NITMED TUTORIALS THE WHO PARTOGRAPH PARTOGRAPH NITMED TUTORIALS















 , 2: sutures overlapped but reducible(moderate), 3:")

























 The Graphic Analysis Of Labour. Am. J. Obstetrics and")
- Slides: 45
NITMED TUTORIALS THE WHO PARTOGRAPH
PARTOGRAPH NITMED TUTORIALS
OUTLINE Objectives of the presentation Introduction History of the Partograph Importance of Partograph components and Standard documentation in Partographic monitoring Clinical relevance Controversy Conclusion References.
OBJECTIVES OF THE PRESENTATION To understand the concept of the partograph Proper documentation on the partograph. To understand the first stage of labour. To interpret a recorded partograph and recognise any deviation from normal.
INTRODUCTION A Greek word meaning “labour curve” The partograph is a composite graphical record of key data (maternal and fetal) during the stage of labour entered against time on a single sheet of paper. the key terms include; maternal status, fetal status, and the progress of labour and the first stage of labour is divided into latent and active phase of labour
HISTORY OF THE PARTOGRAPH First graphical documentation-1950 s FRIEDMAN described a normal cervical dilation pattern- latent and active phase- 1954 - Friedman curve -(sigmoid curve) acceleration phase, phase of maximum slope, deceleration phase Hendrick et al-1969 - cervical dilatation rate, refuted deceleration phase Scientific basis for intervention to prevent prolonged labour was confirmed-1970 s Philpot and castle 1970 - built on Friedman’s work.
HISTORY OF THE PARTOGRAPH WHO model as international standards in 1988. A multicenter trial involving more than 35000 women in Indonesia, Malaysia and Thailand-outcomes of labour are better with partograph , leading to WHO recommendation for all labour. WHO partograph in 1994 - included the latent phase of 8 hrs the issues of latent phase with management. modified WHO partograph- 2000 - no latent phase
IMPORTANCE OF PARTOGRAPH It is a graphical representation of labour progress and the condition of mother and fetus Guides in early detection of prolonged labour and obstructed labour. Informs decision making in the management of labour. It is a universal consensus on reporting labour events. Useful and relevant in any part of the world. It aids in proper handing over of paturient from one caregiver to the other. It is a legal document.
THE PRINCIPLES OF THE PARTOGRAPH The active phase of the labour commences at 3 cm for primigravida and 4 cm for multigravida. The latent phase should not last longer than 8 hrs During the active phase, the rate of cervical dilatation should not be slower than 1 cm/hour
THE PRINCIPLES OF THE PARTOGRAPH A lag time of 4 hours between the slowing of labour and the need for intervention unlikely to compromise the fetusormother and avoid unnecessary intervention. Vaginal examination should be performed as infrequently as is compatible with safe practice. Midwifes and other personnel may have difficulty in constructing alert and action lines and it is better to use partograph with preset line
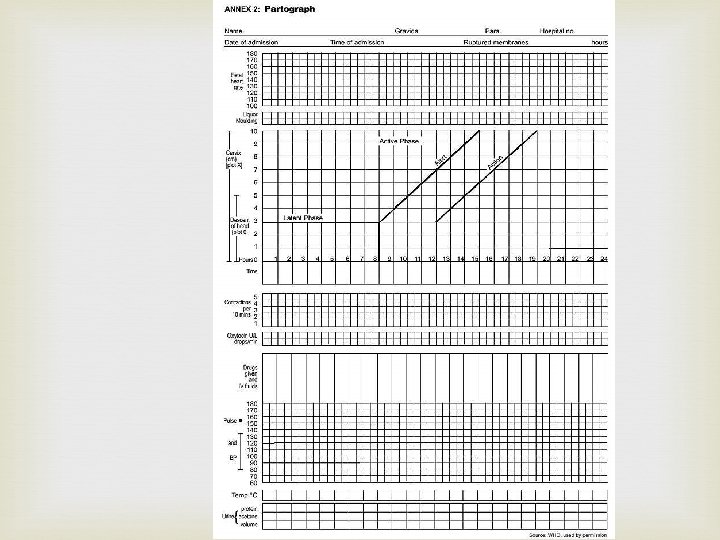
DESCRIPTION OF THE PARTOGRAPH It consists of: Biodata Fetal condition Progress of labour Maternal condition
BIODATA Name of patient Gravidarity/parity Hospital number Date and time of admission Time of ruptured of membrane
FETAL CONDITION This part of the graph is used to monitor and assess fetal condition 1 - Fetal heart rate 2 - Membranes and liquor 3 - Molding the fetal skull bones. Caput
FETAL CONDITION Fetal heart rate and pattern; record every half hour. usually done with a dot and linked by a line.
FETAL CONDITION Amniotic fluid colour; labelled with ICMB. I - intact membrane, C- membrane, M- meconium stained liquor, B- blood stained liquor
FETAL CONDITION Moulding; 1: sutures apposed (mild) , 2: sutures overlapped but reducible(moderate), 3: sutures overlapped and not reducible(severe)
PROGRESS OF LABOUR Cervical dilatation Descent of the fetal head Uterine contractions This section of the partograph has, as its central feature, a graph of cervical dilation against time
PROGRESS OF LABOUR. Cervicograph; a plot of cervical dilatation against the hours and time in labour starting from the onset of active phase there are two distinct lines on the graph- the alert and the action lines. the alert line starts from the 4 cm mark and ascend at the rate of lcm/hour. The action runs parallel to this line but at a 4 cm distance to the right. Recordings are first made with the mark of a cross(x) and subsequently linked by a linear line. Begin plotting from the 4 cm
PROGRESS OF LABOUR Descent- part of the fetal head palpable above the pubis symphysis , measured in number of fifth. recorded as a circle(o). this is done at every vaginal examination.
PROGRESS OF LABOUR Contractions: Chart every half hour; palpate the number of contractions in 10 minutes and their duration in seconds Less than 20 seconds: Between 20 and 40 seconds: More than 40 seconds:
PROGRESS OF LABOUR Oxytocin: Record the amount of oxytocin per volume IV of fluids in drop per minute every 30 minutes when used. drugs given; record any additional drugs given.
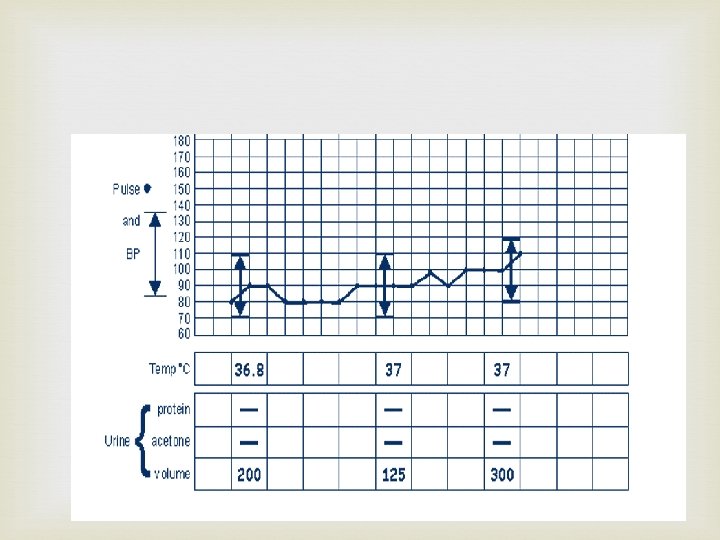
MATERNAL CONDITION Pulse: record every 30 minutes and mark with a dot ( • ) Blood pressure. record every 4 hours and mark with arrows. Temperature: record every 2 hours. Protein, acetone and volume. record every time urine is passed.
CLINICAL RELEVANCE
COMPONENTS OF NORMAL LABOUR PATIENT Pain , bladder empty , dehydration , exhaustion POWERS Uterine contractions Maternal effort PASSAGES Maternal pelvis ( Inlet - Outlet ) Maternal soft tissue PASSENGER Fetal ( size - presentation - position – Moulding) Cord Placenta Membranes
MANAGEMENT OF NORMAL LABOUR USING THE PARTOGRAPH
Do not augment with Oxytocin if active latent and phases go normally Do not intervene unless complications artificial develop rupture of membranes ( ARM ) No ARM in latent phase ARM at any time in active phase
MANAGEMENT OF ABNORMAL PROGRESS OF LABOUR
AT OR BEYOND ACTION LINE Conduct full medical assessment Consider intravenous infusion / bladder catheterization / analgesia Options Deliver by cesarean section if there is fetal distress or obstructed labour Augment with Oxytocin by intravenous infusion if
PROLONGED LATENT PHASE If a woman is admitted in labor in the latent phase ( less than 3 cm dilatation ) and remains in the latent phase for next 8 hours Progress is abnormal and she must be transferred to a hospital for a decision about further action This is why there is a heavy line drawn on the partograph at the end of 8 hours of the latent phase
PROLONGED ACTIVE PHASE In the active phase of labor , plotting of cervical dilatation will normally remain on or to the left of the alert line. But some cases will move to the right of the alert line and this warns that labor may be prolonged This will happen if the rate of cervical dilatation in the active phase of labor is not 1 cm / hour or faster A woman whose cervical dilatation moves to the right of the alert line must be transferred and managed in a hospital with adequate facilities for obstetric intervention unless delivery is near at the action line , the woman must be carefully reassessed for why labor is not progressing and a decision made on further management
SECONDARY ARREST OF CERVICAL DILATATION Abnormal progress of labor may occur in cases with normal progress of cervical dilatation then followed by secondary arrest of dilatation
SECONDARY ARREST OF HEAD DESCANT Abnormal progress of labor may occur with normal progress of descent of the fetal head then followed by secondary arrest of descent of fetal head
POINTS TO REMEMBER It is important to realize that the Partograph is a tool for managing labor progress only The Partograph does not help to identify other risk factors that may have been present before labor started
POINTS TO REMEMBER Only start a partograph when you have checked that there are no complications of pregnancy that require immediate action A partograph chart must only be started when a woman is in labor, Be sure that she is contracting enough to start a partograph If progress of labor is satisfactory , the plotting of cervical dilatation will remain or to the left of the alert line
POINTS TO REMEMBER When labor progress well , the dilatation should not move to the right of the alert line The latent phase. 0 – 3 cm dilatation , is accompanied by gradual shortening of cervix. normally , the latent phase should not last more than 8 hours The active phase , 3 – 10 cm dilatation , should progress at rate of at least 1 cm/hour When admission takes place in the active phase , the admission dilatation, is immediately plotted on the alert line
POINTS TO REMEMBER Dilatation of the cervix is plotted ( recorded with an X , descent of the fetal head is plotted with an O , and uterine contractions are plotted with differential shading Descent of the head should always be assessed by abdominal examination ( by the rule of fifths felt above the pelvic brim ) immediately before doing a vaginal examination Assessing descent of the head assists in detecting progress of labor Increased molding with a high head is a sign of Cephalopelvic disproportion
POINTS TO REMEMBER Vaginal examination should be performed infrequently as this is compatible with safe practice ( once every 4 hours is recommended ) When the woman arrives in the latent phase , time of admission is 0 time A woman whose cervical dilatation moves to the right of the alert line must be transferred and managed in an institution with adequate facilities for obstetric intervention , unless delivery is near
POINTS TO REMEMBER When a woman‘s Partograph reaches the action line , she must be carefully reassessed to determine why there is lack of progress , and a decision must be made on further management ( usually by an obstetrician or resident ) When a woman in labor passes the latent phase in less than 8 hours i. e. , transfers from latent to active phase , the most important feature is to transfer plotting of cervical dilatation to the alert line using the letters TR, Leaving the area between the transferred recording blank. The broken transfer line is not part of the process of labor DO not forget to transfer all other findings vertically
CONTROVERSY OVER INCLUSION OF THE LATENT PHASE Against: the reading of the partograph is simple and easier to use. It increases the chances of unnecessary caesarean section. For: proper management of latent phase has advantages- prevent prolonged labour, fetal and maternal mortality and morbidities.
CONCLUSION. The WHO has endorsed that all labour should be monitor closely by the Partograph. When used appropriately, it improves the management of labour and support decision making regarding interventions
REFERENCES Friedman E. A. (1954) The Graphic Analysis Of Labour. Am. J. Obstetrics and Gynaecology. 68(6); 1568 -1575. Kwawukumen E. Y. , Emuvegan E. E. (eds)(2002) Comprehensive Obstetrics In The Tropics. Asante and Hittscherz Printing Limited, Accra. Philpott R. H. and Castle W. M. (1972), Cervicographs In The Management Of Labour In Primigravida. The Action Line And Treatment Of Abnormal Labour. Journal of Obstetrics and Gynaecology of the British Commonwealth. 79(7): 599 -602. World Health Organisations. (2000) Multicountry Survey on National and Newborn Health