NICE Public Health Briefings Peninsula Public Health Network

NICE Public Health Briefings Peninsula Public Health Network 7 th Annual Conference Stephen Judge, NICE Implementation Consultant Dr Rachel Kettle, NICE Public Health Analyst

The role of NICE • To identify good clinical and public health practice using the best available evidence • To help resolve uncertainty for the public, patients and professionals • To reduce variation in the availability and quality of practice and care. April 2013 – social care guidance and standards

Public Health Briefings TOPIC PUBLICATION Physical activity July 2012 Workplace health July 2012 Tobacco July 2012 Alcohol October 2012 Health inequalities October 2012 NICE guidance and the public health outcomes framework November 2012 Behaviour change January 2013 Walking and cycling January 2013 Obesity March 2013 Contraceptive services TBC Effective partnerships TBC Health equity audit TBC Return on investment TBC

• Introduction • Action planning • Key Messages • Costs and Savings • What can Local • Background to Authorities Achieve • What is Effective • Good practice examples recommendations • • Support from NICE. Other useful resources • Summarise key issues on many public health topics • Suggest effective interventions • Web based, and signpost further information • Intended for audiences less familiar with public health or with NICE • Appeal to others such as CCGs and local public health teams • Written in a way we hope is appealing to readers (don’t worry about ‘proportional universalism’ – there are glossaries !)

What are health inequalities ? • Differences between people due to social, biological or geographical factors • Can result in huge disparity in expectations of long and healthy lives • Some causes, such as ethnicity, are fixed. Others we can tackle. . . • Low ‘social position’ means likely worse health

. . . in a nutshell. . . only those in least deprived circumstances are likely to have any disability-free retirement

Local authorities are well placed to make a difference

What might be achieved ? • The cost in lost taxes and higher welfare payments arising from health inequalities has been estimated in the region of £ 28 -32 billion. • Continuing to reduce smoking prevalence can have significant local impacts, and is very clearly linked to health inequalities, with the more deprived being more likely to smoke and to smoke more heavily. • In Lancashire, halving the health gap between the least deprived fifth and the rest would avoid 1500 premature deaths, gain the population as a whole an extra 1. 3 life years and almost double that (2. 5) in disability free life years- tha gains would be greatest in the deprived • Strategy will need a mixture of both targeted and universal services

Quick Wins ? • Preventing unintentional road injuries in under 15 s e. g. 20 mph speed limit zones • Smoking cessation e. g. access to cessation services (see ROI tool) • Reducing teenage pregnancies e. g. LARC, emergency contraception • Improve the economy by reducing sickness absence – e. g. workplace physical activity programmes – Business case tool for promoting physical activity in the workplace

Acting on Information • Identifying local need is the first step • The Public Health Observatory network provides health inequality data which can help contribute to local JSNA PH 15 Step two is to identify groups and target interventions (see NICE PH 15 identifying and supporting people most at risk of premature death)

Planning services • Always ‘equity proof’ policies and programmes to help identify and address health disparities – even those without an explicit health focus • Equity auditing as part of the JSNA process is recommended • Use health impact assessment to assess the potential health impact of a proposal and mitigate against unintended consequences Using these tools can result in changes to programmes that give: – – equal access for equal need (e. g. increased availability of free fruit in schools with pupils in greater need) equal use for equal need (e. g. increase access to smoking cessation in lower income workplaces) – equality of care (e. g culturally specific maternity services for BME communities) – equal outcomes for equal need (e. g. greater reduction in CHD in more deprived groups)

Equal impact for all A public health intervention where all are affected equally means, everyone’s health state improves equally… BUT The gradient remains the same and health inequality has not changed.

Proportionate universalism A public health intervention where the intensity of effort is signified by the size of the arrow and determined by the needs of the group… The gradient flattens and health inequality has reduced. . AND Everyone in the population has had health gains.

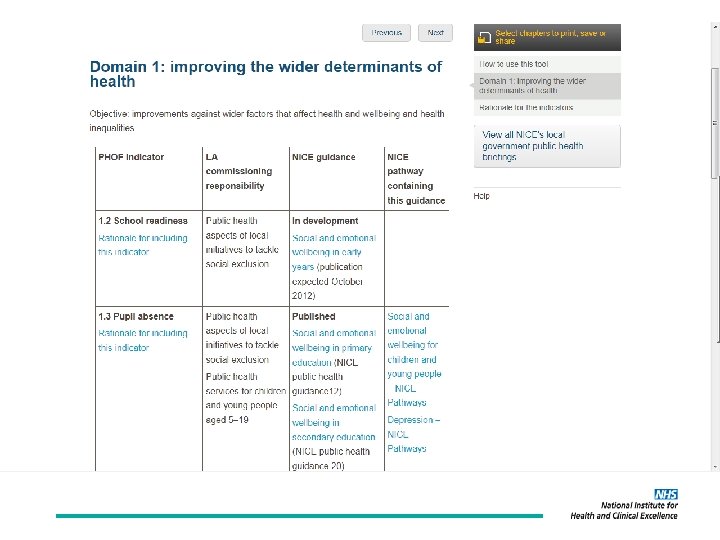
Public Health Outcomes Framework and NICE One of two overarching aims – reduce health inequalities NICE have mapped relevant guidance and standards to the 4 domains of the PHOF NICE guidance; - Is based on the best available evidence - Is compiled by independent experts - Assesses effectiveness and cost effectiveness of interventions

Harmful behaviours? • Alcohol – see NICE Pathway on prevention strategies • Obesity – see ‘physical activity pathway’ where recommendations for workplaces and environmental interventions can be found • Smoking – NICE recommendations tailoring or targeting services for minority ethnic and disadvantaged communities • Unintentional injuries – refer to NICE guidance for preventing accidents in under 15 s by reducing the speed of drivers

Help to see more clearly I cdnoult blveiee taht I cluod aulaclty uesdnatnrd waht I was rdanieg. The phaonmneal pweor of the hmuan mnid, aoccdrnig to rscheearch at a Cmabrigde Uinervtisy, it deosn’t mttaer in waht oredr the ltteers in a wrod are, the olny iprmoatnt tihng is taht the frist and lsat ltteer be in the rghit pclae. The rset can be a taotl mses and you can sitll raed it wouthit a porbelm. Tihs is bcuseae the huamn mnid deos not raed ervey lteter by istlef, but the wrod as a wlohe. Amzaning – and I awlyas tohuthgt slpeling was ipmorantt !

NICE Pathways – set out all that NICE have to say about a particular topic or condition in an easy to navigate graphical format. As well as providing summary information at each ‘node’, they also provide links to the underlying guidance, quality standards and supporting tools. Now optimised for Ipad too ! . Some topics feature summary descriptions of effective interventions – treatments or actions that have been shown to work
 • More people at")
Costs and Savings • The QALY (Quality adjusted life year) • More people at risk and treated – lower QALY • Public Health interventions overwhelmingly suggest the biggest return – albeit you may have to wait a while for the outcome (e. g. obesity) • Savings, or avoided costs, may materialise in different departments, organisations or even sectors – a powerful reason to consider integrated budgeting and commissioning

Quality Adjusted Life Years • • Combines both quantity and health-related quality of life (Qo. L) into a single measure of health gain Qo. L (utility) determined using validated questionnaires Conversion to numerical utility values reflecting preferences over health 1 Health-related quality of life • Initial QALY loss due to side effects New treatment Current treatment QALYs gained 0 Length of life (years)

ROI Tool

. If reading this online, click the links below to download; Guidance app for Apple Guidance app for Android Also available – the app for the British National Formulary BNF app for Android BNF app for Apple

Want to know more ? • Website www. nice. org. uk • Sign up to receive monthly NICE News • NHS Evidence www. evidence. nhs. uk • Email stephen. judge@nice. org. uk

Don’t mention the • Name two interventions you think would make a real impact on reducing inequality • What do you see as the key barriers to introducing those changes ? • What would help to overcome those barriers ? • From what you have heard in this session, how might you utilise NICE’s support ?
- Slides: 26