increase in unmeasured cations ii. Addition of something new to the blood such as Li+ iii. Reduction in a major plasma protein such as albumin (renal loss). iv. Hyperlipidemias and other less common causes.


HYPERKALEMIA o Hyperkalemia is generally associated with acidosis n Accompanied by a shift of H+ ions into cells and K+ ions out of the cell to maintain electrical neutrality + H + K

HYPERKALEMIA Hyperkalemia is an elevated serum K+ n H+ ions are buffered in cell by proteins o Acidosis may cause Hyperkalemia and Hyperkalemia may cause Acidosis o + H + K

ELECTROLYTE SHIFTS Acidosis Compensatory Response H+ K+ Result - H+ buffered intracellularly - Hyperkalemia cell Alkalosis Compensatory Response H+ K+ cell Result - Tendency to correct alkalosis - Hypokalemia

ACIDIFICATION OF URINE BY EXCRETION OF AMMONIA


ACIDIFICATION OF URINE BY EXCRETION OF AMMONIA Capillary Distal Tubule Cells NH 2 NH 3 H + WHAT HAPPENS NEXT? Tubular urine to be excreted 29

ACIDIFICATION OF URINE BY EXCRETION OF AMMONIA Capillary Distal Tubule Cells NH 3 Dissociation of carbonic acid -+H H 23 CO HCO 3 Notice the H+-Na+ exchange to maintain electrical neutrality + + Cl. Na. Cl + Na. HCO 3 NH 3 Cl. NH 4 Cl Tubular Urine 30



ACID-BASE BALANCE o Derangements of hydrogen and bicarbonate concentrations in body fluids are common in disease processes 34

ACID-BASE BALANCE o H+ ion has special significance because of the narrow ranges that it must be maintained in order to be compatible with living systems 35

Metabolic effects o Respiratory n n n hyperventilation shift of haemoglobin dissociation curve to the right decreased 2, 3 DPG levels in red cells (shifting the ODC back to the left) Cardiovascular o Others o n n increased bone resorption (chronic acidosis only) shift of K+ out of cells causing hyperkalaemia


- Slides: 38